-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(6): 2964-2968
doi:10.5923/j.ajmms.20261606.38
Received: May 7, 2026; Accepted: Jun. 3, 2026; Published: Jun. 9, 2026

Features of Pregnancy Course in Primiparous Women Primiparous Women as a High Obstetric Risk Group: A Systematic Review and Meta-Analysis
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLL. R. Agababyan, A. T. Akhmedova
Samarkand State Medical University, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Objective. To synthesize current evidence on the course of pregnancy, delivery characteristics, postpartum recovery, and complications in primiparous women, and to identify clinically meaningful patterns relevant to risk stratification, intrapartum management, and postpartum follow-up. Methods. A structured literature review of studies published in 2004-2025 was performed using open bibliographic sources and journal webpages. Eighteen studies published in Scopus-indexed journals were included. Owing to heterogeneity of designs and outcomes, the manuscript was prepared as a systematic review with a meta-analytic synthesis of effect direction and magnitude rather than as a single pooled estimate across all endpoints. Results. Nulliparity is consistently associated with higher rates of hypertensive disorders, placenta-mediated complications in high-risk cohorts, spontaneous preterm birth in selected low-risk cohorts, prolonged labour, operative vaginal delivery, cesarean delivery in many routine-care settings, postpartum haemorrhage, and slower early recovery after cesarean birth. However, the effect of labour induction is context-specific: observational cohorts showed higher cesarean rates after induction, whereas the ARRIVE randomized trial demonstrated a lower cesarean rate with elective induction at 39 weeks in low-risk nulliparous women. Conclusion. Nulliparity should be considered an independent modifier of obstetric risk. Clinical care in first pregnancy should prioritize early screening for placenta-mediated disease, tailored decisions on the timing of labour induction, prevention of prolonged labour and postpartum haemorrhage, and individualized monitoring in the early postpartum period.
Keywords: Primiparous women, Nulliparous, Primiparity, Pregnancy, Delivery, Postpartum period, Complications, Cesarean section, Postpartum haemorrhage
Cite this paper: L. R. Agababyan, A. T. Akhmedova, Features of Pregnancy Course in Primiparous Women Primiparous Women as a High Obstetric Risk Group: A Systematic Review and Meta-Analysis, American Journal of Medicine and Medical Sciences, Vol. 16 No. 6, 2026, pp. 2964-2968. doi: 10.5923/j.ajmms.20261606.38.
1. Introduction
- First pregnancy and first childbirth remain central topics in modern obstetrics because primiparous women account for a substantial share of primary cesarean sections, prolonged labour, operative vaginal births, postpartum haemorrhage, and a portion of severe placenta-mediated complications. The international literature more often uses the term nulliparous as an operational definition for a woman who has not had a previous birth beyond the threshold of fetal viability; in practical obstetric use, this is close to the concept of a primiparous woman.The clinical significance of this issue is determined not only by the higher probability of intrapartum interventions during first birth, but also by the fact that the outcome of the first pregnancy largely shapes a woman's future obstetric trajectory. Primary cesarean section, severe preeclampsia, massive postpartum haemorrhage, birth trauma, and an unfavourable postpartum recovery experience may influence both reproductive behaviour and the risk profile of subsequent pregnancies.Despite the large number of publications, data on primiparous women remain heterogeneous. Some studies demonstrate increased risks of operative delivery and complications, whereas others emphasize the context-dependent nature of these effects, for example, elective induction at 39 weeks in low-risk nulliparous women. For some outcomes, the effect of parity is non-monotonic. This requires a careful synthesis of evidence without excessive simplification.Aim of the StudyTo systematize and critically summarize the literature on the course of pregnancy, characteristics of delivery, the early postpartum period, and complications in primiparous women, and to formulate practical conclusions for clinical management and scientific publication.
