Md. Nurul Islam 1, Md. Golam Hossain 1, Md. Rezaul Karim 2, Md. Rafiqul Islam 3, Pete E. Lestrel 4, Md. Ashraful Islam 2
1Professor, Department of Statistics, University of Rajshahi, Rajshahi-6205, Bangladesh
2Research of Health Researcher group, Department of Statistics, University of Rajshahi, Rajshahi-6205, Bangladesh
3Professor, Department of Population Science and Human Resource Development, University of Rajshahi, Rajshahi-6205, Bangladesh
4Emeritus Professor, Sections of Orthodontics and Oral Biology, School of Dentistry, University of California, Los Angeles, California 90024-1668, USA
Correspondence to: Md. Rafiqul Islam , Professor, Department of Population Science and Human Resource Development, University of Rajshahi, Rajshahi-6205, Bangladesh.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
Abstract
In this paper we attempted to modify Bongaarts' model considering all fetal wastage for estimating approximately true value of TFR. Also, it was found the effect of proximate variables on change the level of fertility during 1975 to 2007 in Bangladesh. For this study, data were extracted from Bangladesh Contraceptive Prevalence Surveys, Bangladesh Fertility Surveys and Bangladesh Demographic and Health Surveys. Proximate determinants influence the level of fertility in a society. Bongaarts' model is a well known approach for studying proximate determinants for total fertility rate (TFR) of a society. Only induced abortion as one of the proximate variable is considered in Bongaarts' model for estimating proximate determinants of fertility, though the other possible factors like miscarriage and stillbirth are also important for fertility. The TFR was estimated by revised model was more close to observed TFR (R2=0.98) than TFR calculated by Bongaarts' original model (R2 = 0.84). Moreover, only abortion (Bongaarts' model) put contribution to change TFR approximately 1 birth while all fetal wastage (revised Bongaarts' model) change TFR approximately 1.40 birth per women. This study demonstrates that all proximate indices shows decreasing tendency over time. The results suggest that revised Bongaarts’ model more accurately estimate TFR than original Bongaarts' model.
Keywords:
Proximate Determinants, Revised Bongaarts' Model, Proportion Married Contraception, Fetal Wastage, Lactational Infecundability
Cite this paper: Md. Nurul Islam , Md. Golam Hossain , Md. Rezaul Karim , Md. Rafiqul Islam , Pete E. Lestrel , Md. Ashraful Islam , Fertility Analysis of Bangladesh Population Using the Revised Bongaart’s Model, Advances in Life Sciences, Vol. 4 No. 2, 2014, pp. 44-51. doi: 10.5923/j.als.20140402.02.
1. Introduction
The study of determinants of human fertility is a very complex process. Human fertility influence population growth, which has consequences such as pressure on resource, employment situations, health and other social facilities as well as savings and investment. Such consequences, in turn, bearing on the socio-demographic and socio-economic variables that affect fertility behavior. The level of fertility in a society is directly influenced by a set of variables called intermediate variable or proximate determinants [1]. In general, the biological and behavioral factors through which socio-demographic, socio-economic, cultural and environmental variables affect fertility, called intermediate fertility variables. Since fertility is the resultant of multiplicity of factors, studies have attempted to identify these factors, which have important bearing for policy intervention on altering the level of fertility [2, 3, 4, 5, 6].Bongaarts' revised the original classification given by Davis and Blake [1] and provided a simple analytical method, which permitted a quantitative assessment of the contribution of different proximate determinants to give fertility levels or change. Bongaarts [7] demonstrated that most of the variation in fertility is due to four intermediate variables or proximate determinants. These are: (i) proportion married, (ii) contraception, (iii) induced abortion and (iv) lactational infecundability. Historical studies about fertility change have shown that as societies begin to undergo the transformation from natural to deliberately controlled fertility, significant changes in the overall levels of total natural fertility, total marital fertility and total fertility also begin to occur [8]. Changes can be traced to one or more proximate determinants, such as, an increase in contraceptive use for stopping and spacing purposes, a rise in age at first marriage, a decline in the proportion married, prolonged breastfeeding, and induced abortion. Among many of researchers [9, 10, 11] using data derived from Bangladesh Fertility Survey and Bangladesh Demographic and Health Survey, investigates the impact