-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Architecture Research
p-ISSN: 2168-507X e-ISSN: 2168-5088
2019; 9(4): 83-98
doi:10.5923/j.arch.20190904.01

Context Considerations for a New Children's Hospital in Palestine with a Particular Focus on Public Spaces
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLRawa Abulawi 1, Stuart Walker 2, Christopher Boyko 2
1Interior Design, An-Najah National University, Palestine
2Imagination, Lancaster University, United Kingdom
Correspondence to: Rawa Abulawi , Interior Design, An-Najah National University, Palestine.
| Email: |  |
Copyright © 2019 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This research discusses the literature review that covers three aspects related to the context of Palestine: Palestinians background; special considerations related to interior architecture and interior design; and health system in Palestine. The literature review discusses general information that provides an overview of the importance of creating a dedicated children's hospital in Palestine. The context of this study identified four important factors that may have a potential influence on healthcare design in Palestine, particularly children's hospital design. Such issues provide a strong platform to conduct qualitative research that uses an innovative workshop format for a new children’s hospital in Palestine. The key findings of this research provide recommendations for the design of children's hospitals, particularly public spaces in the context of Palestine.
Keywords: Children’s hospitals, Architecture, Culture, Healthcare system
Cite this paper: Rawa Abulawi , Stuart Walker , Christopher Boyko , Context Considerations for a New Children's Hospital in Palestine with a Particular Focus on Public Spaces, Architecture Research, Vol. 9 No. 4, 2019, pp. 83-98. doi: 10.5923/j.arch.20190904.01.
Article Outline
1. Introduction
- The importance of this research stems from the fact that few hospitals are specialized in the treatment of children in my homeland, Palestine. Most of the Palestinian children are treated in adult hospitals that lack the comfortable environment that helps lessen the level of trepidation and worry of children during their hospitalization [1].In 2004, I gave birth to a child who suffered from an illness that was impossible to diagnose until he was one year old. Diagnosing the problem required visits to several hospitals in Palestine. He had to be hospitalised for several days, which allowed me to see first-hand the poor conditions of primary care, especially for children. For example, there was no place for a parent or primary carer to sleep; only a small chair beside the bed, and the room was shared with eight other children, along with their mothers and other visitors. In addition, there were no public spaces set aside for children to play and no consideration of the aesthetics of the environment that might help children forget their illness. In other words, the environment was not conducive to supportive healing. As an architect and interior designer, these images and memories stimulated me to ask: for a new children's hospital in Palestine, how can we provide a supportive environment for all age ranges of children, particularly in the public spaces? By answering this question, the literature review contributed to the context of Palestine especially Palestinian background; special design considerations related to architecture and interior design; environmental considerations; and healthcare system in Palestine.
2. Literature Review
- From literature, there is only limited research that focuses on the interior architecture and design of children’s hospitals [2] especially in public spaces, such as atriums; and there are gaps in the empirical evidence for creating appropriate and comfortable environments conducive to supporting healing [3]. Few studies include the preferences of children in the design of the public spaces [4]. In addition, there are few studies that have discussed in detail how the medical functions in hospitals affect the design of the main entrance and atrium of children’s hospitals or their relationship to supporting healing [5]. Moreover, there is a lack of consistency with respect to the functions and requirements of the interior spaces, including the supportive activities that are accommodated in the public spaces [6]; e.g., some hospitals provide a play area for smaller children in the main entrance, others do not [7]. Design for children should be distinct from design for adults [8]. The spaces are be for children of different ages, and so the interior design needs to be flexible and adaptable [9]. Such needs can be translated into supportive healing spaces. Despite this, we still find healthcare spaces that do not address the needs of children across all ages [1]. Instead, they tend to support the views of adults or may encompass themes that are appropriate for younger children but not for adolescents. Hence, it is important to include the views of children of all ages in the design, as well those of parents, in order to develop best practice [10].Children’s hospitals should offer spaces and provide welcoming interior environments as well as facilities that accommodate children of all ages, and allow them to feel comfortable and at ease [11]. Generally, however, interior spaces are still not designed to meet the specific cognitive needs of children [12]. For instance, many Palestinian children are treated in adult hospitals that do not have a child-oriented environment conducive to healing [1].
2.1. Palestinian Background
- The Palestinian health sector has been affected by several factors that have influenced the development, structure and accessibility of health services. These include: occupation, culture, architecture, economics, and environmental considerations (i.e. climate and location, topography, typology and materials). Before discussing these factors, we will first consider the geography of Palestine.Palestine is located on the eastern side of the Mediterranean Sea, bordered by Lebanon to the North, Egypt to the South, and Jordan to the East [13]. This unique location has given it an important historical status and has made it a target for invaders over thousands of years. Palestine is split geographically into the West Bank and the Gaza Strip. The latter is considered the most densely populated area on earth [14]. The number of Palestinians worldwide recently reached 13 million: 4.2 million live in the occupied Palestine territory; 2 million are refugees; 1.3 million live in Israel; and 5.5 million live abroad [15]. Palestine has a total area of 27,000 km2. Israel controls 85% of the area [15]. Palestinian society is proportionally young; according to the Palestinian Central Bureau of Statistics [16] the proportion of individuals under the age of 15 years is 41.3%, while the proportion of elderly individuals is low (see Figure 1). For instance, in another statistic by PCBS [17], the percentage of young children between 0-17 years old forms 51.04-53.04% of the total population, particularly in the cities of Nablus, and Khan Yunis (see Figure 2). Such statistics indicated the need of a dedicated children hospital in Palestine.