2. Material and Methods
- Study design: a systematic literature review with meta-analytic synthesis of effect direction and comparable quantitative indicators. The search covered publications from 2004 to 2025 using PubMed/PMC, publishers' websites, and journal profiles in order to identify articles published in journals indexed in Scopus. Cohort studies, population registries, prospective observational studies, and randomized clinical trials were eligible.Inclusion criteria were as follows: (1) studies of primiparous, nulliparous, or first-birth cohorts; (2) analysis of at least one domain of interest, namely pregnancy course, delivery, postpartum recovery, or postpartum complications; (3) baseline data or conclusions applicable to obstetric practice; and (4) publication in a journal listed in Scopus/SCImago or identified on the publisher's website as Scopus-indexed. Publications with irrelevant populations, duplicate samples without new findings, and studies lacking meaningful data on outcomes in primiparous women were excluded.The final evidence base comprised 18 studies. Because of differences in design, populations, outcome definitions, and statistical models, a single pooled estimate for the entire set of outcomes was not calculated. Instead, a domain-based synthesis was performed, focusing on effect direction, magnitude of association, clinical interpretation, and the consistency of the observed pattern.
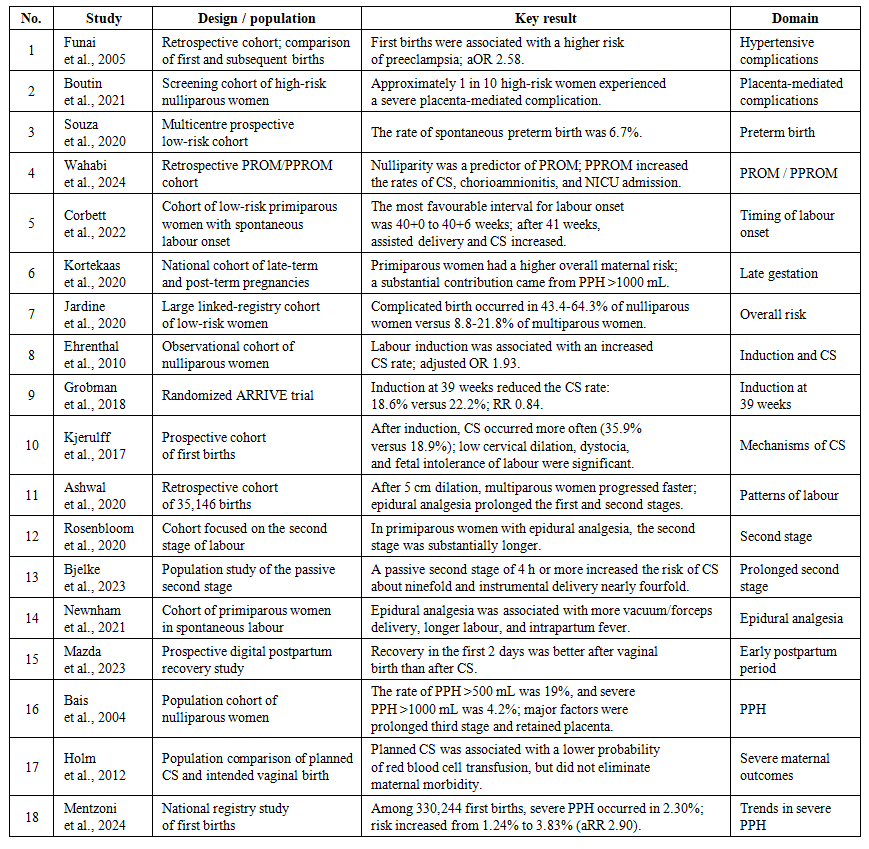 | Table 1. Characteristics of Included Studies |
3. Results
- 1. Features of Pregnancy Course in Primiparous WomenThe most consistent association in the reviewed literature is the link between nulliparity and hypertensive as well as placenta-mediated complications. In the retrospective cohort reported by [1] the risk of preeclampsia in first births was more than 2.5 times higher than in subsequent births. This finding accords with current concepts of immunologic and placental adaptation as one possible explanation for the greater frequency of hypertensive complications during the first gestation.Screening data from [2] indicate that risk is not uniform even within the primiparous population. Among nulliparous women classified as high risk by prenatal screening algorithms, approximately 10% developed severe placenta-mediated complications. In practical terms, this means that first pregnancy should not be treated as a homogeneous category; earlier differentiation into low-risk and high-risk subgroups is necessary.In the multicentre low-risk cohort of [3] the rate of spontaneous preterm birth was 6.7%. Although this figure cannot be directly generalized to every population, it emphasizes that even clinically healthy primiparous women retain a measurable burden of adverse outcomes requiring antenatal monitoring.Rupture of membranes and timing of labour onset also deserve special attention. In the study by [4] nulliparity was identified as one of the predictors of PROM, while PPROM was associated with increased cesarean delivery, chorioamnionitis, longer hospitalization, and higher rates of neonatal intensive care admission. In the study by [5] the most favourable profile for low-risk primiparous women was observed when spontaneous labour began at 40+0 to 40+6 weeks, whereas after 41 weeks rates of assisted vaginal birth, cesarean section, and low Apgar scores increased.It is important to note that the effect of parity is not uniformly linear across all complications. Contemporary large cohorts emphasize an outcome-specific pattern: for some complications the unfavourable profile is more pronounced in nulliparity, whereas for others it increases with higher parity. Therefore, the formula 'first pregnancy equals maximum risk for all outcomes' is methodologically incorrect.2. Features of Delivery in Primiparous WomenAt the stage of delivery, primiparous women account for much of the burden of complicated labour and primary cesarean section. In the large population analysis by [7] among