of four intermediate fertility variables--namely marriage, contraception, lactational infecundability and induced abortion on fertility in Bangladesh. The contribution of each proximate variable was observed through the decomposition of the total fertility rate (TFR) into proximate components. Contraception is seen to be the most prominent determinant in lowering the total fertility rate [11, 12].Fertility decline has been endorsed to rapid socioeconomic development and influenced only on fertility through the intermediate variables. Application of Bongaarts' model on Peninsular Malaysian data indicates that marriage postponement and contraceptive use are the two most important proximate determinants of fertility, but the effects are not uniform across the ethnic groups [13]. Findings also suggested that, postpartum infecundability and abortion also play a part in explaining ethnic fertility differentials. The fertility inhibiting effects of these proximate determinants have significant implications on reproductive health and future population growth [13].Bongaarts' proposed the classical proximate determinants of fertility framework using the 2003 Reproductive Health Survey of Mongolia data for applied in order to analyze which factors shape period fertility and found that the importance of induced abortion in the determination of fertility level has reduced and that the use of modern contraception has increased progressively and contributed most in determining fertility level [14].However, it is suggested that Bongaarts' model for proximate determinants of fertility gives over estimate the fertility rate (TFR), because in the model he considered only induced abortion in computing the index of induced abortion as one of the proximate determinants of fertility. Consequently, in this paper we attempt to revise Bongaarts' model which gives approximately true estimate of the TFR. While it is true that induced abortion has direct impact on fertility, the other fetal wastage categories; namely, miscarriage and stillbirth also direct impact on fertility. So, we considered all fetal wastage including induced abortion for computing the index instead of only induced abortion which we termed as index of fetal wastage. Also, to improve our understanding of fertility change, we critically examine the effect of major proximate determinants: (i) proportion married, (ii) contraception, (iii) all fetal wastage (iv) lactational infecundability.
2. Sources of Data of This Study
Data were derived from Bangladesh Contraceptive Prevalence Surveys 1979, 1981, 1983, 1985; Bangladesh Fertility surveys 1975, 1989 and Bangladesh Demographic and Health Surveys 2000, 2004 and 2007. All these surveys are nationality representative and the data provided by these surveys are of good quality.
3. Methods and Methodological Issues
3.1. Bongaarts' Model
To quantify the fertility inhibiting effect of the four major proximate determinants, Bongaarts [15] developed a model, which is now widely used in fertility analysis. Bongaarts' model estimating the effect of different proximate determinants assumes that the natural reproductive capacity (that is, total fecundity rate, TF) of women is nearly the same for all women, but their actual reproductive performance is modified by four major proximate determinants. In this model Bongaarts' [15] expressed total fertility rate (TFR) as the product of four indices measuring the fertility inhibiting effect of these four indices and the fecundity rate (TF). The TF is the average number of live births expected among women who during their entire reproductive period remain married, do not use contraception, do not have any induced abortion and do not breastfeed their children [7]. According to Bongaarts' model, the TFR can be written as: | (1) |
where, Cm is the index of proportion married  Cc is the index of non-contraception
Cc is the index of non-contraception Ca is the index of induced abortion, and
Ca is the index of induced abortion, and  Ci is the index of lactational infecundability.The estimation procedure of the indices is given bellow:
Ci is the index of lactational infecundability.The estimation procedure of the indices is given bellow:
3.2. Index of Proportion Married (Cm)
The index of proportion married is estimated by the equation | (2) |
where m(a) is the age-specific proportion of females currently married and g(a) is the age-specific marital fertility rate.
3.3. Index of Non-contraception (Cc)
The index non-contraception Cc can be estimated as: | (3) |
where, u is the proportion currently using contraception among married women of reproductive age (average of age specific use rate), e is the average contraceptive effectiveness and a value for s = 1.08 (Sterility correction factor) obtained by Henry [16].