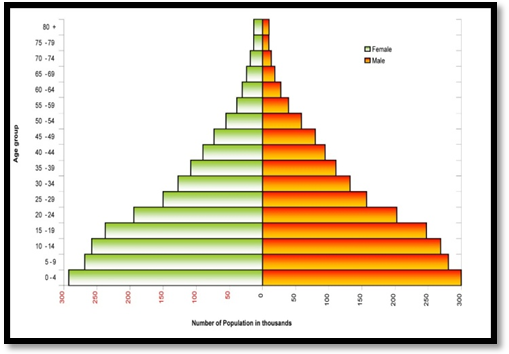 | Figure 1. Palestinian population pyramid – notice the high proportion of individuals under the age of fifteen years is 41.3 % while the proportion of elderly is low [16] |
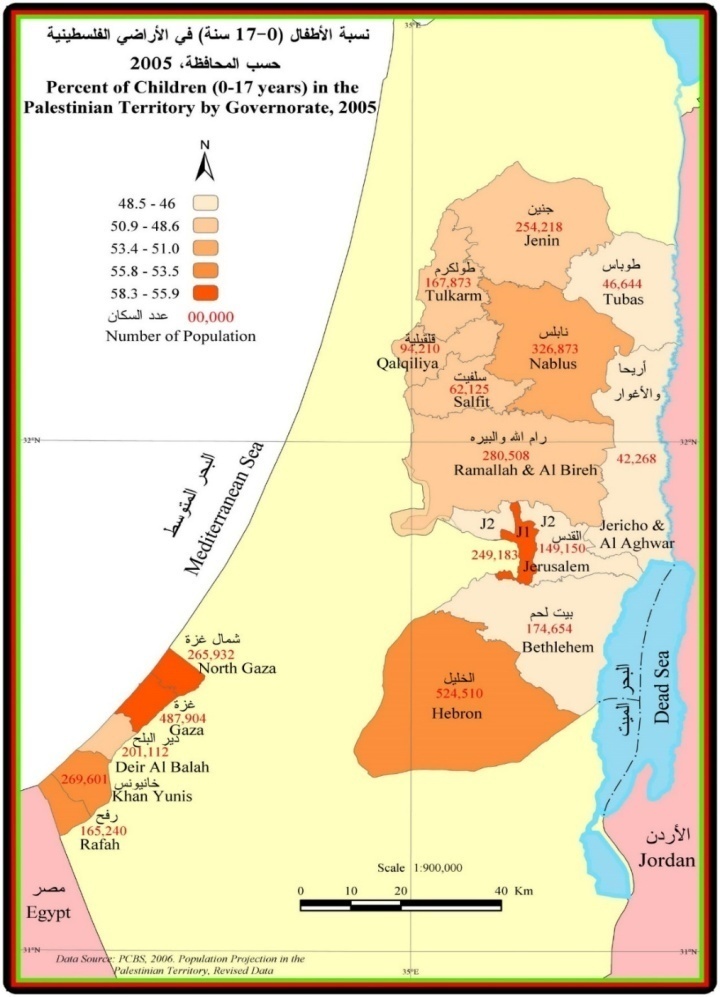 | Figure 2. Percentage of children between 0-17 years in the Palestinian Territory Governorate [17] |
2.2. Special Considerations
- The literature review identified many factors that have had positive or negative effects on Palestinian life, including culture, and architecture (indoor space and outdoor space), economics, functions, and environmental considerations (i.e. climate & location, topography, typology and materials):
2.2.1. Architecture and Interior Design
- The architecture of Palestine has been interpreted and affected by different cultures and layers of history, and has also been impacted by the changing political conditions [22]. Senan pointed to the contradiction between traditional and contemporary architecture in Palestine. This contradiction caused a sense of loss and confusion and obscured the identity of the Palestinian territory for its inhabitants [23]. As a result, significant architectural heritage with different styles has emerged in Palestine—including traditional and contemporary architecture [24]. Contemporary (modern) Palestinian architecture can be described as architecture that has been created from new materials and techniques. At the beginning of the 20th century, new materials such as cement and steel were used for the first time, resulting in new structural designs, such as beams, columns and thinner walls [24], [22]. However, traditional architecture refers to a structure that has been created in a traditional way, using local materials and techniques, and is designed to react to nature and extreme changes in climate [19]. Traditional Palestinian architecture has different characteristics according to the different climates and materials of specific areas. For example, different styles of roofing are used in some areas to adapt to the weather conditions [24]. Within the literature, it is clear that traditional Palestinian architecture was affected by different cultures, such as the Ottoman, Roman, Byzantine, Crusaders, and many others who left their influence on the traditional architecture. Many buildings still survive from the Ottoman period as well as some connected to Mamluk architecture and a small number related to the Umayyad and other periods [24]. There are many elements and details that distinguish traditional from contemporary architecture (i.e. very thick walls, inclined roof, floors, iwan courtyard and fountain, portico, openings, Al-Mashrabiya (Figures 3-5), plaster and limewashing (for more details see [19], [24], [25].
 | Figure 3. Mashrabiya and shade in the courtyard [19]. |
 | Figure 4. Inside a traditional courtyard house [19] |
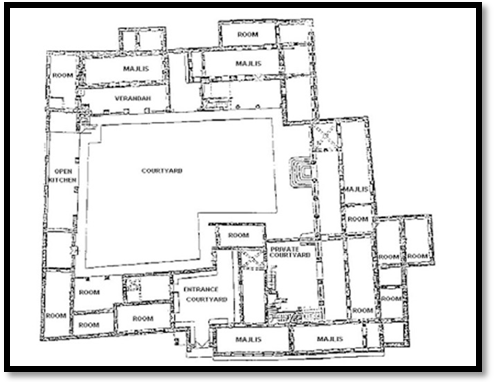 | Figure 5. Plan of a traditional courtyard house [19] |
2.2.2. Factors affecting Palestinian Architecture and Interior Design
- Culture: It can be manifested in both physical objects and subjective responses to the environment [26]. According to Jabareen [27], the concept of culture and its components, such as worldviews (i.e. value, meanings, norms, standards, expectations, rules), kinship relations, family structure, gender, politics, religion, and social networksare manifested in people’s behaviours and in the design considerations of houses in Gaza [27]. For instance, one of the most important elements of traditional architecture is the courtyard. It reflects Palestinians’ beliefs, religion, traditions, and economic and cultural aspects. In the literature, the courtyard in Palestine is considered a sustainable space. Courtyard design differs in size and shape according to the geographical location, type of climate, property shape, restructuring activities, and socio-cultural situation. Generally, two types of courtyards are used: the first is surrounded by the building and open to the sky. The second has been created by adding rooms around an open space as the family increases in size. The concept of using courtyards is to: i) create an open space for circulation; ii) to provide private space; iii) to create a social gathering area and for security; iv) to provide daylight; and v) to be used day and night in winter and summer according to changes in temperature [19], [24].In Palestinian culture, hospitality is paramount, so the interior decoration of the guest room is always specifically designed [28]. In addition, privacy is the most important element when designing the interior space, particularly the spaces where women spend most of their time. For instance, in Nablus city, privacy in indoor and outdoor spaces is preferred, so, to achieve this, they suggested using light materials such as aluminium windows, window boxes and canopies [38]. Palestine shares its Islamic values alongside a Christian and Jewish culture [29]. The largest section of Palestine is Islamic (Sunni), particularly those parts under the Palestinian Authority, with smaller Christian and Jewish areas. The Sunni religion affects Palestinian arts, design and graphics. For instance, Islam forbids the portrayal of people and animals; most Arab designs feature plants, greenery, geometric shapes, and calligraphy [30].Economics: It is clear that people with low incomes are not able to build the same type of houses as rich people [27]; [31]. In 2005, the Palestinian National Poverty reported“three out of five Palestinians live under the income poverty line” and “a third of the Palestinian population lives under the consumption poverty line”; the level of poverty in Gaza was twice that of West Bank [29]. Consequently, interior design is affected by factors that include personal, economic and social features [32]. Some Palestinians organise the interior décor of their houses using purely a modern or traditional theme, while others used a mixture of both. For example, the interior decoration of guest rooms in the West Bank villages