-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Clinical Medicine and Diagnostics
p-ISSN: 2163-1433 e-ISSN: 2163-1441
2017; 7(1): 23-30
doi:10.5923/j.cmd.20170701.04

Study of B-Type Natriuretic Peptide and Exercise Electrocardiography Test to Predict Silent Myocardial Ischemia in Asymptomatic Egyptian Patients with Type 2 Diabetes Mellitus
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKhaled Massoud Dessouky1, Mahmoud Osama Ahmed1, Abdelaziz Rezk Sheridah2, Kamel Soliman Hammad3, Kamal Hashem Salah3
1Internal Medicine Department, Faculty of Medicine (Boys), Al-Azhar University, Cairo, Egypt
2Cardiology Department, Faculty of Medicine (Boys), Al-Azhar University, Cairo, Egypt
3Clinical Pathology Department, Faculty of Medicine (Boys), Al-Azhar University, Cairo, Egypt
Correspondence to: Khaled Massoud Dessouky, Internal Medicine Department, Faculty of Medicine (Boys), Al-Azhar University, Cairo, Egypt.
| Email: |  |
Copyright © 2017 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

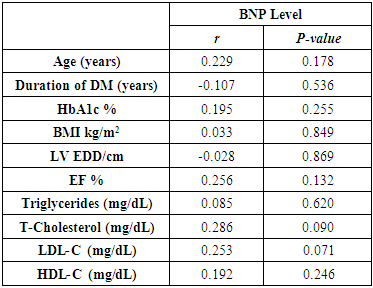
Background: Silent myocardial ischemia (SMI) is more frequent in diabetic patients leading to a delayed diagnosed and more advanced stage of coronary artery disease (CAD) at the time of diagnosis. Different none—invasive tests to determine the presence of CAD by national societies of cardiology and / or diabetology. Exercise electrocardiography (ECG) test can be recommended in first intension if maximal heart rate can be achieved. B-type natriuretic peptide (BNP) is a hormone that is released primarily by ventricular myocyte in response to physiological and pathological stimuli. Aim of this study: was to evaluate BNP in predicting silent myocardial ischemia in asymptomatic Egyptian patients with type 2- diabetes mellitus [T2DM]. Patients: This study was conducted on 50 patients with T2DM. We excluded patients with a history or evidence of heart failure or CAD. Methods: All patients were subjected to: full history taking, complete cardiac examination and routine laboratory investigations in addition to BNP level. Moreover, resting, stress ECG and transthoracic 2D Doppler Echocardiography. Results: 36 out of 50 patients (75%) were found positive for exercise induced ischemia (positive group), while 12 out of 50 patients (25%) were normal exercise ECG test (Normal group) and 2 patients were excluded from the study as they failed to reach 85% of the predicted maximal heart rate for the corresponding age (Inconclusive stress test). Positive group patients were older with longer duration of uncontrolled diabetes mellitus, higher Body Mass Index (BMI) and waist circumference (WC). BNP level was significantly higher in positive group patients compared to normal group (43.5 ± 9.6 pg/ml) vs. (15.43 ±3.91pg/ml (P< 0.000). Receiver operating characteristic curve (ROC- curve) analysis revealed that the BNP level above 22.4 pg /ml predicted silent myocardial ischemia with sensitivity 88.89% and specificity 75%, positive predictive value of 91.4% and negative predictive value of 69.2%. No statistically significant correlation was found between BNP level and each of age, duration of DM, BMI, and HBA1c and lipid profile except total cholesterol in positive group patients. Conclusion: BNP level is of value in predicting silent myocardial ischemia on stress ECG testing in asymptomatic Egyptian patients with T2DM.
Keywords: B-type natriuretic peptide, Stress ECG test, Silent myocardial Ischemia
Cite this paper: Khaled Massoud Dessouky, Mahmoud Osama Ahmed, Abdelaziz Rezk Sheridah, Kamel Soliman Hammad, Kamal Hashem Salah, Study of B-Type Natriuretic Peptide and Exercise Electrocardiography Test to Predict Silent Myocardial Ischemia in Asymptomatic Egyptian Patients with Type 2 Diabetes Mellitus, Clinical Medicine and Diagnostics, Vol. 7 No. 1, 2017, pp. 23-30. doi: 10.5923/j.cmd.20170701.04.