3.4. Index of Induced Abortion (Ca)
Although reliable measurements of the prevalence of induced abortion in many societies, even in cases where good estimates are available, it has proven difficult to determine abortion. Estimates of number of birth averted by induced abortion are largely based on numerical exercise using mathematical reproductive models. The most detailed studies of this topic have been made by Potter [17], whose work has demonstrated the following:In the absence of contraception, an induced abortion averts about 0.4 births, while about 0.8 births are averted when moderately effective contraceptive is practiced. To generalize from these findings, the births averted per induced abortion (B), may be estimated with the following equation: | (4) |
A convenient overall measure of the incidence of induced abortion is provided by the total abortion rate (TA), equal to the average number of induced abortions per woman at the end of the reproductive period. The reduction in fertility associated with a given level of total abortion rate is calculated as: | (5) |
Where, A equals the average number of birth averted per woman by the end of the reproductive years. The index of induced abortion is defined as the ratio of the observed total fertility rate (TFR) to the estimated total fertility rate with induced abortion, TFR+A; that is  | (6) |
The index Ca equals the proportion by which fertility is reduced as the consequence of the practice of induced abortion (Note that Ca decline with increasing incidence of induced abortion).
3.5. Index of Lactational Infecundability (Ci)
In modern western population, lactation is generally short and many women do not lactate at all. In traditional societies in Africa, Latin America and Asia, lactation is usually long and lasts until the next pregnancy occurs. Lactation has an inhibition effect on fertility and thus increases the birth interval and reduces natural fertility [18]. A typical average birth interval without lactation can be estimated to be 18.5 months [19]. The ratio of the average birth intervals without and with lactation, which measure the index of lactational infecundability and given by | (7) |
where, i is the average duration (in months) of infecundability from birth to the first post-partum ovulation (menses). An indirect estimate of i as developed by Bongaarts' is given by | (8) |
where, B is the average duration of breastfeeding in months.
3.6. Revised Bongaarts' Model
In Bongaarts' model, we replace one index which is the index of fetal wastage instead of the index of induced abortion. The other indices remain same as given by Bongaarts'.In proposed model, we considered all miscarriage or all fetal wastages (miscarriage, abortion and stillbirth) taking together in computing the index, because the index of miscarriage or fetal wastage have direct impact on fertility. The index may be termed as index of fetal wastage and indicated as Cfw.. Then the proposed model becomes | (9) |
Where, the index of fetal wastage is defined as the ratio of the observed total fertility rate to the estimated total fertility rate with all fetal wastage which is (TFR+AFW) that is | (10) |
Where AFW equals the average number of birth averted per woman by the end of the reproductive years for all fetal wastage and which is estimated by  . Here TFW is the total fetal wastage rate and which is average number of fetal wastage per woman at the end of the reproductive years.
. Here TFW is the total fetal wastage rate and which is average number of fetal wastage per woman at the end of the reproductive years.
3.7. Magnitude of the Fertility Inhibiting Effect Being Accounted for Each Proximate Determinant
The difference between the total fecundity rate (TF, taken as 15.30 in 2007) and the estimated TFR is attributed result of the inhibitory effect of each variable. The total inhibiting effect is prorated by the proportion of the logarithm of each index to the sum of logarithm of all indices  | (11) |
 | (12) |
 | (13) |
 | (14) |
 | (15) |
3.8. Decomposition of the Change in Fertility and Contribution of Proximate Variables
The proposed model given by the equation can easily be turned to a decomposition equation that allows the quantification of the contribution made by each of the four intermediate fertility variables to an observed change in fertility between two time points 0 and t. The basic equation is as follows: | (16) |
Considering two time points 2004 and 2007, we can write as: | (17) |
where  | (18) |
 | (19) |
 | (20) |
 | (21) |
 | (22) |
 | (23) |
The relationship becomes | (24) |
Here, I represent an interaction factor. This equation simply states a given proportional change in the TFR between 2004 and 2007 is equal to the sum of the proportional changes due to the different intermediate fertility variables plus an interaction term. The decomposition procedure for the TFR can easily extend to allow the decompositions of a change in the crude birth rate (CBR). The CBR is linked to its proximate determinants by the following equation: | (25) |
Where, S is an age-sex composition term calculated by | (26) |
Again, | (27) |
 | (28) |
Then it becomes | (29) |
Where, Pm, Pc, Pfw, Pi, and Pr were described earlier.