reflect and represent the unity of the family by displaying photographs of male family members. Such elements represented the taditional themes of interior décor [32]. Function: the function of the building plays an important factor in shaping the form and the style of the buildings [27]. The function of the courtyard is particularly important. The courtyard (Hosh) can be used for different social celebrations such as weddings; funeral ceremonies; and domestic activities, such as eating, cooking, sleeping, entertaining, meeting members of the family, and playing [28]. Climatic considerations: The climate of Palestine is in general influenced by the Mediteranean climate: hot and dry in summer and short, cool, rainy winters [33]. However, this climate has some variations according to the topographical regions in the West Bank/Palestine [24], [34]. For instance, in the the West Bank (Nablus City) it’s warm and sub-humid in summer and cold in winter:mechanical cooling and heating systems are needed. The orientation of the building is important to tackle the various types of climate. In Nablus city, the outdoor spaces are oriented to the west to deal with the excessive heat of summer and the strong winds that come from the northwest [28]. More information can be found at [19], [24].
2.3. Health System in Palestine
- The Palestinian healthcare system is a mixed system divided into four sectors [35], [36]:(1) the governmental sector, administered by the Ministry of Health (MOH);(2) private sector for profit;(3) the NGO sector for non-profit; and(4) the sector run by UNRWA (The United Nations Relief and Working Agency for Palestinian Refugees in the Near East).The diversity of the Palestinian service has enabled the health system to face the challenges brought about by regional conflict, but it also leads to diffusion and duplication of the services [37].The Ministry of Health manages public health services and delivery of primary, secondary and tertiary care in governmental facilities. It has primary responsibility as the provider and regulator of the health sector [20].Private sector health provides services such as clinics, hospitals, pharmacies, laboratories, and radiology, physiotherapy, and rehabilitation centres. According to the Municipality of Health, in 2006, the private sector provided approximately 433 beds in twenty-three hospitals that specialised in maternity and diagnostic units [37]. NGO services have declined in Palestine since the establishment of the Ministry of Health. However, they do still provide most secondary and tertiary care services, especially for underserved and vulnerable populations in rural areas [37]. UNRWA has played a significant role since 1950; they provide a health service for the 1.3 million Palestinian refugees in the West Bank and Gaza with only 10% of the total Ministry of Health budget. UNRWA health services include primary and some secondary care, disease prevention and control, family health, health education and physiotherapy support [37].The Palestinians healthcare system depends on many sources for income. The USAID [37] pointed to these main sources:(1) General taxation(2) Health insurance premiums, fees, and co-payment(3) Private for-profit investment(4) International donors including UNRWA(5) Household expenditure
2.3.1. Factors Affecting Health and Health System
- The ongoing conflict in the region has had a detrimental effect on the health system in Palestine [31]. According to UNRWA [38], the conflict between 2007-2008 damaged 15 hospitals and 41 health clinics in the Gaza Strip [38]. In addition, low incomes, unsuitable housing, unsafe workplaces, and lack of access to health facilities have negatively affected the health of residents [14].
2.3.2. Evaluation of the Health System in Palestine
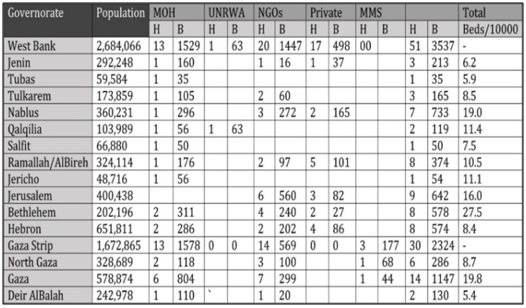
- The health service in Palestine has remained static, with no potential improvement registered since the 1990s [15]. There are still gaps in the quality of health service provision. Uncomfortable interior environments for waiting areas and the need for privacy indicate an urgent need for investment in the clinic infrastructure [39]. Access to adequate health service in Palestine remains low due to financial, geographic and political barriers [37].According to Horton [40] the Palestinian health system can be improved by having a balanced solution of economic, social and political accountability. Eklund [18] pointed to the importance of increasing the number of hospitals to increase the accessibility of Palestinian people to reach their healthcare services. The Palestinian Authority and Ministry of Health created several strategies to develop the health sector in Palestine with the collaboration of foreign countries. One of the primary strategies is to increase access to the health services by increasing and establishing new facilities [39]. The proposed complex will be represented by four new hospitals (i.e. Sheikh Zayed Hospital for emergencies, Kuwait Hospital for specialised surgery, Bahraini Hospital for paediatrics, and blood banks in Ramallah city); these will provide specialised services and tertiary care to the Palestinian people [37]. According to the literature and these strategies there is no suggestion for establishing a dedicated children’s hospital in Palestine, although the number of children under five years of age accounted for 14.7% of the total population living in the Palestinian territories; 40.2% were in the age group (0-14 years) [41]. According to the WHO [42] young people’s mental and psychological health needs focussed attention because they face a combination of violence, high levels of unemployment and a lack of control over their lives [42]. Furthermore, there is a need to improve the management of health facilities, physical environments, and satisfacion of stakeholders, in especially hospitals [20].There are eighty-one hospitals in Palestine [43]. They are distributed in the West Bank (Figure 6) and Gaza (including East Jerusalem). More details can be seen in Table 1.
