-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Advances in Life Sciences
p-ISSN: 2163-1387 e-ISSN: 2163-1395
2014; 4(4): 196-199
doi:10.5923/j.als.20140404.02
Female Orgasmic Disorder Treatment Using Cognitive-behavioral Approach
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLSimin Gudarzi
MA in Counseling, Islamic Azad University, Science and Research Branch of Tehran
Correspondence to: Simin Gudarzi, MA in Counseling, Islamic Azad University, Science and Research Branch of Tehran.
| Email: |  |
Copyright © 2014 Scientific & Academic Publishing. All Rights Reserved.
Sexual disorders are more common than was previously thought. They are usually concealed by females due to a variety of reasons such as fear, anxiety, shame, feelings of inadequacy and guilt. The latent problem occurs with other symptoms such as physical discomfort, depression and marital dissatisfaction and causes pathological reactions affecting the entire couples’ communication system as a stress factor. Accordingly, the present study was conducted to treat female orgasmic disorder using cognitive-behavioral approach. The target statistical society includes 30 females aged between 20-40 divided into two experimental and control groups of 15 members. A written questionnaire was then designed and placed at disposal of both group members in which the demographic characteristics of the participants, including age, husband's age, education, spouse's education, number of children, duration of marriage as well as female orgasmic disorder symptoms had been included. Subsequently, the impact of sex therapy with cognitive-behavioral approach on treatment of female orgasmic disorder was merely investigated on the experimental group. The filled out questionnaires were then analyzed by statistical tests using the software SPSS. Considering the P-value of 0.477 and the significance level of larger than 0.05, the null hypothesis was confirmed by which it was approved that sex therapy with cognitive - behavioral approach has an impact on arousal of 20-49-year old women.
Keywords: Orgasmic disorder, Female, Cognitive-behavioral approach, Sex therapy
Cite this paper: Simin Gudarzi, Female Orgasmic Disorder Treatment Using Cognitive-behavioral Approach, Advances in Life Sciences, Vol. 4 No. 4, 2014, pp. 196-199. doi: 10.5923/j.als.20140404.02.
1. Introduction
- Female sexual dysfunctions are categorized as disorders of desire, arousal, orgasm, and pain (including dyspareunia and vaginismus) (ter Kuile et al., 2010). Sexual dysfunction is affected further by different factors such as medical, psychiatric, cultural, and stage of life (Clayton and Hamilton, 2010). The cognitive behavioral treatment (CBT) differs depending on the specific sexual dysfunction to be treated. However, there have been only a few CBT treatment methods for female sexual dysfunction done empirically in a methodologically sound and little is known about which of the treatment components are most effective (ter Kuile et al., 2010). As stated by Plaud in 2007, behavior analytic approaches to sexual disorders have as their bases the relationships among habituation, classical and operant conditioning, and overt sexual behavior. Carey in 1998 carried out a research on sexual disorders and concluded that in the context of the sexual dysfunctions, the initial goal of assessment is diagnosis to determine whether psychosocial or lifestyle risk factors play a significant role in the maintenance of the disorder. Orgasmic dysfunction is a common clinical issue which affects at least 15% of the entire populations (McGloin and Chris Carey, 2006). Female orgasmic disorder is defined as persistent or recurrent delay in, or absence of, orgasm following a normal sexual excitement phase (McGloin and Chris Carey, 2006). Ramage in 2006, briefly demonstrated the complexities of Female Sexual Dysfunction, both in terms of the circumstances in which the problems can arise, and the multiplicity of causations. In a research done by Hanim Ismail et al. (2014) the prevalence and associated factors of orgasmic dysfunction were investigated among Malay women with type 2 diabetes mellitus in Malaysia. They finally concluded that orgasmic dysfunction was highly prevalent among the Malay women regardless of the diabetic state. Spence in 1985 investigated effectiveness of group vs individual applications of behavioral procedures for primary and secondary female orgasmic dysfunction. He found no changes over time in experimental conditions on measures of heterosexual anxiety, sexual activities or attitude towards masturbation. He reported improvements in sexual arousal and ratings of satisfaction with the sexual relationship across all experimental conditions. Fugl-Meyer in 2008 carried out a research to present some of the currently available questionnaire-based methods for identification and quantification of female orgasmic function and dysfunction and to elucidate to which extent women’s orgasmic dysfunction impacts on their level of sexual satisfaction. He recommended further distinctive research on women’s sexual function concluded upon the background that women’s orgasmic function is closely correlated with a wealth of psycho-sexual parameters. Michetti in 2008 conducted a wide literature review to explore, from both a neurobiological and psychological point of view, the development in knowledge of inhibited male orgasm with specific regard to therapeutic approach. He concluded that the integration of future drugs and sex therapy will achieve more satisfactory treatment. Reisinger in 1974 treated a 23-yr-old college woman in a laboratory setting for primary orgasmic dysfunction by employing masturbatory training with erotic stimuli. He could provide evidence supporting the efficacy of the treatment procedures by recording changes in subjective and objective indices reflecting degree of sexual arousal. Atrash et al. (2014) conducted a case-control study to assess Female sexual dysfunction in Egyptian women with lower urinary tract symptoms in comparison to normal women. They concluded that arousal, satisfaction, orgasmic and lubrication disorders were more common in the women with lower urinary tract symptoms. The present study was conducted to test the applicability of cognitive-behavioral approach in treatment of female orgasmic disorder. The target statistical society includes 30 females aged between 20-40 divided into two experimental and control groups of 15 members.
