-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Clinical Medicine and Diagnostics
p-ISSN: 2163-1433 e-ISSN: 2163-1441
2012; 2(3): 6-8
doi: 10.5923/j.cmd.20120203.02
A Rare Cause of Complete Atrioventricular Block: Lyme Carditis
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-Text HTML
Full-Text HTMLMesut Aydin 1, Serkan Bulur 1, Yasin Turker 1, Kezban Ozmen Suner 2, Ahmet Sahin 3, Hakan Ozhan 1
1Düzce Medical School Department of Cardiology, Duzce University, 81620 Konuralp, Düzce, Turkey
2Duzce Medical School, Department of Chest Disease, Duzce University, 81620 Konuralp, Düzce, Turkey
3Duzce Medical School, Department of Infectious Disease, Duzce University, 81620 Konuralp, Düzce, Turkey
Correspondence to: Mesut Aydin , Düzce Medical School Department of Cardiology, Duzce University, 81620 Konuralp, Düzce, Turkey.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
Lyme disease is a tick-borne spirochete infection that may affect the heart. Cardiac manifestations include conduction disturbances and other pathologies of the heart. Disturbance of atrioventricular (AV) node conduction is the most common cardiac manifestation of Lyme disease. We report a 61-year old female, who was admitted to the emergency department with the complaints of syncope, dizziness and generalized fatigue. Physical examination revealed normal findings. The patient’s electrocardiogram on admission revealed a newly diagnosed bradycardia due to third degree of AV block with40/min ventricular rate. The patient was admitted to the coronary care unit and was placed a transvenous pacemaker. Lyme serology and Western blot were positive for Borrelia antibodies. The symptoms and AV block resolved completely after doxycycline therapy.
Keywords: Tick, Lyme Disease, Lymecarditis, Atrioventricular Block
1. Introduction
- Lyme borreliosis is a tick-borne disease that is known to affect primarily the skin, heart, nervous system, and joints. Generally, cardiac complications occur in the earlydisseminated phase. Disturbance of atrioventricular (AV) nodal conduction is the most common cardiac manifestation of Lyme disease. In this report, a patient with complete AV block caused by Lyme disease was presented and relevant literature also was reviewed.
2. Case Presentation
- A 61-year-old woman without history of cardiovascular diseases was admitted to the emergency department with complaints of syncope, dizziness and generalized fatigue. The pulse was 40 beats per minute and blood pressure was 90/60 mmHg. There were no abnormal findings other than a slight redness in the right upper arm on physical examination. She also did not use any drugs or medication and no history of tick bite. The patient’s ECG revealed third degree AV block (Figure 1).