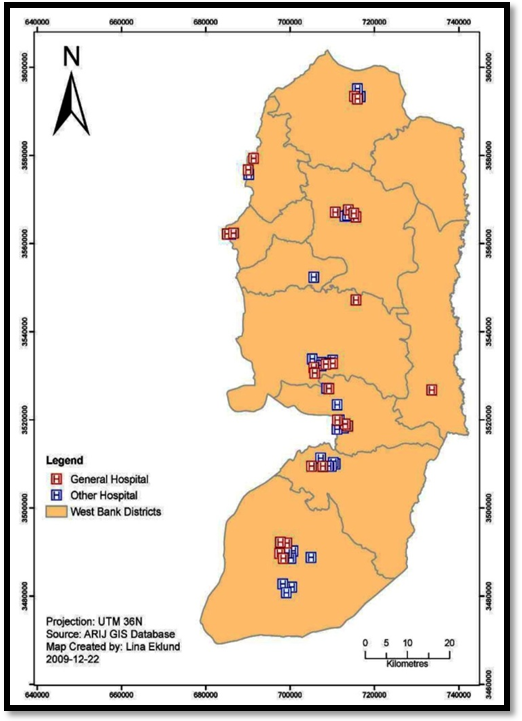 | Figure 6. Distribution of hospitals in Palestine/West Bank [18] |
|
|
3. Design Considerations
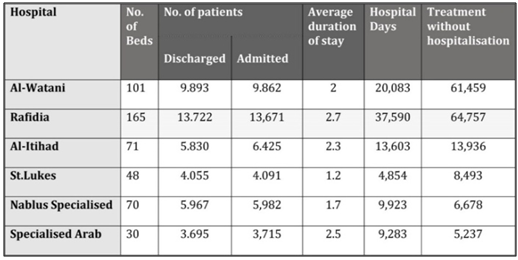
- Context specific issues identified four main factors that designers should consider for a new children's hospital because they have a potential influence on healthcare design in Palestine, particularly children’s hospital design. These factors are related to:(1) Architecture: Palestinian traditional and contemporary architecture has been influenced by three key elements i.e. culture, economics, and function.(2) Interior design: three concepts of interior design are used i.e. purely modern, traditional, or a mixture of both. (3) Evironmental considerations: three important environmental elements were identified: topography and climate and location. (4) Healthcare system in Palestine highlighted three issues that need to be taken into consideration.• The Palestinian healthcare system is a mixed system divided into four sectors, which tends to result in duplication of resources and inefficiencies. • It is important to increase the number of hospitals in Palestine.The Palestinian healthcare system depends on many sources for income i.e. general taxation health insurance premiums, fees, and co-payment; private for-profit investment; international donors including UNRWA; and household expenditure.Based on the evaluation of the healthcare system in Palestine, four key issues were identified that need to be taken into consideration for this research:(1) There are still gaps in the quality of provision of appropriate environments within the health service (i.e. uncomfortable waiting areas and the need for privacy). (2) There is a need to increase the number of hospitals in Palestine to foster accessibility, but there has been no recent announcement by the authorities to establish a hospital dedicated to children.(3) Nablus city is one of the largest cities in Palestine. It has eight hospitals but none of these has the capacity to provide treatments for all age ranges of children (0-18 years). Rafidia Surgery Hospital, the largest public hospital in Palestine/Nablus city, is the only public hospital that can accommodate children from 0-13 years. However, this hospital still lacks some of the appropriate environments to accommodate children. For instance, it does not have a sufficient number of beds, play areas for children, nor a special waiting area for children’s parents to stay with their children. In addition, the number of children aged between 0-17 form around 51.0-53.04 of the population of Nablus city [16].Thus, for the above reasons, it is important to provide a dedicated children’s hospital in Palestine. Although the literature review provided key design considerations for designing children’s hospitals to create healing environments, one still finds uncertainty about:• How to involve children in the design process.• How children can contribute in the early stages of the design process for creating more age-appropriate and healing environments.• How to include children, parents, medical staff, psychologists and others in the process of designing their healthcare settings.• What methods should be adopted to ascertain the perspectives of children to achieve effective change in optimising the healing environment?• How to uncover the specific psychological needs of children.• How to incorporate environmental, interior architecture and interior design considerations that result in age-appropriate public spaces in hospitals.• How to design a programme for medical functions and its effect on the interior design and interior architecture that can or should be contributed to the public spaces of children’s hospital. It is important to study the considerations related to the design of hospitals in Palestine due to the different cultural and social influences in the region. Thus, for a new children’s hospital in Palestine, and for all the above reasons, this research will use qualitative research that employs an appropriate and innovative workshop format. The field research will be conducted in Palestine, particularly in Nablus city.
4. Methodology & Methods
- This study employs qualitative research that uses an innovative workshop format. Data were collected using ten co-design and co-creation workshops that included arts-based activities and semi-structured recorded interviews conducted in Palestine. Participants included children from 3-18 years, parents, doctors, nurses, staff from the reception and admissions desks and four groups of designers. All the participants, apart from the designers, participated in drawing and modelling activities. These methods can provide valuable information and lead to better design solutions; use of drawings with children is considered an indispensable and valuable tool because verbal expression is often insufficient, not only because of a lack of developed vocabulary but also because preferences and ideas can be expressed more intuitively [45]. Similarly, models can be an effective tool because they can express ideas and preferences about form, materials and size, and can facilitate and represent the ideas of children [46].Sample size: Fifty-five participants (n=18 school children (9 male (m) & 9 female (f)), 5 children under six years (1m & 4f), 8 parents (4m & 4f), 3 doctors (1f & 2m), 4 nurses (2f & 2m), 2 staff members (f) working in admissions and reception; 12 designers (7m & 5f), and 3 individual interviews (2m civil engineers & 1m Director of Rafidia Surgical Hospital).Before starting the data collection, I acquired all necessary ethics approvals from the RSO Ethics Committee at Lancaster University.Data Analysis & Results: A thematic analysis approach was used to analyse the primary data. [47]. The results of data analysis helped to identify two major themes connected to the participants’ preferences (See Appendix B \Figure 17):(1) Context-specific issues to be taken into consideration for children’s hospitals: culture, appropriateness of visitors’ area, age appropriateness of hospitalisation, and support of the children by family and friends.(2) The physical environment: interior architecture and interior design: medical spaces, non-medical spaces, design elements, and environmental considerations.The emerging themes will inform the development and design of the interior architecture and the interior design of the public spaces of a children’s hospital in the particular context of Palestine.
