-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Clinical Medicine and Diagnostics
p-ISSN: 2163-1433 e-ISSN: 2163-1441
2016; 6(5): 122-125
doi:10.5923/j.cmd.20160605.02

A Comparative Study of Marginal Fit between IPS e.max Press Crown and Endocrown after Cementation (In Vitro)
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLRana Dalloul, Jihad Abou Nassar, Nabil Al-Houri
Department of fixed prosthetic, Faculty of Dentistry, Damascus, Syria
Correspondence to: Rana Dalloul, Department of fixed prosthetic, Faculty of Dentistry, Damascus, Syria.
| Email: |  |
Copyright © 2016 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The aim of this study was to evaluate the marginal fit of two types of IPS e.max Press crowns after cementation (conventional crown and Endocrown) in vitro. Twenty extracted permanent first and second mandibular molar teeth, were collected. The proximal walls were cut 1 mm above the cementoenemal junction and the endodontic treatments were performed. The molar teeth were randomly divided into two groups. The first group (n= 10) was restored with composite core and prepared to receive IPS e.max Press conventional crown (C). The second group (n=10) was prepared to receive IPS e.max Press Endocrown (E). All crowns were cemented by dual cure resin cement then the marginal fit evaluated under stereo microscope by measuring 13 random points at marginal-edge of the buccal, lingual, mesial and distal sides of the crown. Statistical analysis was accomplished with t-student test and significance was predetermined at p<0.05. The mean marginal fit in group E (34.38µm±3.23) was that in group C (47.08 µm ±SD4.96) P=0.000. The mean marginal fit of proximal surfaces in group E (Mesial 22.08 µm±4.43 and Distal 21.54 µm±3.16), was significantly less than that of Buccal and Lingual surfaces (46.15 µm±8.18, 47.77 µm±9.87) respectively P=0.000. Within the limits of this study, it can be concluded that the marginal fit of Endocrown was better than that of the conventional crowns.
Keywords: Endocrown, Marginal fit, IPS e.max Press crown
Cite this paper: Rana Dalloul, Jihad Abou Nassar, Nabil Al-Houri, A Comparative Study of Marginal Fit between IPS e.max Press Crown and Endocrown after Cementation (In Vitro), Clinical Medicine and Diagnostics, Vol. 6 No. 5, 2016, pp. 122-125. doi: 10.5923/j.cmd.20160605.02.
Article Outline
1. Introduction
- The good marginal fit seems to be one of the most important technical factors for the long-term success of crowns [1]. Increased marginal discrepancies expose the luting material to the oral environment, thus leading to cement dissolution and microleakage. The cement seal becomes weak, permits the percolation of bacteria, and can cause inflammation of the vital pulp. The in-vivo studies have provided evidence that a large marginal discrepancy in a fixed restoration correlates with a higher plaque index and reduced periodontal conditions [2]. Minimal marginal gaps result in less gingival irritation, cement dissolution, recurrent caries and marginal discoloration [3, 4]. All ceramic materials are widely used in dentistry for restoring anterior and posterior teeth to provide a metal-free structure and esthetic appearance [5, 6]. IPS e.max Press (Ivoclar Vivadent) was introduced in 2005 as an improved press-ceramic material compared to IPS Empress II (Ivoclar Vivadent). It also consists of a lithium-disilicate pressed glass ceramic, but its physical properties and translucency are improved [7]. The heat-pressing technique can be used for the fabrication of copings or full anatomy crown and is based on the lost-wax technique. Prefabricated ceramic ingots of lithium-disilicate are heated and then pressed into the lost-wax form of the full crown [8].Ceramic monoblock technique for broken down teeth was described for the first time by Pissis [9] in 1995. Later Bindl and Mörmann [10] named this restorative procedure “Endocrown” in 1999. The Endocrown is a total porcelain crown fixed to a pulpless posterior tooth, which is anchored to the internal portion of the pulp chamber and to the cavity margins, thus obtaining macro mechanical retention provided by the pulpal walls, and micro retention by using adhesive cementation [11, 12].There were no previous studies evaluated the marginal fit of Endocrown in vitro. Types of finish lines [5, 13] ceramic manufacturing technique [14-16] and fracture resistance [17-19] are the factors that have been investigated for all-ceramic crowns in vitro. The purpose of this study was to compare the marginal fit between two types of Ips e.max Press crowns (conventional crown and Endocrown).