women without previously recognized risk factors, complicated birth occurred substantially more often in nulliparous than in multiparous women. This is particularly important because even a formally low-risk status does not eliminate the specific features of first birth.Labour induction remains one of the most debated issues. Observational studies by [8] and [10] showed higher cesarean section rates after induction. At the same time, [10] demonstrated that a considerable part of this association is mediated by intrapartum factors such as low cervical dilation at admission, dystocia, and signs of fetal intolerance of labour. In other words, induction is often not the sole cause but rather one component of a more complex intrapartum scenario.In contrast, the randomized ARRIVE trial showed that in low-risk nulliparous women, elective induction at 39 weeks may be associated with a lower cesarean section rate without worsening the main neonatal composite outcome. Thus, the effect of induction depends on the precise clinical context, selection criteria, and organizational model of labour management; the blanket statement that induction in primiparous women always increases the cesarean section rate is not supported by the overall evidence.Labour progress in primiparous women is characterized by greater duration and greater sensitivity to interventions. According to [11] after 5 cm of cervical dilation, labour accelerated faster in multiparous women, whereas in nulliparous women the pace remained slower. Epidural analgesia prolonged both the first and second stages of labour. Additional studies showed that when the passive second stage lasted 4 hours or longer, the probability of cesarean section and instrumental vaginal delivery increased sharply.The work of [14] complements this picture: in primiparous women with spontaneous labour, epidural analgesia was associated with more vacuum and forceps deliveries, longer first and second stages, higher intrapartum temperature, and more frequent antibiotic use. These findings do not imply that epidural analgesia should be avoided, but they do require appropriate patient counselling and closer monitoring of labour progress.3. Early Postpartum Period and ComplicationsThe early postpartum period in primiparous women cannot be regarded as clinically simple. According to the digital prospective study by [15] women who had spontaneous vaginal birth recovered better during the first 48 hours than women who underwent cesarean section, and convergence of recovery indicators occurred only by days 3 to 4. Consequently, the mode of delivery in a primiparous woman shapes not only the intrapartum course but also the early functional postpartum profile.The most important complication of the postpartum period remains postpartum haemorrhage. In the cohort described by [16] among nulliparous women the rate of PPH exceeding 500 mL was 19%, while severe PPH over 1000 mL occurred in 4.2%. The key determinants were a prolonged third stage and retained placenta. More recent national data from [18] indicate that severe PPH was recorded in 2.30% of first births, with a clear increase in risk over the study period.The findings of [17] show that even if planned cesarean delivery reduces some severe outcomes, this does not alter the general principle: prevention of obstetric morbidity in primiparous women should not be built around a single procedure, but around optimization of the entire intrapartum scenario - from selecting the timing of induction to preventing uterine atony, ensuring active management of the third stage, and promptly detecting retained placenta.Taken together, these data indicate that primiparous women constitute a distinct clinical group in which the early postpartum period is closely linked to the course of labour: the duration of the second stage, the frequency of operative interventions, the method of analgesia, and the presence of blood loss all directly influence early functional recovery.