5. Findings & Discussion
- The initial results of the workshops conducted with children, parents and medical staff were tabulated, and the findings shared with the designers prior to their workshops in order to provide a comprehensive decision that could help the reader consider if the findings could be transferred to other situations [48]. A comparison of the findings with previous studies is included [49]. All the findings and design insights from the discussion that included findings from literature and field research with feedback on those results from the designers’ workshops were classified and prioritised; e.g. findings that were supported by, different from, or not included in, the literature, and findings that are essential and recommended. These categories were synthesised and provided along with some critical considerations of the findings, which helped in developing initial recommendations (See Appendix C) and drawing out conclusions to inform evidence-based healthcare design guidelines. The developed recommendations encompass general recommendations (GR), and recommendations related to the specific context of this project-Palestine (PR).
6. Conclusions
- This study identifies the importance of context specific issues in designing children's hospitals, particularly public spaces. Following this, designers should consider the initial recommendations to design interior architectural spaces related to public spaces of children's hospitals. However, testing the findings and triangulating them through survey research will provide further valuable insights that help to provide supportive environments, particularly in the public areas that are appropriate for all age ranges of children. To achieve that, it is important to validate the initial recommendations from this research study by discussing findings with parents, children, staff, and designers, to ensure that the interpretations of what was said in the field research is reasonably accurate, and to obtain input from them.
ACKNOWLEDGEMENTS
- We would like to show our grateful to all the research participants, and to An-Najah National University to support this research.
Ethics Issue
- Before starting data collection, researchers acquired necessary ethics approvals from the RSO Ethics Committee at Lancaster University.
Appendix A
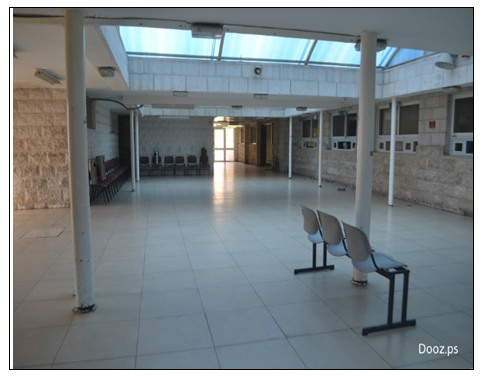
- Sceines that explain the unappropriate design and evironments related to Rafidia Surgical Hospital (figures 8—15).
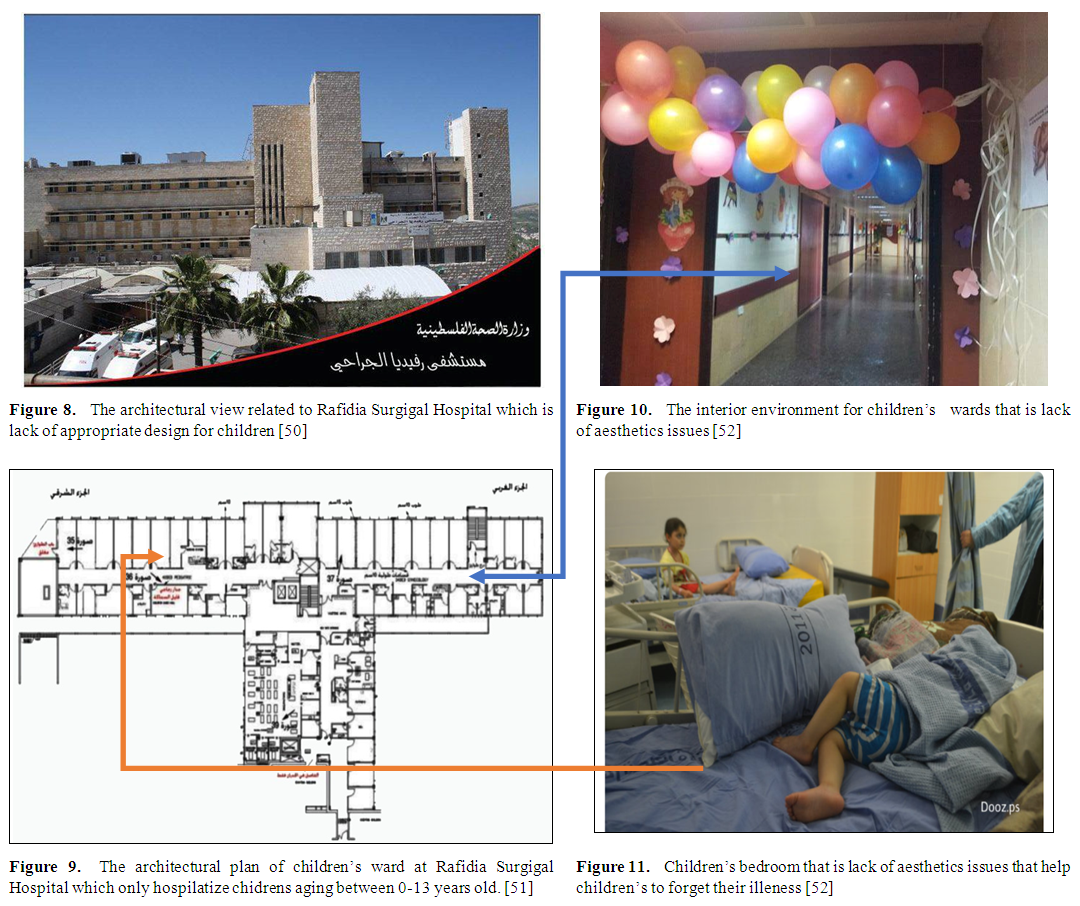 | Figure 8-11 |
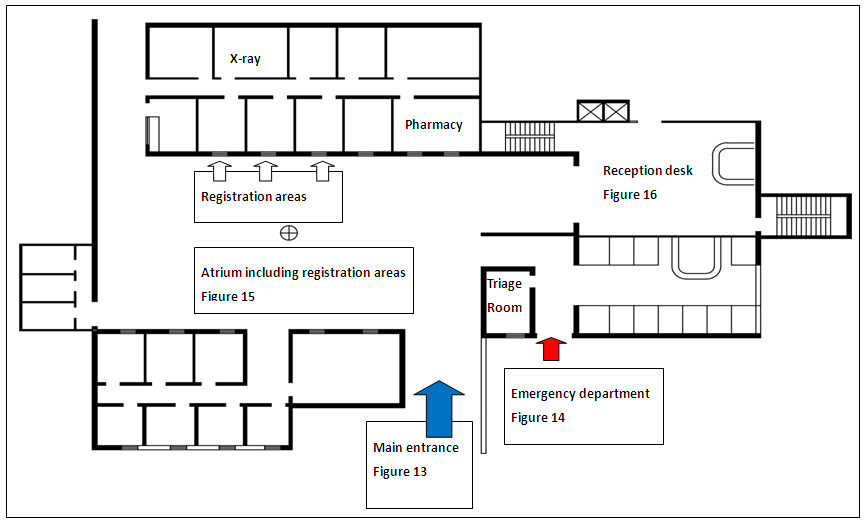 | Figure 12. The public spaces of Rafidia Hospital that is including main entrance, atrium, reception, and registration areas 0-13 years old. [Researcher] |
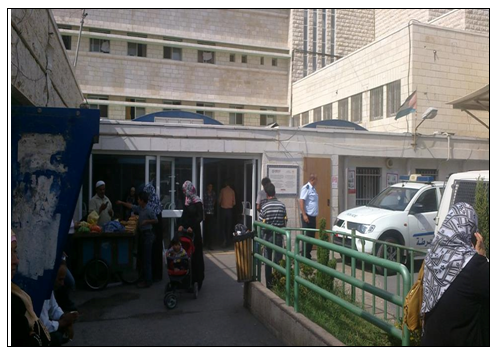 | Figure 13. The main entrance of emergency department located in close proximity to the main entrance of the hospital. Such issue can cause fears for children which they acces to the hospital [Rsearcher] |
 | Figure 14. The interior environment of the Rafidia Hospital atruim. The interior enviroment do not include spaces for children (e.g. play areas), aesthetic elements or enough spaces and comfortable environment for users patriculary parents to wait their turn or to hospitalize their children [Researcher] |
 | Figure 15. The interior environment for children’s wards which is lack of aesthetics issues [52] |
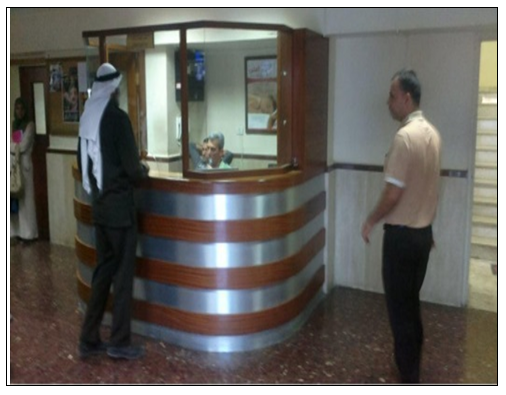 | Figure 16. The reception area of Rafidia Surgical Hospital [source researcher] |
Appendix B
- Data Analyis and Results
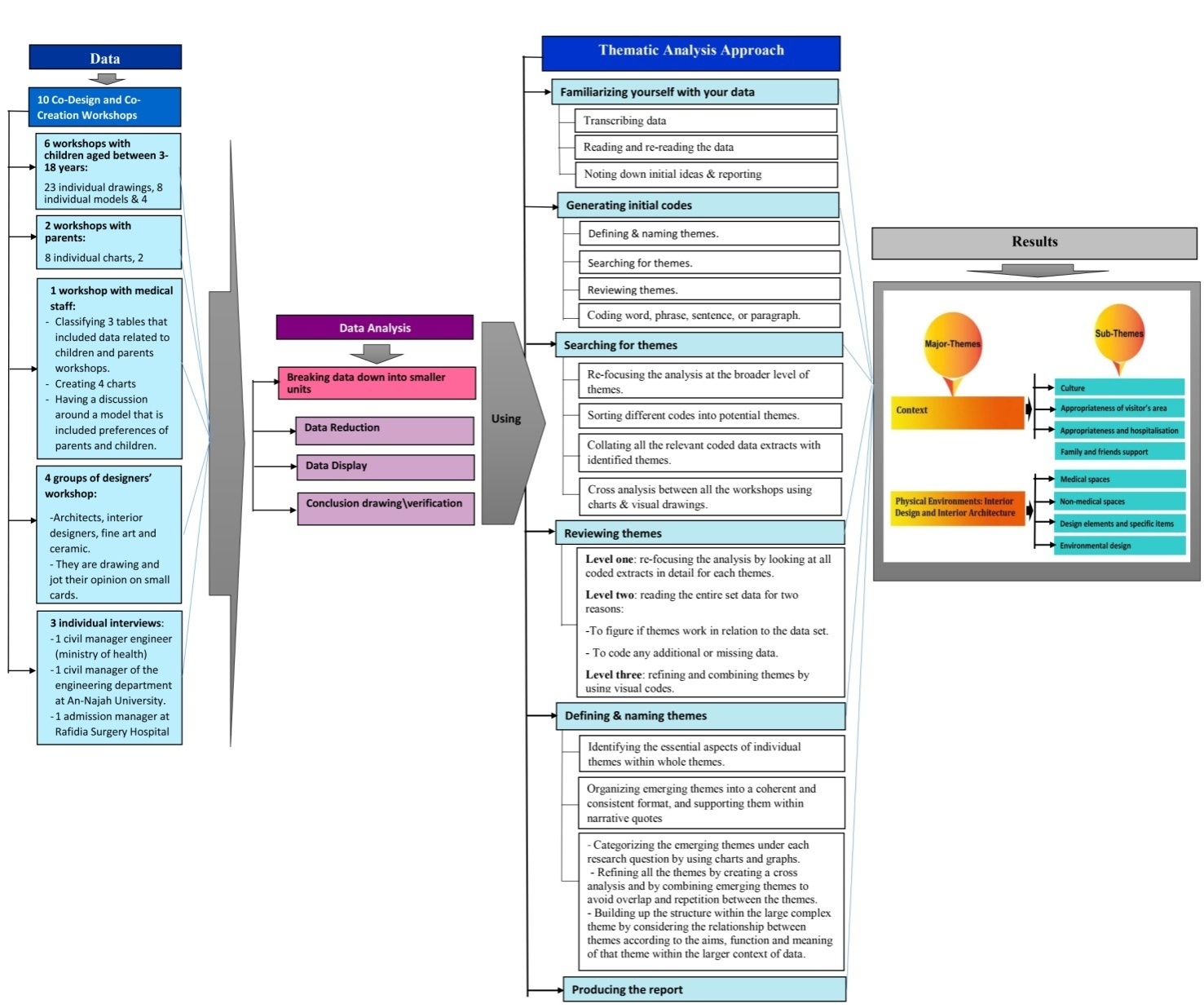 | Figure 17. Data analysis and results |
Appendix c
- 1. Recommendations that are essential to provide supportive healing environments and age-appropriate design for children.1.1. Recommendations related to aesthetic components Art. The findings included various types of art-related suggestions. From these findings, the following recommendations are made: 1.1.1. The interior design of public spaces of children’s hospitals should include:• Various types of art related to nature, water themes, culture, music, and semi-permanent and impressionistic abstract art, particularly in the main entrance, waiting, admission, and registration areas. However, designers should concentrate on using art that is connected to nature and water themes, and should prevent cartoon-like art. This is a general recommendation. [GR].