2. Methods and Materials
2.1. Preparation of the Sample
- Twenty extracted permanent first and second mandibular molars were randomly divided into two groups (C and E groups). Mesial and distal surfaces of all specimens were removed to 1 mm above the cementoenamel junction(CEJ). In conventional crown group(C) (n =10), molar teeth were restored with composite cores and prepared to receive Ips e.max Press crown. Wide circumferential deep chamfer margin (0.8mm) was prepared at the CEJ, and 1.5 mm were cut from the axial walls, and 2 mm from the occlusal surface of the composite core restoration. In Endocrown group(E) (n =10), molar teeth were prepared to receive Ips e.max Press Endocrown. The “Endo” preparation was performed by making a circular butt margin with a central retention cavity with rounded internal line angles. Wide circumferential deep chamfer (o.8 mm) was prepared at the CEJ, and 1.5mm were cut from the axial walls, and 2 mm from the occlusal surface of the tooth. Impressions were made with two-step technique with putty and light condensation silicone (Putty and Light Body, Zetaplus, Oranwash L, Zhermack, Italy). They were then casted by gypsum IV to get the dies for fabricating the IPS e.max Press crowns using lost wax technique. All crowns were cemented by dual cure resin cement (Metacem, META BIOMED, Dual Cure).
2.2. Measurement of Marginal Fit
- Marginal fit were evaluated under stereo microscope (Olympus Optical CO. LTD, Tokyo, Japan) (Figure 1) by measuring 13 random points at marginal-edge at buccal, lingual, mesial and distal sides of the crown which calculated 52 points for whole crown (Figure 2). Statistical analysis were accomplished with t- student test and significance was predetermined at p<0.05.
 | Figure 1. Stereo Microscope |
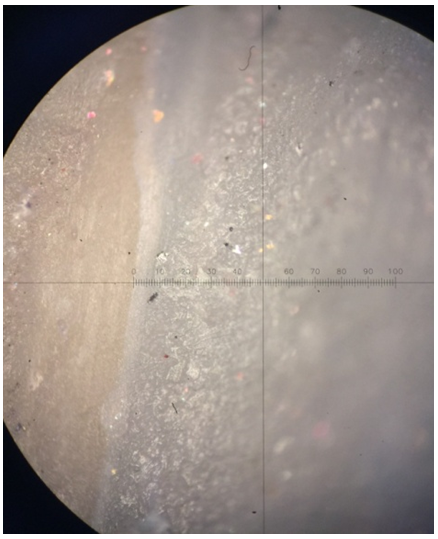 | Figure 2. Fifty micrometer marginal fit under stereo microscope X 10 |
2.3. Results
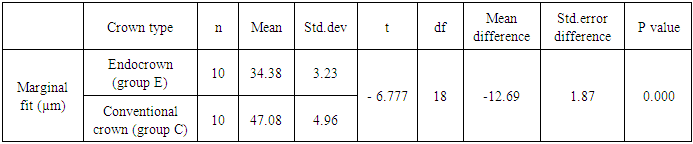
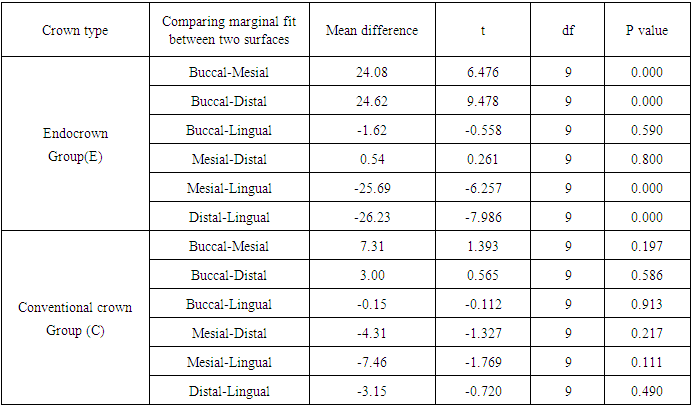
- In general the mean marginal fit values of Endocrown group (34.38µm ± 3.23) was significantly less than that in conventional crown group (47.08 µm ± 4.96), P=0.000. (Table 1).
|
|
|
2.4. Discussion
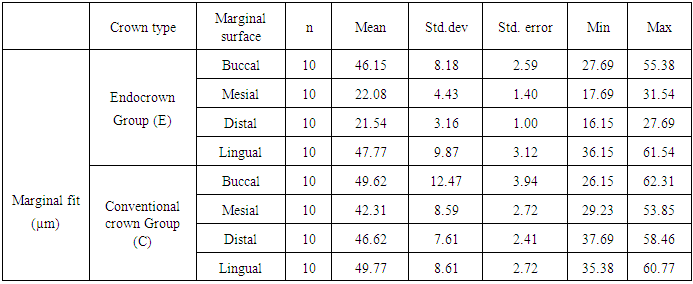
- Endocrown as a relatively new technique had a few studies evaluating it. Some of them were in vivo [10, 20, 21], where the clinincal performance of the Endocrown were evaluated. Others were in vitro [17-19] and were limited by testing the fracture resistance of the Endocrown. To our knowledge, no study so fare evaluated the marginal fit of Endocrown in vitro, where measurements can be obtained more accurately using the stereo microscope. This allow reading the marginal gaps of all surfaces including mesial and distal surfaces which are hard to asses in the vivo studies. Thirteen random points were measured at marginal-edge at the buccal, lingual, mesial and distal sides of the crown accounting for 52 points for each crown as recommended by Groten et al [22] to achieve an accurate result that could be compared with clinical studies. Moldovan et al [23]. rated the values of 100µm for marginal misfit as good, and the values of 200–300 µm as acceptable. Therefore, the marginal accuracies, represented by the absolute marginal discrepancy and measured in the present study, can be rated as good for both groups. However, most studies continue to use the criteria established by McLean and Von-Fraunhofer [24] for evaluating a clinically acceptable maximum marginal gap width. Considering this, both groups had clinically accepted marginal fit which is less than 120 µm. The overall mean marginal fit of the Endocrown Group (34.38µm ± 3.23) was significantly less than that of the conventional crown group (47.08 µm ± 4.96), P=0.000. Moreover, mesial and distal surfaces in Endocrown group had the lowest mean marginal fit (22.08µm ± 4.43, 21.54µm ± 3.16) respectively. This may be secondary to the rounded shoulder finish line in the proximal surfaces in the Endocrown group, whereas it was deep chamfer in all surfaces in the conventional crown group. This corresponds with Cho et al study where they investigated the marginal fit of two crown types (Ceramic optimized polymer (Ceromer) and fiber-reinforced composite (FRC)). They found that shoulder finish line had better marginal fit than chamfer finish line (P<.001) [25].In this study the mean marginal fit of conventional crown group was close to that of Neves et al study, where the mean marginal fit of Ips e.max Press crowns was (36.8 μm ±13.9) [26]. It was also close to Farid et al study, where the marginal fit of 0.8 mm Ips e.max coping was ( 40.5 µm±SD 1.7) and (41.3 µm±SD 2.0) for 1mm Ips e.max coping [27].
3. Conclusions
- Within the limits of this study, it can be concluded that the marginal fit of Endocrown was better than that of the conventional crown. Thus better chance of success when crowning endodontially treated teeth. However, clinical studies are needed to confirm this finding.