Article Outline
1. Introduction
- The heart is now recognized as an endocrine organ. It released a number of hormones, which belong to the natriuretic peptide family. There are currently four types of natriuretic peptides that have been described as ANP, BNP, CNP, and DNP. ANP and BNP are primarily released from heart [1].In human, BNP is primarily derived from the ventricular myocyte. It has several systemic effects, which counteract CV volume overload including vasodilatation, diuresis, and inhibition of the Renin- Angiotensin- Aldosterone system [2].BNP synthesis is constitutive and its release is triggered by variety of physiological and pathological stimuli including CHF, LV systolic and diastolic dysfunction, Left ventricular hypertrophy (LVH), valvular heart disease, pulmonary, renal diseases and advanced age [3]. The use of BNP in the diagnosis and prognosis of heart failure patient is now well established [4]. However, Evidence point towards a role of BNP in identifying patients with myocardial ischemia and CAD [3].BNP may also help to identify CAD in asymptomatic patients and this particularly important because patients with SMI have a 21 – fold increase risk of coronary event [5]. In addition almost 50% of sudden cardiac death still occurs in people with no documented previous history of overt cardiac disease [6]. Coronary artery disease accounts for 70- 80% of mortalities in patients with T2DM. T2DM is recognized as a CAD risk factor [7]. In patients with T2DM, CAD is generally detected at an advanced stage with extensive atherosclerosis and poor outcomes, whereas CAD is commonly missed in the asymptomatic stage [8]. Thus, there is a clear need to identify patients with T2DM who are at risk for cardiovascular events before the onset of symptoms. About 11 years ago, the American Diabetes Association (ADA) suggested a risk factor-guided screening approach (e.g., considering age, gender, hypertension, and dyslipidemia) for early detection of CAD in asymptomatic patients withT2DM. The ADA also recommends that DM patients perform a treadmill exercise test as early detection of CAD [9].Myocardial ischemia is defined as a transient and reversible decrease in oxygen to myocardium, responsible for the following events: Initially, hemodynamic changes followed by kinetic changes (elevated end-diastolic left ventricular pressure then kinetic changes), then metabolic (lactate production), electric (repolarization changes), and clinic (chest pain). SMI is defined as the presence of objective evidence of myocardial ischemia in the absence of chest discomfort or other anginal equivalents symptoms (e.g., dyspnea, nausea, and diaphoresis). SMI can be detected also using cardiac stress testing. SMI has been defined as exercise-induced ST depression of >1mm in absence of CAD symptoms [10]. Due to its predictive power, exercise ECG has received much attention in recent years. Among asymptomatic patients, those with an abnormal ECG response during exercise have a substantially high risk of developing manifest coronary heart disease than those with a normal ECG response [11].This current study aimed to determine whether BNP can predict silent myocardial ischemia on exercise Stress testing in asymptomatic Egyptian patients with T2DM.
2. Patients and Methods
2.1. Patients
- 50 patients with T2DM were included in this study. They were selected from outpatients DM Clinic of Sayed Galal Al – Azhar university hospital. The study was performed during the period from October 2013 to March 2015. All subjects were informed of the general aim of the study and their participation was fully voluntary and informed written consent was obtained from all subjects pre-enrollment.Inclusion criteria: All patients with T2DM were on regular anti- diabetic therapy either oral or insulin, duration of diabetes more than 10 years. Exclusion criteria: patients suggested to have myocardial ischemia and those known to have CAD or undergone coronary intervention, with evidence of LVH, heart failure, arrhythmia, ejection fraction < 50% on resting transthoracic echocardiography. Patients with serum creatinin >1.2 mg /dL and patients who had parenchymal or pulmonary vascular disease.Methods: All patients included in the study were subjected to the following:1-Comprehensive history taking including cardiac, family history of CAD, medications and other risk factors. Thorough clinical examination including arterial blood pressure systolic and diastolic blood pressure (SBP & DBP), (BMI) was calculated as the weight in kilograms divided by the height in meters squared (Kg/m2) and (WC). WHO cutoff for BMI (30≥kg/m2 was considered obese) was used [12]. Central obesity was considered if WC ≥ 90 cm in men and ≥ 80 cm for women) [13].