• Art that encompasses traditional elements and motifs relevant to the culture in Palestine. This recommendation applies specifically to the Palestinian context. [PR].Colours. The findings included a number of colour-related suggestions. From these findings, the following recommendation is made:1.1.2. The interior design and interior architecture of public spaces should include different types of colours, but with a concentration of using natural colours and light colours, and the use of colours as a way of coding to provide identity to the different areas and to help with wayfinding. [GR]Furniture. A high value was placed on including various types of outdoor and indoor furniture-related suggestions Therefore, from these results, the following recommendation is made:1.1.3. The outdoor and indoor public spaces of children’s hospitals should provide an adequate amount of furniture that is adaptable, safe, age-appropriate, durable, home-like, modern, and has circular and organic forms and shapes. [GR]Thematic design. The findings showed different types of thematic design-related suggestions. Therefore, from these findings, the following recommendation is made:1.1.4. The interior design of public spaces of children’s hospitals should include thematic design related to nature, particularly in the waiting areas. However home-like design and design that includes storytelling and symbols should also be applied, but perhaps in other areas. [GR]Forms and shape. The discussion of findings acknowledged various types of forms and shape-related suggestions. Therefore, from these findings, the following recommendations are created:1.1.5. The interior architecture and interior design of public spaces of children’s hospitals should include:• Various forms and shapes (e.g. circular, organic smooth, gable roofs, symmetrical, l-shape, and irregular forms). [GR].• Forms that reference cultural heritage and combine traditional architectural elements with modern elements related to Palestine. This should be included specifically for the main entrance. [PR]Wayfinding. The findings yielded different considerations to wayfinding signs- related suggestions. Therefore, from these findings, the following recommendations are made:1.1.6. The interior design and interior architecture of public spaces of children’s hospitals should:• Include clear, attractive, and appropriate wayfinding signs with a provision to integrate wayfinding signs with thematic interior design and architecture of public areas. [GR].• Provide three different themes of wayfinding signs related to medical, non-medical and entertainment and play areas. [PR]Materials. The discussion of findings showed various types of materials-related suggestions. Therefore, from these findings, the following recommendation is constructed:1.1.7. The interior architecture and interior design of public spaces of children’s hospitals should include various types of materials such as non-absorbent, bright, textured, safe, transparent, soundproof, easy to clean, and materials connected to nature.Attractive distraction elements. The findings showed a high value was placed on including attractive distraction elements. Therefore, from these findings, the following recommendation is created:1.1.8. The interior design and interior architecture of public spaces, particularly the main entrance, waiting areas and registration areas should include attractive distracting elements for children. [GR].1.2. Recommendations related to design according to ageDividing interior spaces of reception, waiting and playing areas according to age. The findings showed different age-related suggestions. Therefore, from these findings, the following recommendations are made:1.2.1. The design spaces of public areas of children’s hospitals should:• Provide design according to all age ranges of children, particularly in the waiting, reception, and play areas. [GR].• Divide public spaces of children’s hospitals according to age ranges of children, particularly in the waiting areas, play areas, admission and reception. Four suggestions can be applied: 1. Play areas and waiting areas into two age ranges (i.e. 0-8, 8-18 years);2. Play areas into three age ranges (i.e. 0-6, 6-12, & 12-18 years);3. Waiting areas into three age ranges (i.e. 0-6, 6-12, 12-18 years); however, the 12-18 age range should consider gender issues; 4. Reception, information and admission departments into three age ranges (i.e. 0-6, 6-12, & 12-18 years). [PR]Age ranges – preferences and cognitive development of children.Findings that do not alter according to age. The findings showed various and different preferences related to children that do not alter according to age ranges and cognitive development of children. Therefore, from these findings, the following recommendations are made:1.2.2. To provide age-appropriate design for all age ranges of children, the interior architecture and