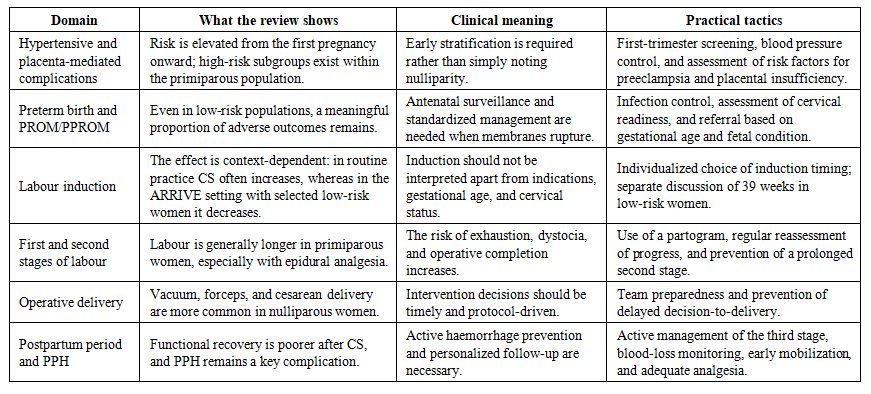 | Table 2. Integrated Clinical Profile of the Primiparous Woman: Risk Domains and Practical Implications |
4. Discussion
- The findings support several key propositions. First, primiparous women do not merely experience longer labour more often; they truly have a distinct obstetric risk profile that includes hypertensive complications, a higher probability of complicated birth, operative vaginal delivery, and postpartum haemorrhage. Second, for some interventions - most notably labour induction - the effect in primiparous women is determined not only by the procedure itself, but also by patient selection, gestational age, cervical status, and the organization of intrapartum care.It is important to avoid overgeneralization. Nulliparity increases the risk of several outcomes, but not all without exception. Moreover, within the primiparous population there are both high-risk and low-risk subgroups. The scientifically sound conclusion is that nulliparity should be interpreted as an independent risk modifier that requires contextual assessment alongside age, body mass index, gestational age, cervical features, comorbidity, and obstetric management.From the standpoint of clinical practice, primiparous women constitute the priority group for prevention of primary cesarean section. This requires a balance between an unacceptably delayed operative decision and an excessively early move to intervention. Where labour is managed according to modern protocols and the woman is selected as low risk, elective induction at 39 weeks may be a rational option. Where the cervix is immature and an unfavourable cluster of factors is present, observational data indicate an increased risk of cesarean section.Practical Implications for the Obstetrician-Gynecologist• First pregnancy should be regarded as a distinct category of obstetric risk already at the stage of antenatal follow-up.• For primiparous women, early screening for preeclampsia and placenta-mediated complications, timely prevention of hypertensive disorders, and clear patient routing are especially important.• Labour induction in primiparous women should be discussed individually; its appropriateness depends on gestational age, cervical maturity, the induction protocol, and the baseline risk profile.• When epidural analgesia is used and labour progress slows, the dynamics of the first and second stages should be actively reassessed so that prolonged labour is recognized in time.• In the early postpartum period, the priorities are prevention and early detection of PPH, adequate pain relief, functional rehabilitation, and patient education.This manuscript was prepared as a systematic review with meta-analytic synthesis, but not as a single quantitative meta-analysis of one outcome. This is due to the clinical heterogeneity of the included studies: outcome definitions, timing of assessment, criteria for low and high risk, statistical models, and comparison groups all differed.Accordingly, the presented conclusions are especially robust with respect to the direction of associations and the clinical patterns observed. A strict pooled OR or RR for individual outcomes would require additional extraction of primary numerical data from the full texts, harmonization of outcomes, and a separate statistical analysis with forest plots, heterogeneity assessment, and publication-bias analysis.Before submission to a specific journal, it is advisable to adapt the abstract length, citation style, section structure, and figure/table limits to the official requirements of the target journal.
5. Conclusions
- Primiparous women are characterized by a specific and clinically meaningful obstetric risk profile. The available evidence confirms a higher probability of preeclampsia, a range of placenta-mediated complications, prolonged labour, operative delivery, and postpartum haemorrhage, as well as more difficult early recovery after cesarean section.At the same time, the effects of individual interventions, especially labour induction, are not universal and must be interpreted in the context of clinical selection and management protocol.Scientifically and practically, the most justified approach is to regard nulliparity not as a formal demographic characteristic, but as an independent risk modifier that requires personalized antenatal, intrapartum, and postpartum care.