2.2. Laboratory Investigations
- All biochemical tests were done by OLYMPUS 7500 AU 2700 ANALYSER, at baseline, in the morning after an overnight fast 12 - 14 hours; 5 ml of venous blood samples were taken from each subject participating in the serum was separated by centrifugation for 15 minutes at 3000xg. The separated serum was stored at -20°C for the measurement of:v BNP test: was measured by enzyme immunoassay technique (Alere Triage BNP test), after exercise ECG test. The reference value of BNP depends on age and gender and is higher in elderly persons and women [14]. v Biochemical parametersHbA1C levels (normal range 4-5.5%) were measured: by using National Glycohemoglobin Standardization Program (NGSP)-certified method and standardized to Diabetes Control and Complication Trial [DCCT] [15]. Serum lipid levels (total cholesterol, triglyceride, HDL-cholesterol) were measured by standard enzymatic spectrophotometric methods, LDL-Cholesterol was calculated from the equation of Friedwald et al., [16] LDL-C (mg/dL) = TC (mg/dL) - HDL-C (mg/dL) - TG/5. Serum creatinine and blood urea were measured by colorimetric method Kinetic UV test.
2.3. Resting Transthoracic 2- D- Doppler Echocardiography
- Echocardiography remains the most frequently used and usually the initial imaging test to evaluate all cardiovascular diseases related to structural, functional, or hemodynamic abnormality of the heart. All patients were examined in left lateral position by experienced cardiologist by using SONO 7500 Philips with 3.5 MHZ probe. All measurements were done according to the recommendation of American Society of Echocardiography. Patients with LVH, valvular heart disease and (EF < 50%) were excluded from the study.
2.4. Resting ECG
- Patients with significant abnormalities on resting ECG like: left bundle branch blocks (LBBB), LVH, atrial fibrillation, ST / T wave abnormalities, significant bradycardia or tachyarrhythmia were excluded.
2.5. Exercise ECG
- Exercise ECG testing is one of the most frequent non-invasive modalities used to assess patients with suspected cardiovascular disease. It is performed according to Bruce protocol and is mainly used to estimate prognosis and determine functional capacity, to assess the probability and extent of coronary disease, and the effect of therapy. It was done by GE Marquette case T 2100. Patients maintained beta blocker, calcium channel blocker; nitrates were instructed to discontinue these medications for 48 hours before the test. The procedure is done after 4 hours fasting. ECG monitoring and heart rate and blood pressure were assessed before and during exercise and recovery period. The duration of the test was noted. The exercise stress test were analysed for the presence of ≥ 1 mm horizontal or down sloping ST segment depression measured at 0.08 seconds after the J point. The American College of Cardiology (ACC)/American Heart Association (AHA) guidelines also specify indications for termination of exercise testing including: drop in systolic blood pressure (SBP) more than 10 mm Hg from baseline or raise in blood pressure (SBP of 250mmHg, DBP higher than 115 mm Hg), Development of new bundle branch block or atrial fibrillation, chest pain, dyspnea, fatigue, dizziness, near syncope, cyanosis, pallor, sustain ventricular tachycardia, ST elevation (> 1mm) in leads without diagnostic Q waves, marked of S-T segments depression (horizontal or down- sloping > 2mm). Interpretation of test finding: Interpretation should include exercise capacity, clinical, hemodynamic and ECG response. The test was considered positive when a horizontal or down-sloping, S-T segment with a depression ≥ 1mm occurred 0.08 second after J point. The test was considered equivocal when a ST segment < 1mm was observed. The test was considered inconclusive if the patients failed to reach 85% of the predicted maximal heart rate for corresponding age [17].
2.6. Statistical Analysis of the Obtained Results [18]
- Results were statistically analysed with statistical package for social science (SPSS) version 21. All data are expressed mean and standard deviation. Student t- test: for testing statistical significant difference between mean values of 2 groups by (P-value) as, P<0.05 significant. Chi - Square test: ficto test for statistical significant relation between different variable and grades in qualitative data (or percentage). The r-test: was used to study the relation between 2 quantitative variables.