2. Material and Methods
- The present study is a cross-sectional research aims at investigating effectiveness of sex therapy with a cognitive-behavioral approach on reduced orgasmic disorder in women aged 20-40 years old. To that end, the target group were divided into two 15-member- experimental and control groups to detect the impact of cognitive-behavioral sex-therapy approach by a written questionnaire placed at disposal of both group members. The questionnaire include demographic characteristics of the participants such as age, husband's age, education, spouse's education, number of children, duration of marriage as the initial part, while the second part was denoted sexual function, comprising arousal disorder components. In the next step, the T-test was used to analyze filled out questionnaires using the SPSS software. As a psychotherapeutic approach, the CBT addresses dysfunctional emotions, maladaptive behaviors and cognitive processes using a number of goal-oriented, explicit systematic procedures (Schacter et al., 2010). Adopting a blend of cognitive and behavioral therapy, the therapists deal with patients’ anxiety and depression. It is a "problem focused" and "action oriented" technique by which therapist tries to assist the client in selecting specific strategies to help address those problems (Schacter et al., 2010).
3. Results and Discussion
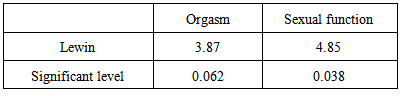
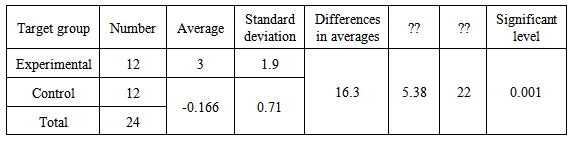
- Personal characteristic analysis The results obtained from analysis of the filled out questionnaire revealed that 41.66% of the entire target group aged between 25 to 30 years old, 8.33% were between 30 and 35 years old and 50% have an age range of between 35 to 40 years old. Furthermore, 25% of the wives of the control group members and 58.3% of control group aged between 20 to 30 years old. The 30-40-year old age cohort contained 33.3% of the experimental group and 25% of the control group. Around 8.33% of the experimental group aged between 50 to 60 years old. The length of marriage varied from 1 to 10 years in 41.66 % of the control group members and 10 to 20 years in 25% of the experiment group and 58.33% of control group. It was beyond 20 years in 33.3% of the experimental group members. The spouse’ literacy level of 8.3% of members in both experimental and control groups was under diploma while 25% of wives in the experimental group and 16.7% of control groups had a diploma license. Around 25% of control group had an associated degree and 33% of both groups had an education degree of B.Sc. About 16.7% of the experimental group and 8.3% of the control group have been graduated with M.Sc. degree. A small proportion of 8.3% of wives in control group had a specialist degree. The number of children was another characteristic polled in this study. Based upon the obtained results, 25% of the experimental group and 8.3% of the control group belonged to families without children. 8.3% of the experiment group and 16.7% of the control group was of one-child families. About 41.7% of experimental group and 33.3% of the control group had two children while 8.7% of the experimental group and 3 3.3% of the control group had three children and 16.7% of both groups had four children. It is worth noting that 83.3% of marriages in the control and experimental groups had been married through traditional customs and 16.7% of marriages in both groups were based on acquaintance before marriage. Sexual function data analysis results In this research, first of all, the sexual function equality of experiment and control groups were tested by “t-test. Prior to running the t-test, the equality condition of variances was examined by Levine Test, as the first necessary step. The P-value of greater than 0.05 and the significant level of 95% revealed that the variances of two groups were equal. In other words, the sexual function of both groups is equal. Table 1 gives Lewin Test for checking equality of variances. As regards, there were two independent groups with pre- and post- tests for analyzing the scores. The difference of scores was calculated by subtracting the pre-test and post-test scores for each subject. Subsequently, the average of subtracted scores was investigated using parametric tests. To that end, the required conditions of parametric tests should initially be tested. In other words, the samples are to be selected randomly and each sample must be chosen independently from the other subjects. The scores must have a normal distribution and two population variances must be equal (homogeneity of variances or equality of variances).
|
|
4. Conclusions
- This is a semi-experimental research on 30 females aged between 20-40 years old. The females received interventional trainings in 10 sessions within two months. The obtained results revealed that sex therapy with cognitive-behavioral approach would be helpful in treatment of orgasmic disorder. The research was conducted on two control and experimental groups. Some strategies are suggested as follow:- Training couples the skills of talking about their sexual expectations and criticism- Holding audio - visual and written forms of sexual training courses for free- Mandatory sexual coursework at universities In this respect, it is suggested to investigate effectiveness of integrated cognitive-behavioral approach and psychoanalysis in resolving orgasmic dysfunctions in men and women.