4. Results and Discussion
4.1. Estimated Proximate Variables and Implications
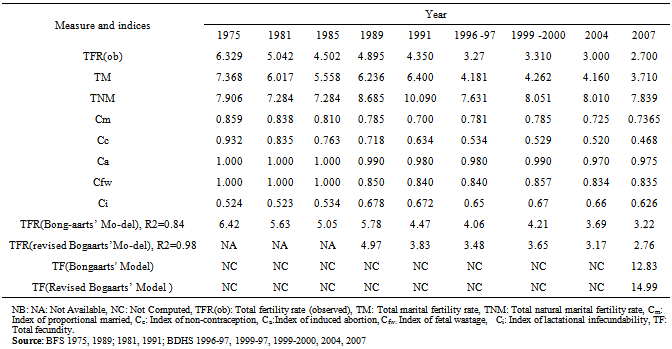
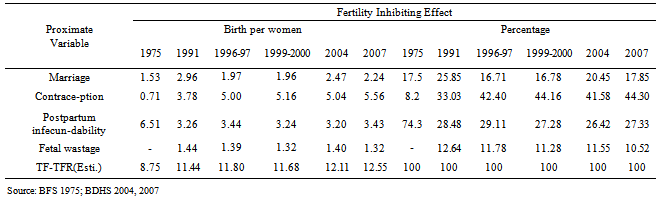
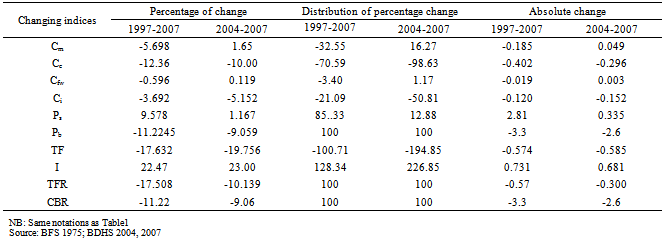
On the basis of the models given in equations (1) and (9), the estimated values of the measures and indices for different time points are presented in table 1. The complement of the indices represents the proportionate reduction in fertility attributed to the fertility determinant. The lower the estimated value of the indices, the greater the fertility reducing effect. The value of Cm in year 1975, 1981, 1985, 1989, 1991, 1996-97, 1999-2000, 2004 and 2007 are 0.859, 0.810, 0.785, 0.700, 0.781, 0.785, 0.725 and 0.736, respectively. These results indicate that the proportion of married women reduces fertility by 14.1%, 16.2%, 19.0%, 21.5%, 30.0%, 21.9%, 21.5%, 27.5% and 26.3% for year 1975, 1981, 1985, 1989, 1991, 1996-97, 1999-2000, 2004 and 2007, respectively. The contraceptives (Cc) reduces fertility by 6.80%, 16.5%, 23.7%, 28.2%, 36.6%, 46.6%, 47.1%, 48.0% and 53.2% for year 1975, 1981, 1985, 1989, 1991, 1996-97, 1999-2000, 2004 and 2007, respectively. The reducing fertility impact of contraceptive on fertility varies from one time point to another because of varying use and effectiveness of methods. In recent years, the results of increased use of contraceptive method, the fertility reducing impact of contraceptive also increased. Induced abortion reduces fertility by 1.0%, 2.0%, 2.0%, 1.0%, 3.0% and for 1989, 1991, 1996-97, 1999-2000, 2004 and 2007, respectively. However, all fetal wastages (Cfw) reduces fertility by 15.0%, 16.0%, 16.0%, 14.3%, 16.6% and 16.5 for 1989, 1991, 1996-97, 1999-2000, 2004 and 2007, respectively. We observe that reduces fertility by all fetal wastages (Cfw) is higher than that of by induced abortion (Ca) for each year. Again, the value of Ci in 2007 is 0.626 indicate that the average estimated effect of lactational infecundability for the reduction in fertility by 37%, compared with the value of Ci in 1999-2000 is 0.670 which indicates that the average estimated effect is 33%. It is clear that there is a downward trend in Cc and Cm, which shows an increasing effect in reducing fertility by the indices.Table 1 also exhibits the estimated value of TFR calculated by original Bongaarts' model and our revised model. We observe that original model gives the over estimate of TFR and difference from observed value, while the estimated value of TFR by revised model is very close to observed value for each year. Again, considering only induced abortion in Bongaarts' model, the calculated TF is 12.83, which is also away from assumed TF, while revised model estimate the value of TF is 14.99, which is very close to observed TF (15.3). Moreover, revised model can more explain (R2 = 0.98) the variation of TFR among surveyed years than that of original model (R2 = 0.84). These results demonstrate that our revised model is better than original Bongaarts' model for estimating fertility level.Trend in the magnitude of the inhibiting effect being accounted for proximate variable at different time points are presented by Table 2. The results indicate that a total of 8.75 births in 1975 being inhibited, 1.53 births are due to effect of marriage variable, 0.71 are due to contraception and 6.51 are due to postpartum infecundability. A total of 12.11 births in 2004 being inhibited of which 2.47 births are due to effect of marriage variable, 5.04 are due to contraception, 3.20 are due to postpartum infecundability and 1.40 are due to fetal wastage. A total of 12.55 births in 2007 being inhibited of which 2.24 births are due to effect of marriage, 5.56 births are due to contraception and 3.43 births are due to postpartum infecundability, and 1.32 births are due to fetal wastage. The