3. Results
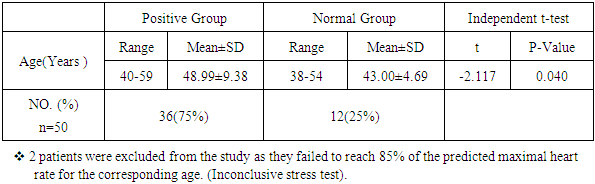
- 50 diabetic [T2DM] normotensive patients were enrolled in this study. The results obtained were tabulated and statistically analysed in tables [1-5].36 out of 50 patients (75%) were positive exercise ECG test for myocardial ischemia (positive Group) while 12 patients (25%) were normal (normal Group) and 2 patients were inconclusive for ischemic heart disease based on exercise testing and excluded from the Study (not age predicted maximal heart Rate (APMHR). The mean age of positive group patients (48.99±9.38.)was significantly higher than that of normal group (43.00±4.69)with a P value of 0.040. (Table 1 & Figure 1).
|
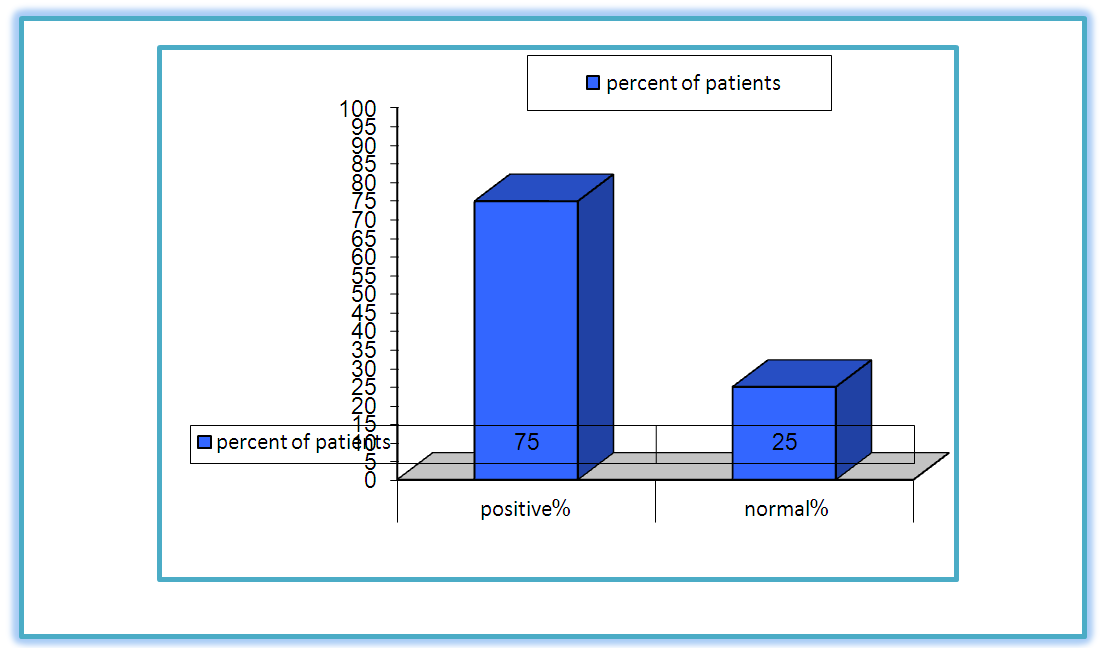 | Figure (1). Percent of myocardial ischemia in studied groups |
|
|

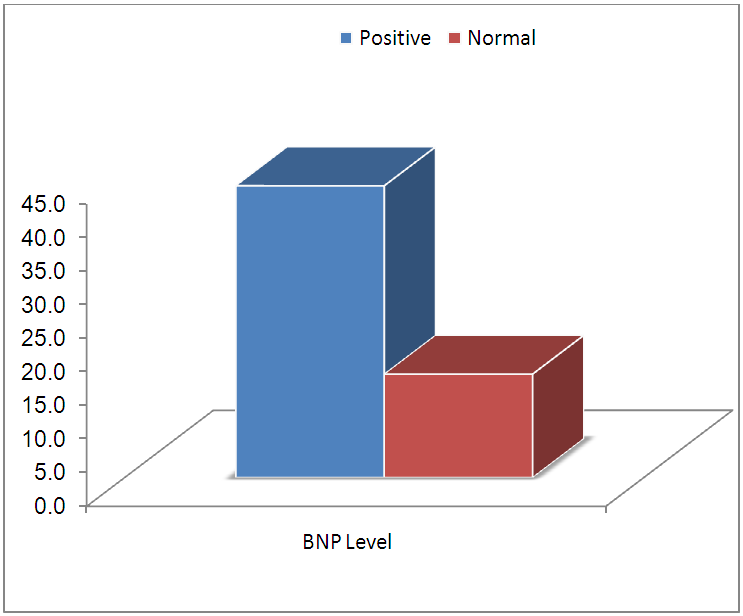 | Figure (2). Comparison between two groups according to BNP level |
|
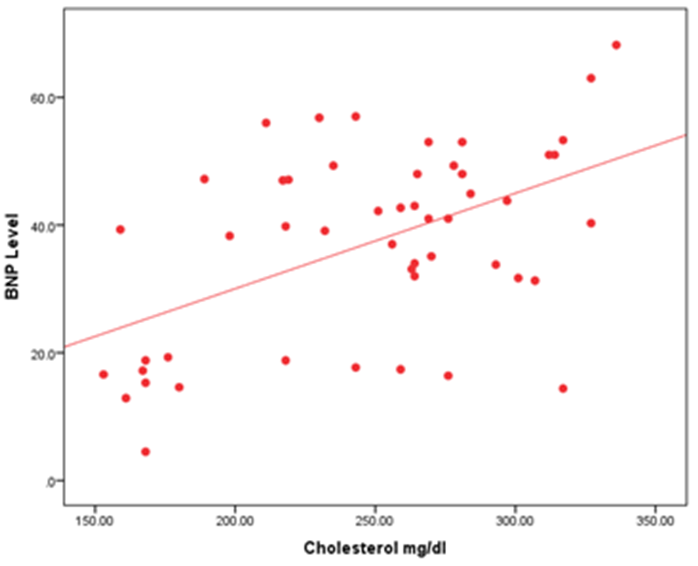 | Figure (3). Show correlation between BNP level and total cholesterol |
|

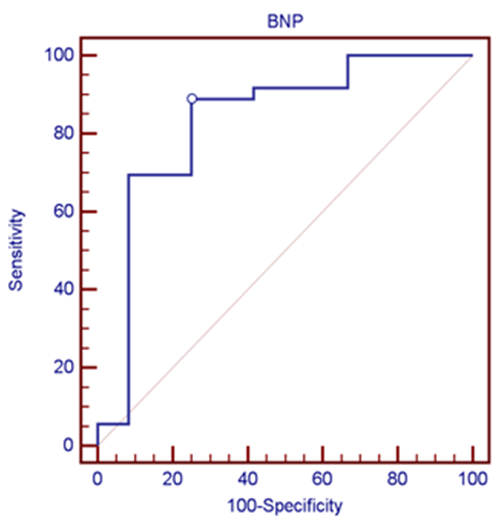 | Figure (4). Receiver operative characteristic (ROC) curve describing the ability of BNP to detect silent myocardial ischemia in patients with no history of ischemic heart disease |
4. Discussion
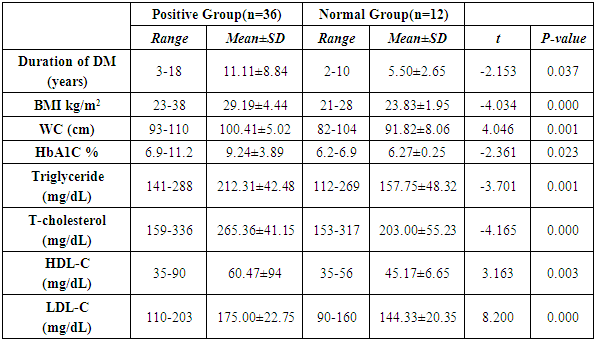
- Diabetic patients have a higher prevalence of SMI and unrecognized myocardial infarction than patients without diabetes. Patients with diabetes and SMI have a very poor prognosis, as reflected by adverse cardiac events or death. The prevalence of silent CAD is 6% to 23% in low risk diabetic patients. In high risk diabetic patients, the prevalence may be high as 60%. So early detection of silent ischemia is important in diabetics [19].This work was planned to determine whether circulating levels of BNP are associated with inducible myocardial ischemia, we measured resting BNP levels immediately after exercise ECG test and suggest cut- off level of BNP that may be appropriate for myocardial ischemia in asymptomatic Egyptian patients with T2DM.In the present study, the incidence of silent ischemia in patients with T2DM detected by exercise ECG test was 75% [36/50] patients [Table 1 & Figure 1]. This result was in agreement with that documented by Scognamiglio et al. [20], Kumar and Singh [11] and Wackers et al., [21] they found 60%, 23.6% and 22% respectively had myocardial ischemia by exercise ECG in T2DM. This wide range in the incidence may be related to patient’s number, selection and risk factors.The major risk factors for coronary artery diseases identified by the Framingham Risk Score include T2DM, total cholesterol, HDL-cholesterol, age and sex [19]. Advanced age was associated with a higher incidence of inducible ischemia among our patients. [Table 1 & Figure 1] This supported by several studies on patients with T2DM over the age of 60 years old [21, 22]. Diabetic dyslipidemia further contributes to atherosclerotic risk, which is mainly due to increased LDL and decreased HDL. In this study , we found increased levels of triglycerides , LDL-cholesterol and total cholesterol were significantly associated with silent ischemia, this supported by the study done by Lavekar and Salkar [23] that found Statistically significant association between increased TG levels, increased TC levels and decreased HDL levels with coronary arterial disease. However, some contradicting results were obtained from the Detection of silent myocardial Ischemia in Asymptomatic Diabetics [DIAD] study and several others showing that there is hardly any association of dyslipidemia with silent ischemia [21].The duration of diabetes is not included among CAD risk factors according to ADA recommendations. However, there are several studies reporting positive correlation between the two [24]. Our study supports the finding that duration of diabetes is a strong predictor of CAD [Table 2]. There are studies recommending routine screening for IHD with exercise ECG test for patients who are suffering from T2DM for more than 10 years [23, 24]. Measurement of HbA1c has been widely used to evaluate glycemic control in patients with diabetes. In the current study, it was revealed that poor glycemic control and silent ischemia are significantly associated with each other. [Table 2] This was in agreement with Eltahwawy et al., [25] they found a significant association between incidence of silent ischemia and HbA1C levels, reflecting the importance of achieving and maintaining euglycemia. However, in this study, we found increased BMI and WC were significantly associated with silent myocardial ischemia .this supported by the work of Sargin et al., [26] suggested that obesity may represent the risk factor of CAD in patients with T2 DM. BNP may help to identify CAD In asymptomatic patients and this is particularly important because patients with SMI have a 21 –fold increase risk of coronary event [5]. In addition almost 50% of sudden cardiac death still occurs in people with no documented previous history of overt cardiac disease [6]. For this purpose the first necessary step would be able to develop