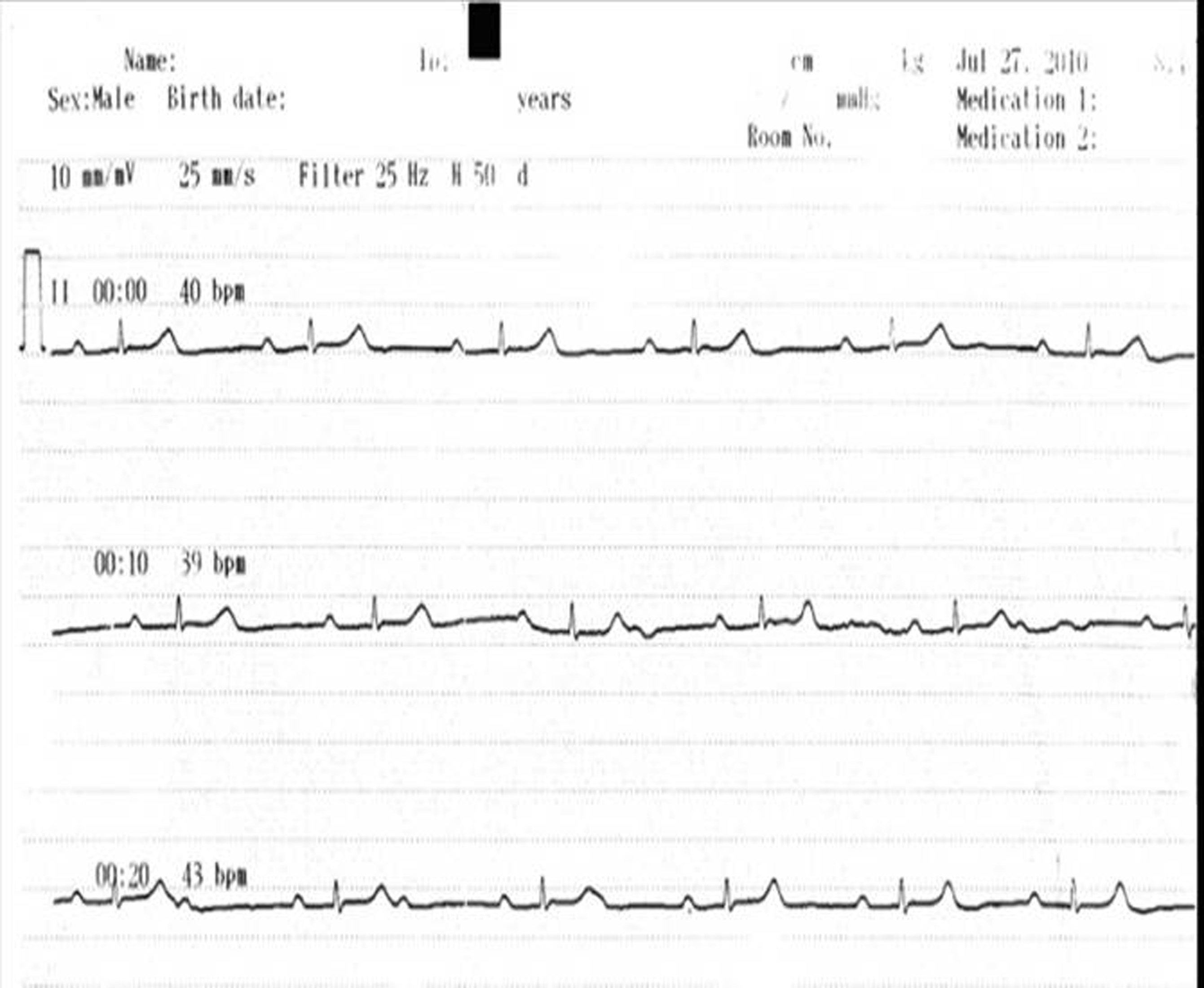 | Figure 1. ECG on admission showing third degree AV block |
|
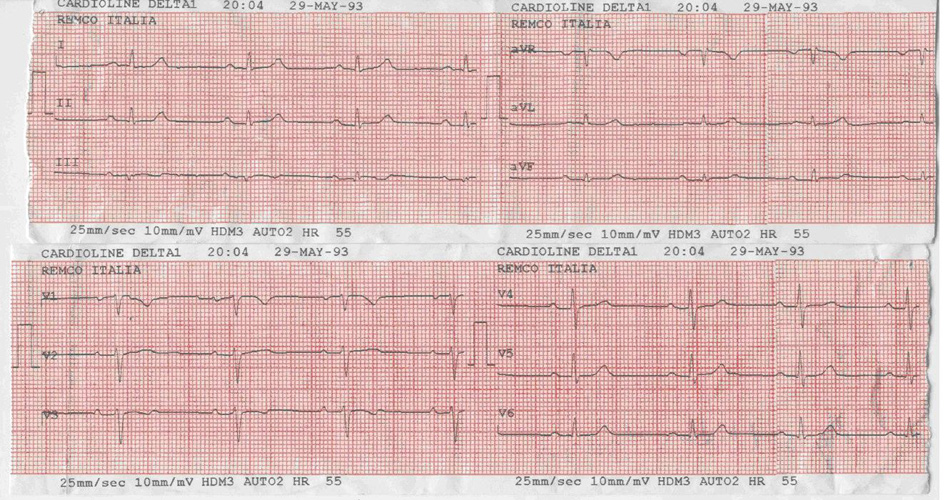 | Figure 2. ECG after treatment with restored sinus rhythm |
3.Discussion
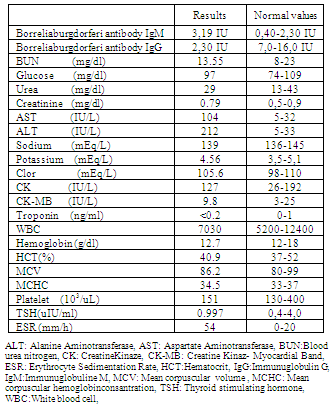
- Lyme Borreliosis (LB) have been reported after 1990’s in Turkey and the spirochete was isolated from the tick vectors[1]. Lyme carditis is a rare manifestation of the disease. It occurs in 1.5%-10% of cases in North America and 0.5%-4% in Europe[2]. There are various symptoms of acute cardiac involvementsuch as exertionaldyspnea, chest pain, palpitation and syncope with a reported rate of 4-10% in patients who have Lyme disease[3,4].The most frequent cardiac manifestation is conduction abnormalities including transient atrioventricular (AV) heart block, junctional rhythm and asystolic pauses. Van der Linde et al.[5] reported the AV block rates as 49% for third degree, 16% for second degree and 12% for first degree in this disease. In addition, the involvement of myocardium and pericardium was reported in the course of disease[7]. There are a number of non-invasive tests such as gallium scanning and indium-labeled anti-myosin antibody scanning toevaluate the myocardial involvement in Lyme carditis[8]. Magnetic resonance imaging canalsobeused fordiagnosingthe acute carditisin positive cases[9]. In addition, cardiacbiomarkersmay be useful in the diagnosis of acute myocarditis andpericarditis[10]. Echocardiography has a low diagnostic value for the detect of Lyme carditis because of it reveals generally normal heart function. However, echocardiography can be used for monitoring the development of dilated cardiomyopathy[11]. On the other hand, serology is usually the first and often the only supportingdiagnostic measure to be deployed, because it is relatively easy to perform with acceptable sensitivity and specificity[12]. The most frequently usedserologic tests are enzyme-linked immunosorbent assay (ELISA), immunofluorescence assays and Western blotting[13]. Generally, the sensitivity of ELISA is less than 50% in acute-phase of patients with erythema migrans(EM). Sensitivity increases rapidly over time after the first week in untreated patients with EM. In addition, sensitivity is very high in patients with objective evidence of extracutaneous involvement (e.g., carditis or neuroborreliosis)[14]. Whole-cell antigen preparations lack specificity because of the presence of cross-reacting antigens of B. burgdorferibroadly. These include common bacterial antigens such as heat shock proteins, flagellarantigens, and others[15]. In this case we have used ELISA kits. However, the limitations of antibody tests must be appreciated. Antibody response in early LB may be weak or absent. On the other hand, a positive specific antibody response may persist for months or even years after successful treatment of the infection, so follow-up of antibody titres in patients following therapy is not a reliable approach for monitoring success of treatment.Temporary cardiac pacing may be required almost a third of cases of Lyme carditis and complete recovery occurs in more than 90% of patients. It has been suggested that the Lyme disease affects the conduction system as a result of the direct dissemination of spirochetes into cardiac tissues, the inflammatory response associated with the infection, or both[16].It has been reported that antibiotic therapy in the early stages of disease prevents the later complications[17]. Patients with minor cardiac involvement (first-degree AV block with PR interval <0.3 s) could be treated orally with doxycycline, tetracycline or amoxicillin[18]. Doxycycline is preferable because of its higher efficacy in other tick borne diseases (babesiosis, ehrlichiosis, anaplasmosis) that could be co-transmittedand might aggravate the outcome[19].Patients with more severe conduction system disturbances (first-degree AV block with a PR interval >0.3 s, second or third-degree AV block) should be hospitalized in a coronary care unit and given either intravenous ceftriaxone or high-dose intravenous penicillin G. Insertion of a temporary transvenous pacemaker could also be consideredaccording to patients’s clinic status. In the literature, permanent pace maker was used in only one case because ofrefractoryAV blockto aggressive pharmacological therapy. In all other cases, permanent pacemakers were implanted prior to the definitive diagnosis of Lyme disease[20].
4.Conclusions
- In the patients who haveAV block of unknown cause, Lymecarditis may be considered as the alternative diagnosis. Early testing and initiation of antibiotic treatment is essential to prevent the later complications.Thus, early diagnosis and treatment may be avoided unnecessary implantation of a pacemaker.