-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Clinical Medicine and Diagnostics
p-ISSN: 2163-1433 e-ISSN: 2163-1441
2015; 5(1): 4-7
doi:10.5923/j.cmd.20150501.02
Robertsonian Translocation in a Down Syndrome: A Case Report
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLBandopadhyay Debasis, Bhatnagar Rajan
Dept of Anatomy, Armed Forces Medical College, Pune, India
Correspondence to: Bandopadhyay Debasis, Dept of Anatomy, Armed Forces Medical College, Pune, India.
| Email: |  |
Copyright © 2015 Scientific & Academic Publishing. All Rights Reserved.
Background: Down syndrome also known as Trisomy 21 is a genetic disorder associated with presence of whole or part of third copy of chromosome 21. It is typically associated with characteristic facial features with varying degree of intellectual disability. The frequency of Down syndrome in Indian population is roughly estimated at 1 in every 920 live births. Almost 90% of Down Syndrome are due to pure trisomy 21, 6-7% are of mosaic types (with both normal and trisomy cells) and 3-4% are due to translocation of chromosome 21 to other acrocentric chromosomes. Casereport:We report a 1year old girl born with congenital cardiac anomalies and typical facial features suggestive of Down syndrome like small chin, upward slanting eyes and flat nasal bridge. 5ml of venous blood was cultured for leucocytes and subsequently karyotyped using standard protocol of Trypsin Giemsa banding. Cytogenetic analysis of peripheral blood revealed Down Syndrome with unbalanced Robertsonian translocation between chromosomes 14 and 21 with 3 copies of long arm of chromosome 21. The karyotype revealed 46,XX,rob(14;21)(q10;q10),+21. The carrier status for balanced translocations for both parents were identified by peripheral blood karyotype and was found to be have normal karyotype. Conclusions: Translocation in Down syndrome is usually of Robertsonian type with fusion of chromosome 21 to D or G group chromosome. Most frequent forms are t(14;21) and t(21;21). The occurrence of translocations is either sporadic or secondary if one of the parents is carrier of a balanced translocation. Most translocation Down Syndrome cases are born to young mothers less than 25 years of age when compared with pure trisomy 21 cases. The carrier status of both parents must be established to determine the probability of recurrence of Down syndrome in the next child. Thus parental karyotype, parental ages and family history together help to provide estimation of risk for the next conception.
Keywords: Down syndrome, Robertsonian translocation, Mosaic, Karyotyped
Cite this paper: Bandopadhyay Debasis, Bhatnagar Rajan, Robertsonian Translocation in a Down Syndrome: A Case Report, Clinical Medicine and Diagnostics, Vol. 5 No. 1, 2015, pp. 4-7. doi: 10.5923/j.cmd.20150501.02.
1. Introduction
- Down syndrome also known as Trisomy 21 is a genetic disorder associated with presence of whole or part of third copy of chromosome 21. It is typically associated with characteristic facial features with varying degree of intellectual disability. About half of all affected children are born with a heart defect. The incidence of trisomy is influenced by advancing maternal age and differs between populations (varying between 1 in 300 to 1 in 1000 live births) [1]. The frequency of Down syndrome in Indian population is roughly estimated at 1 in every 920 live births with an annual incidence of 18,000 cases [2]. Almost 90% are due to pure trisomy of the 21st chromosome. About 6-7% of the Down syndrome cases show mosaic cell lines with varying percentage of normal and trisomy cells. A small proportion of approximately 3-5% is due to unbalanced chromosomal translocation involving the acrocentric groups of chromosomes especially chromosomes 14 and 21 [3]. Robertsonian translocations occur during gametogenesis due to non dysjunction at mitosis or meiosis [4]. The occurrence of translocations is either sporadic or secondary if one of the parents is carrier of a balanced translocation. The carrier status of both parents must be established to determine the probability of recurrence of Down syndrome in the next child. About half of the translocation Down syndrome cases are inherited and hence close relatives will have higher chances of carrying the translocation thereby producing affected babies [3]. Thus close relatives must also be advised to get karyotype done to detect carrier status for balanced translocations before conceiving. In our study no further molecular analysis was done to establish the parental origin of the re-arrangements. As per recent advances the extra copy of Hsa21 gene is proposed to result in increased levels of expression of many genes encoded in chromosome 21 thereby producing varying degrees of Down Syndrome phenotypes [5]. However such gene expression profile and correlation with Down Syndrome phenotypes was beyond the scope of our study. Further genomic association studies will point to the genes responsible for the pathology.
2. Case Report
- We report a 1 year old girl child born to young father and mother from Uttar Pradesh, India of age 29 and 24 years respectively. The couple was married since 2009 with history of one live birth healthy girl by Lower Segment Caesarean Section (indication? Cord prolapsed) in 2011 and a history of first trimester (08 wks) elective abortion by MTP in 2012. The mother was a booked case under antenatal care with normal Level I and II USG reports for the third pregnancy. The baby was born at term by normal delivery in Aug 2013. The baby was soon detected to have poor oxygenation status following which investigations revealed congenital heart disease. The face had dysmorphic features like small chin, upward slanting eyes and flat nasal bridge suggestive of Down Syndrome. There was no history of similar illness in babies of close relatives. At the time of referral to our lab the girl was 1 year of age and weighed 9 kgs. She had delayed developmental milestones in terms of motor and social development. She was also advised an immediate surgery for sub-aortic ventricular septal defect. At first we collected 5ml of venous blood of the child in a heparanized syringe. Under aseptic conditions about 1ml of buffy coat of plasma rich in lymphocytes was planted in the culture medium PB Max solution and grown for 70 h at 37ºC in a CO2 incubator. Two separate cultures were set, one in culture vial and another in centrifuge tube. The cells were then arrested at metaphase using 0.1ml colcemid (10µgm/ml) by process called harvesting. After 2h the cultures were subjected to centrifugation at 1000rpm for 10min, the supernatant was discarded and 5ml hypotonic solution (0.56% KCL) was added in each vial/tube. This mixture was incubated at 37ºC for 40 min followed by prefixation with 2-3 drops of Carnoy’s Fixative (3:1 proportion of Methanol and Acetic acid) and centrifugation at 1000rpm for 10 mins. The supernatant was discarded and 5ml of freshly prepared fixative was added to each vial/tube and kept overnight in a refrigerator at 4ºC. Next morning repeated washes were given with Carnoy’s fixative till the cell pellet was white. These cells were then dropped on the slides and allowed to dry over uniform moist heat. Thereafter the slides were placed on stands overnight at room temperature for the process of aging. The slides were then treated with Trypsin and subsequently stained with Giemsa stain for G-Banding. The metaphase spreads were viewed under oil immersion at 100X and at least 20 good spreads were captured for karyotyping using an image analyzer (Cytovision Imaging software).The karyotype analysis detected unbalanced Robertsonian translocation of chromosomes 14 and 21 with trisomy for the long arm of chromosome 21. All the cells showed 46, XX, rob(14;21)(q10;q10),+21 karyotype in the girl child (Fig 1).
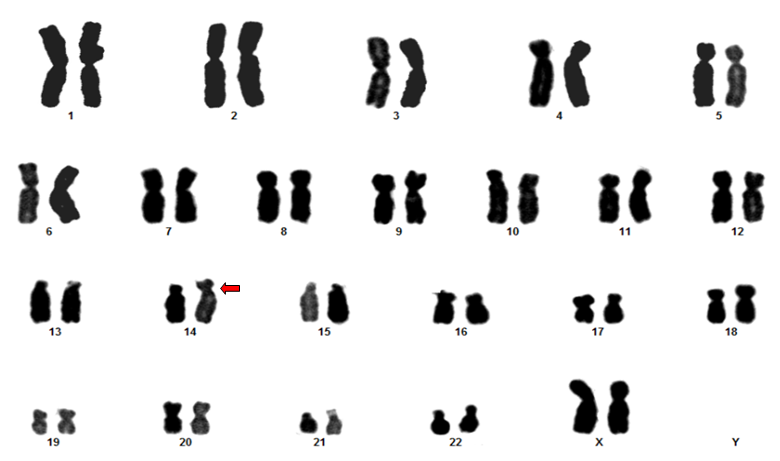 | Figure 1. 46,XX,rob(14;21)(q10;q10),+21 karyotype of the girl child |
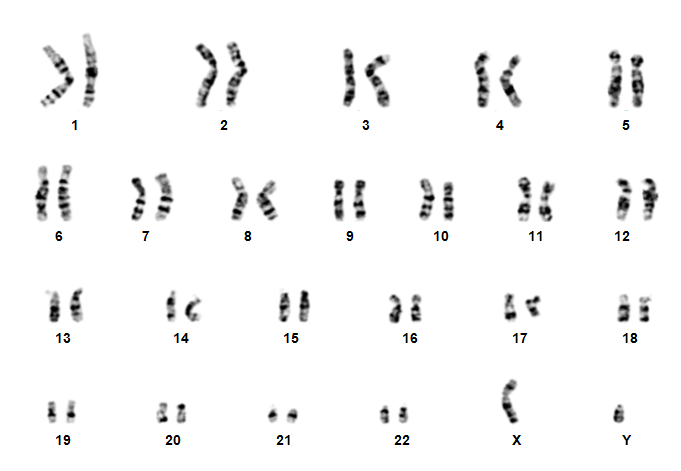 | Figure 2. Normal male karyotype of the father |
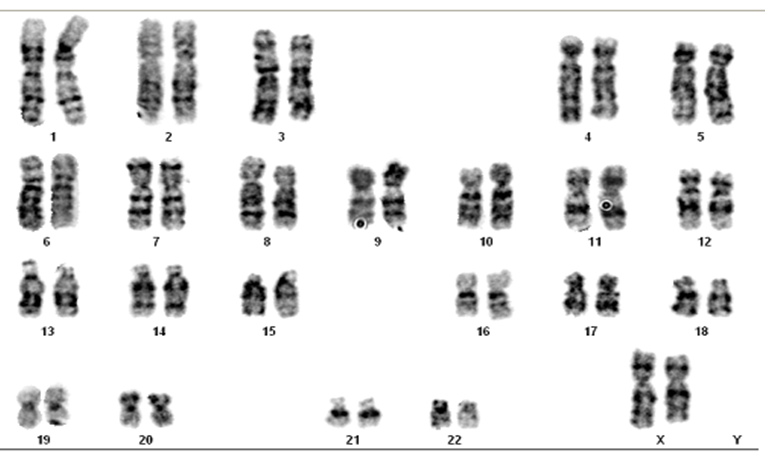 | Figure 3. Normal female karyotype of the mother |
3. Discussion
- The incidence of Down Syndrome in India is 1-2 per 1000 live births [1]. As early as 1959 Legune and co-workers reported an extra chromosome 21 and suggested a chromosomal basis to this disorder [6]. Almost 90% are due to non dysjunction during gametogenesis resulting in classical trisomy 21 of the newborn while rest are due to mosaicism and translocation. The translocation is generally of Robertsonian type involving chromosome 21 and other acrocentric chromosomes and account for 5-6% of the Down Syndrome cases [7]. The most frequent forms of Robertsonian translocations involve the acrocentric groups of chromosomes and occur when the long arms of two acrocentric chromosomes fuse at the centromere while the two short arms get lost [8]. When such translocation takes place between 14/21 or 21/22 chromosomes the translocation may be balanced in either parents showing no phenotypic changes. Such a parent is a balanced translocation carrier. The babies born to such parent may however show an unbalanced translocation between 14/21 or 21/22 resulting in 3 copies of chromosome 21 thereby expressing Down phenotype. Sporadic translocation occurs when part of chromosome 21 breaks off during cell division and attaches to another chromosome, at or prior to conception. Familial translocation occurs when one parent is a balanced translocation carrier. The heterozygous carrier is phenotypically normal though the total number of chromosomes may be 45 as he has all the genes but the child may be born with unbalanced translocation with an extra copy of 21 chromosome [9]. The recurrence rate is higher depending on parental origin. If the mother is a carrier of balanced translocation the recurrence rate is three times higher than father being a carrier [10].Our patient was a 1year old girl child born to young parents of 29 yrs (father) and 24 yrs (mother). There was a history of one live birth of healthy girl child in 2011 by LSCS (indication cord prolapse) and one elective MTP at 8 weeks in 2012 (indication planned parenthood). At the time of 3rd pregnancy during antenatal checkups the Level I and II USG Pelvis detected no abnormality. The baby was a full term normal delivery. The baby showed respiratory distress and poor oxygen saturation soon after birth for which echo cardiogram was done and found to have sub-aortic VSD. The face also showed dysmorphic features like small chin, upward slanting eyes and flat nasal bridge suggestive of Down Syndrome. The child was treated symptomatically and advised surgery for repair of septal defect at a later stage. She reported to us for karyotype analysis at 1yr of age. Cytogenetic examination revealed unbalanced Robertsonian translocation between chromosome 14 and 21 resulting in trisomy for the long arm of chromosome 21. Since the mother was young and the baby had an unbalanced translocation involving 14 and 21 chromosomes both the parents were advised peripheral blood karyotype to verify their balanced transloction carrier status to rule out familial disposition. Both of them were found to have normal karyotype. Hence ours was a case of sporadic translocation and future pregnancies were unlikely to have a higher recurrence rate. It is known that majority of de novo Robertsonian translocations are formed during maternal meiosis [11]. The parental origin can be determined by PCR analysis using polymorphic markers on somatic cell hybrids. In our case no molecular analysis was carried out to determine the parental origin of the translocation. The recent advances suggest Hsa21 gene expression variation being responsible for the varied phenotypes of Down syndrome. Over-expression of Hsa21 gene has been directly implicated for learning disabilities. Gene expression can be assayed using quantitative and qualitative real-time polymerase chain reaction. However such gene expression analysis studies was beyond the scope of our study.
4. Conclusions
- Down syndrome is caused by trisomy of chromosome 21. Though more than 90% of the cases show free trisomy about 5-6% exhibit Robertsonian translocation. While free trisomy is attributed to rising maternal age the Robertsonian translocation is seen in young mothers. It may be sporadic or familial. In familial cases one of the parents is a carrier of balanced translocation. If such translocations are seen in the mother the recurrence rate of an unbalanced trisomy child is much higher compared to translocations of paternal origin. In familial cases of Robertsonian translocation close relatives should also be investigated for balanced carrier translocation status.