interior design of public spaces of a dedicated children’s hospitals should consider:• The inclusion of circular, soft and organic forms and shapes, materials connected to nature, textured materials, colours including blue, green, purple, pink, brown, and yellow, art connected to nature and music, and various types of games and entertainment activities (physical/active, passive/quiet, and learning/educational). [GR]• The provision of schematic colours related to green, blue, yellow, purple, pink, and brown, and abstract art to the context of this study. [PR]Findings that vary according to age. The findings identified four elements- related suggestions. Therefore, from these findings, the following recommendations are created:1.2.3. To provide age-appropriate interior design and interior architecture for the public spaces of children’s hospitals, designers should:• Include thematic design connected to nature. However, there should be a consideration of how children depict nature according to their cognitive development. [GR]• Consider differences in cognitive development between age ranges of children regarding the inclusion of spaces for food, irregular forms and shapes, and symbols. [PR]Findings that are related specifically to age ranges. The field research identified some elements that are connected specifically to age ranges of children-related elements.. Therefore, from these findings, the following recommendation is made:The interior design and interior architecture of public spaces of children’s hospitals particularly in the context of this project should consider the differences across age range preferences and needs, specifically in relation to the inclusion of bright and glittery materials, colours related to orange, turquoise, black, white, and red, games and entertainment activities, and separation between genders particularly for age range 15-18 years. [PR].Age-appropriate hospitals in Palestine. Field research showed that current hospital environments are inadequate, especially in relation to age-appropriateness. Children’s wards in existing hospitals cater to the ages 0-13, with older children entering adult wards. Also, there is no dedicated children’s hospital in Palestine. Therefore, from these findings, the following recommendation is made:1.2.4. The Palestinian Authority should give serious consideration to the creation of a dedicated children’s hospital in Palestine that serves the age range 0-18 years. [PR].1.3. Recommendations related to gender difference, minor or no differenceThe findings identified some preferences of children that have gender differences, others showed minor gender differences, and some included no gender differences. Therefore, from these findings, the following recommendations are made:1.3.1. The interior design of a dedicated child’s hospitals, in particular public spaces, should consider gender differences regarding the inclusion of symmetrical forms, and minor differences between genders of children regarding the inclusion of impressionistic types of art. [GR]1.3.2. It is essential for interior designers and interior architects in Palestine when it comes to designing a new children’s hospitals to consider:• The differences between genders of children regarding the inclusion of abstract art, and the colours purple, white, brown and pink. • Minor differences between genders of children regarding inclusion of impressionistic type of art, circular, smooth and organic forms and lines.• No gender differences regarding the inclusion of art connected to nature, form and shape connected to culture, and schematic colours related to blue and green. 2. Recommendations for the provision of a supportive environment for all stakeholders2.1. Recommendations related to the interior architecture plan for the various spaces and activitiesThe findings indicated various design considerations related to the location of non-medical and medical spaces, access, integration between inside and outside green areas, types of waiting areas, separation between young and older children, inclusion of courtyards, supplementary non-medical spaces, security and saftey, architectural open plan design, and environmental design considerations.1.1.1. The architectural design plan of public spaces of children’s hospitals, particularly the main entrance and atrium, should provide:• Easy access between waiting areas and other non-medical spaces related to smoking, breastfeeding, eating, play areas, diaper changing, resting, small shops, coffee shops, snack bars, prayer room and toilets. [GR]• Easy accessibility and wide main entrances with good visibility throughout. [GR]• A prominent location for reception and admission desks with easy access from the car park and to the emergency department. [GR]• Easy access between administration, medical and non-medical spaces; and direct access to the accounting department. [GR]• Integration between outdoor green areas and interior public spaces, i.e. waiting areas, main entrance, play areas, places to eat, and reception. [GR].