inhibiting of proportion married index, which is more or less continuously increasing from a level of 1.53 births per-woman in 1975 to 2.24 in 2007. Again, the effect of contraceptive use increased from 0.71 births per-women in 1995 to 5.56 births per-woman in 2007. In contrast, the effect of postpartum infecundability decreased during the period from 1975 to 2007. Again, effect of fetal wastage has not changed very much during the period (Table 2).Table 3 represents the values of the decomposition of change by all indices in TFR between 1997-2007 and 2004-2007. It indicates that TFR has declined about 17.51% from 3.27 in 1997 to 2.7 in 2007. Again it declined about 10.14% from 3.00 in 2004 to 2.7 in 2007. This indicates that the decomposition of this decline in TFR between 1997 to 2007 is nearly 5.69% due to change in proportion married, about 12.36% decline due to increased use of contraceptive and effectiveness, while about 0.596% decrease due to increase the index of fetal wastage. Again approximately 3.69% decrease due to increase of the duration of lactational infecundability. The remaining proximate determinants together contribute 22.47% decrease and 17.67% increase in TFR due to the interaction factor.Table 1. Estimated different reproductive measures and indices of fertility, Bangladesh 1975-2007
 |
| |
|
Table 2. Trends in the magnitude of the total fertility inhibiting effect being accounted for proximate variables
 |
| |
|
Table 3. Decomposition of changes in TFR & CBR by different measures and indices, Bangladesh 1997 to 2007
 |
| |
|
Again, the decomposition in TFR between 2004-2007 has been 1.65% increases due to change in the proportion married, about 10% decline due to increased use of contraceptive. During the period 0.12% increase due to decrease of fetal wastage, a dramatic change about 5.15% decline due to increase the duration of lactational infecundability. The remaining proximate determinants together contribute about 19.76% decreases and the interaction factor contribute 23% increase.The decomposition results are standardized to add to 100%. Further, table 3 indicate that during 1997 to 2007, it has declined 0.57 births per-woman of which 0.185 births declined by proportion married, 0.402 births declined due to contraceptive use, 0.019 birth declined due to fetal wastage, and 0.120 births decreased due to lactational infecundability. Lastly, 0.574 births declined by other proximate determinants and the interaction factor increased by 0.731 births per-woman.Again, during 2004 to 2007, it has declined by 0.30 births per-woman of which 0.049 births has increased by proportion married, 0.296 births decline due to contraceptive use, 0.003 births increased due to fetal wastage, and 0.152 births declined due to lactational infecundability. Again 0.585 births declined by other proximate determinants, and interaction factor contribute 0.681 births. It is clear from table 3 that fertility is declining by proportion married, which made a significant contribution to the overall fertility reduction, and the contraceptives have the highest impact on reducing fertility which may be attributed to the increase use of contraception from 7.3% in 1975 to 58.1% in 2004 and 55.8% in 2007 [20].
5. Conclusions
Findings of the study clearly indicate that there is a downward trend in all the proximate indices. Between 1997 and 2007, the amount of decrease in the total fertility rate is about 17% and about 10% from 2004 to 2007. This is primarily caused by an increase in the use and effectiveness of contraception. Again comparison among the observed and estimated values by the original Bongaarts' model and revised Bongaarts' model, we conclude that the revised model is better than original model. It is hoped that, revised model may use for further research in fertility analysis.