a simple test which is able to identify those patients with diabetes with silent coronary artery disease. In the present study, we found increased BNP level was a valuable predictor of silent myocardial ischemia evaluated by exercise ECG in patients with T2DM irrespective of age, duration of DM, glycemic control, BMI, WC and lipid profile except TC. [Tables 3 & 4 & figure 2 & 3] This was in agreement with results of studies done by Babes et al., [27] & Hamano et al., [28], Cosson et al., [29] and Rana et al., [30] they found that increased levels of BNP were independently associated with silent myocardial ischemia in patients with T2DM. Our result demonstrated that A cut –off BNP value above 22.4 pg/ml had sensitivity 88.89% and specificity 75% for detecting silent myocardial ischemia with positive predictive value of 91.4% and a negative predictive value of 69.2% in T2DM Egyptian patients [table 5 & figure 4]. This result was in accordance with that concluded by Rana et al., [30] who reported that BNP above 20 pg / ml with sensitivity and specificity for detection of positive exercise test were 87% and 37% respectively, and BNP value above 35 pg /ml the sensitivity 69% and specificity 72%. and for BNP value above 40 pg /ml sensitivity was 63% and specificity 81%.
5. Conclusions
- Silent myocardial ischemia was found in 75% of patients with T2DM. The risk for SMI in type 2 diabetes increased with old age, long duration of diabetes, poor glycemic control as well as obesity and dyslipidemia. BNP was a valuable predictor of silent myocardial ischemia detected by exercise ECG in Egyptian patients with T2DM. The risk associated with BNP elevation was independent of confounding variables including: advanced age, duration of diabetes, glycemic control and dyslipidemia except total cholesterol. Thus elevated BNP is a strong predictor for myocardial ischemia.
6. Recommendations
- On basis of these data, we hope that future studies on large population are needed for more evaluation the diagnostic accuracy of serum BNP as an acceptable substitute of exercise stress testing for diagnosis of silent myocardial ischemia and to see different cut off for BNP can perform better in different groups of patients. Routine screening for SMI is advised in T2DM especially if they have other risk factors. The most recommended technique used for screening coronary artery disease in these patients is myocardial perfusion scintigraphy or stress echocardiography because of greater sensitivity and specificity in relation to the exercise ECG test.