• Various types of outdoor and indoor waiting areas suitable for short-term and longer-term visiting. [GR]• Degrees of separation between young children’s play spaces and those designed for older children. [GR]• Courtyards in the architectural plan for main entrance spaces that can reflect the spirituality of the space and serve as a concept design that might help in arranging the interior architectural spaces. [GR]• An open plan design concept for reception areas and play areas that allow for good visibility, but the design should provide semi-private design spaces that are distiguished by some visual separation (e.g. screens, or other interior design elements, such as plants) for both genders. This is a general recommendation with particular attention necessary for providing semi-private spaces related to the context of this study. [GR, PR]• Natural ventilation, sufficient lighting, use of cleanable materials and surfaces that can be kept clean and hygenic, and use of sound absorbing materials/dampening, and adequate ventilation to avoid unpleasant smells, especially in a hot climate like Palestine. This is a general recommendation with particular attention necessary for ventilation consideration in hot climates. [GR, PR]• Security in the main entrance that included spaces for police and CCTV cameras to provide safety for all users. [GR, PR]2.2. Recommendations related to provide separation between genders in the public spacesOne of the most significant culture-related findings from this study is the notion of separation between genders. Therefore, from these findings, the following recommendations are made:2.2.1. It is essential to include separation between genders of children in the public spaces of children’s hospitals, particularly in the context of this research. Designers should consider the inclusion of:• Complete separation between genders in the spaces designated for praying, sleeping, and in the toilet areas for children age eight years or older on religious and cultural grounds. [PR] • Partial separation between children over seven years of age, particularly in the waiting and playing areas. [PR]• Complete separation between genders of children above the age of thirteen. [PR]Designers also should consider that:• Children who are younger than fifteen do not pay much attention to separation, even though they prefer to play with children of their own gender. However, children who are fifteen and older prefer strongly to include gender separation to provide them with a sense of comfort.All the (above) recommendations apply specifically to the Palestinian context. [PR].2.3. Recommendations related to provide a) supportive environments for families and friends, b) support for the children by their family and friendsThe findings showed the value in providing easy access to family and friends. Also, the findings identified the importance of providing supportive family spaces for family-related suggestions. From these findings, the following recommendations are made:2.3.1. Dedicated children’s hospitals should provide easy access to family and friends, particularly in the public spaces to support their children during their treatments, but it is important to consider safety issues.2.3.2. The architectural design plan for the public spaces of children’s hospitals should provide indoor and outdoor supportive spaces for family and friends to socialise and to provide them with comfort.3. Recommendations that are essential to the provision of treatments and well-being for children3.1. Recommendations related to medical functional spacesThe findings identified the location and access between eight medical function-related. From these findings, the following recommendations are made:The architectural design plan for dedicated children’s hospitals should include eight functional medical spaces in close proximity, on the same level as the main entrance and atrium, in order to ensure they are readily accessible, namely: emergency, triage room, x-ray, laboratories for diagnosing and testing, outpatient department, pharmacy, physiotherapy and the orthopaedic department, and consulting rooms. Also, the main entrance of the emergency department should be placed away from or be visually separated from the main entrance. [GR].