ACKNOWLEDGEMENTS
The authors would like to thank the Bangladesh Contraceptive Prevalence Surveys (BCPS), Bangladesh Fertility Surveys (BFS) and Bangladesh Demography and Health Survey (BDHS) for providing nationally representative data for several years. All authors declared that there were no conflicts of interests in relation to this study.
Conflict of Interest
All authors declared that there were no conflicts of interests in relation to this study.
References
| [1] | Davis, K., and Blake, J., 1956, Social Structure and Fertility: An Analytic Framework, Economic Development and cultural Change, 4(3), 211-235. |
| [2] | Heer, David M., 1966, Negro-white marriage in the United States, Journal of Marriage and the Family, 28, 262-273 |
| [3] | Cain, G.G., and Weininger, A., 1973, Economic determinants of fertility: results from cross-sectional aggregate data, Demography, 10(2), 205-223. |
| [4] | Edith-Jane Bahr, ‘Help, Please’ Knopf Doubleday Publishing Group, New York City, United State, ISBN-10: 038509776X | ISBN-13: 9780385097765, 1975. |
| [5] | Defranzo, J., 1976, Cross-sectional areal analyses of factors affecting marital fertility: actual versus relative income, Journal of Marriage and Family, 38(4), 669-676. |
| [6] | Kohli, K.L., 1977, Regional variations of fertility in Iraq and factors affecting it, Journal of Biosocial Science, 9(2), 175-182. |
| [7] | Bongaarts, J., 1982, The fertility-inhibiting effects of the intermediate fertility variables, Studies in Family Planning, 13(6-7), 179-189. |
| [8] | Bongaarts. J, and G.R. Potter, Fertility, Biology and Behavior: An Analysis of the Proximate determinants, Academic press, New York, 1983. |
| [9] | Islam, M.N., Trends and correlates of marriage and fertility in Bangladesh, Unpublished Ph.D. Dissertation, Department of Statistics, University of Rajshahi, Bangladesh, January, 1996. |
| [10] | Islam, M.N., and Islam, M.M., 1993, Biological and behavioural determinants of fertility in Bangladesh: 1975-1989, Asia Pacific Population Journal, 8 (1), 3-18. |
| [11] | Kabir, M. and A.K.U. Rob, Fertility and its proximate determinants, in: M. BadrudDuza (ed.), South Asia Study of Population Policy and Programmes, Bangladesh, (Dhaka, UNFPA), 1990, pp. 53-86. |
| [12] | Abedin, S., and Islam, M.N., 1994, Implication of Contraceptive practice of future trends in fertility in Bangladesh, Jonural of Family Welfare, 40(3), 37-41. |
| [13] | Tey N.P., Ng S.T., and Yew S.Y., 2012, Proximate determinants of fertility in peninsular Malaysia. Asia Pac J Public Health, 24 (3), 495-505. PMID: 21490114 |
| [14] | Spoorenberg, T., 2009, Changes in the proximate determinants of fertility decline in post-socialist Mongolia, J Biosoc Sci., 41(5), 607-624. doi:10.1017/S0021932009003459. |
| [15] | Bongaarts, J., 1987, The proximate determinants of exceptionally high fertility, Population and Development Review, 13 (1), 133–139. |
| [16] | Henry L., Some data on natural fertility, Taylor & Francis online, Eugenics Quarterly, 8(2), 81-91, 1961. |
| [17] | Potter, R.G., 1976, Additional births averted when abortioil is added to contraception, Studies in Family Planning, 7(8), 224-230. |
| [18] | Potter, R.G. Jr., Wyon J.B., Parker M, and Gordon J.E., 1965, A Case Study of Birth Interval Dynamics, Population Studies, 19(1), 81-96. |
| [19] | Chen, L.C., Ahmed, S., Gesche, M. and Mosley W.H., 1974, A Prospective Study of Birth Interval Dynamics in Rural Bangladesh, Population Studies, 28(2), 277-297. |
| [20] | National Institute of Population Research and Training (NIPPORT), Bangladesh Demographic and Health Survey Dhaka, Mitra & Associates and ORC Macro, Bangladesh and Calverton, MD, USA, 2009. |
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML