-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(6): 2957-2963
doi:10.5923/j.ajmms.20261606.37
Received: May 7, 2026; Accepted: Jun. 6, 2026; Published: Jun. 9, 2026

Optimization of Management Tactics for Pregnant Women with Cervical Pathology
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLL. R. Agababyan, N. U. Rabbimova
Department of Obstetrics and Gynecology, Samarkand State Medical University, Samarkand, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Background. Cervical pathology during pregnancy includes HPV-associated squamous and glandular lesions, invasive cervical cancer, benign cervical conditions, and structural abnormalities such as short cervix and cervical insufficiency. Pregnancy creates diagnostic difficulties because physiologic cervical changes can resemble pathology; at the same time, antenatal care provides an important opportunity to identify women who are overdue for screening and to prevent missed invasive disease. Objective. To synthesize current evidence and guideline recommendations and to propose an optimized, pregnancy-adapted management pathway for women with cervical pathology. Materials and methods. A narrative literature review was performed using international guidelines and peer-reviewed publications from WHO, ASCCP, ACOG, SMFM, ESGO/ESTRO/ESP, ESGO/INCIP, PubMed-indexed articles, and epidemiological reports relevant to Uzbekistan. Emphasis was placed on sources published from 2019 to 2025, while landmark studies were included when clinically relevant. Results. Pregnancy does not appear to accelerate the natural history of HPV-associated cervical precancer, and most CIN lesions can be managed conservatively once invasive cancer has been excluded. Risk-based triage, colposcopy by experienced specialists, avoidance of endocervical curettage, selective biopsy when clinically indicated, and structured postpartum follow-up are the core elements of safe management. High-grade lesions require surveillance during pregnancy, while treatment is generally deferred unless cancer is suspected. Invasive cervical cancer requires immediate multidisciplinary assessment in a gynecologic oncology and perinatal center. Structural cervical pathology requires a separate pathway based on obstetric history, standardized transvaginal cervical length assessment, progesterone therapy, and selective cerclage. Conclusion. Optimization of care for pregnant women with cervical pathology should combine oncologic safety, obstetric risk reduction, individualized counseling, and postpartum continuity. A unified clinical algorithm can reduce unnecessary invasive procedures while preventing delays in diagnosing clinically significant disease.
Keywords: Pregnancy, Cervical pathology, Cervical intraepithelial neoplasia, HPV, Colposcopy, Cervical cancer, Cervical insufficiency, Short cervix, Postpartum follow-up
Cite this paper: L. R. Agababyan, N. U. Rabbimova, Optimization of Management Tactics for Pregnant Women with Cervical Pathology, American Journal of Medicine and Medical Sciences, Vol. 16 No. 6, 2026, pp. 2957-2963. doi: 10.5923/j.ajmms.20261606.37.
Article Outline
1. Introduction
- Cervical pathology in pregnancy is a clinically heterogeneous concept. It may refer to abnormal cervical screening results, HPV-associated cervical intraepithelial neoplasia (CIN), adenocarcinoma in situ (AIS), invasive cervical cancer, benign inflammatory or vascular conditions, and structural cervical disorders associated with pregnancy loss or spontaneous preterm birth. These conditions differ in pathogenesis and urgency, but they share a central challenge: management must protect maternal health without causing avoidable fetal or obstetric harm.The problem is particularly relevant for countries with evolving cervical cancer prevention programs. According to the ICO/IARC HPV Information Centre, cervical cancer remains one of the leading cancers among women in Uzbekistan, with an estimated 1,887 new cases and 1,103 deaths annually in the 2023 country fact sheet [1]. Uzbekistan has also made important progress in HPV vaccination, including the introduction of HPV vaccination into the national immunization calendar in 2019 and high first-dose coverage among adolescent girls reported by WHO/Europe [2]. Nevertheless, vaccination benefits will take decades to fully affect cancer incidence in adult women, meaning that organized screening, quality colposcopy, and rational management of detected pathology remain essential.Pregnancy is not a contraindication to cervical screening when a woman is due or overdue for testing. However, pregnancy-related changes such as increased cervical vascularity, glandular eversion, mucus production, decidual reaction, and inflammation can complicate visual interpretation and may increase anxiety when contact bleeding or abnormal discharge is present. Therefore, the clinical objective is not aggressive treatment of all lesions, but accurate exclusion of invasive cancer, careful risk stratification, safe surveillance, and reliable postpartum completion of care.This narrative review was developed from guideline documents, consensus statements, and peer-reviewed studies on cervical pathology in pregnancy. The core sources were WHO cervical cancer prevention recommendations, ASCCP risk-based management guidelines and pregnancy-specific practice guidance, SMFM recommendations on short cervix and cerclage, ACOG guidance on cervical insufficiency, ESGO/ESTRO/ESP cervical cancer guidelines, and ESGO/INCIP guidance on gynecologic cancers during pregnancy [3-14]. Additional sources were included for epidemiology, natural history of CIN in pregnancy, obstetric outcomes after previous cervical treatment, and management of benign cervical lesions.Because the topic includes several clinical entities rather than one intervention, the review is organized by management pathway: screening and triage, colposcopy and diagnosis, management of CIN and AIS, suspected or confirmed invasive cancer, benign cervical conditions, and structural cervical pathology. The proposed optimization model is based on recurring principles across the literature: risk-based decision-making, minimizing unnecessary intervention, early referral for high-risk findings, and closing the postpartum follow-up gap.
2. Epidemiology and Clinical Significance
- HPV-associated disease remains the major oncologic component of cervical pathology. Persistent high-risk HPV infection is the necessary cause of most cervical cancers, and population-level prevention depends on vaccination, screening, triage, diagnosis, and treatment of precancer. In Uzbekistan, the 2023 ICO/IARC fact sheet estimated cervical cancer as the second most frequent cancer among women overall and among women aged 15-44 years [1]. This epidemiologic context supports the need to use antenatal visits as a quality-control point for identifying women who have missed routine screening.Pregnancy also intersects with prior cervical disease treatment. Women who have undergone excisional treatment for CIN or early invasive disease may have higher risk of spontaneous preterm birth, particularly when the excised cone depth is larger. Meta-analyses have reported a dose-response association between depth of cervical excision and adverse obstetric outcomes, although women with CIN may also have baseline risk factors for prematurity [15,16]. Thus, management of cervical pathology should consider both current disease and the obstetric consequences of previous cervical procedures.The clinical significance of cervical pathology in pregnancy can be summarized in three questions. First, is invasive cancer present or reasonably suspected? Second, if the lesion is preinvasive, what is the likelihood of progression before postpartum reassessment? Third, is the cervix structurally or functionally compromised in a way that increases risk of pregnancy loss or preterm birth? Optimized care requires that these questions be answered separately rather than treating all cervical findings as one disease.
3. Physiologic Cervical Changes During Pregnancy and Differential Diagnosis
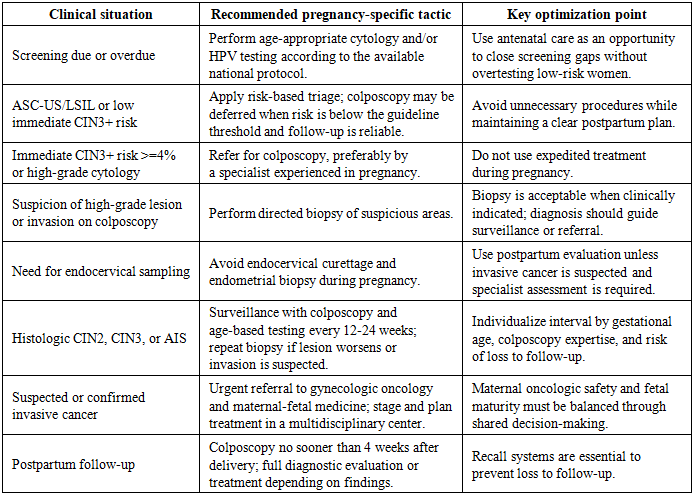
- Pregnancy causes predictable changes in the cervix: increased vascularity, softening, edema, glandular hypertrophy, cervical ectropion, mucus production, and decidualized stromal reaction. These changes may be visible on speculum examination or colposcopy and can resemble inflammation, low-grade lesions, or even high-grade colposcopic patterns. For this reason, the diagnostic accuracy of colposcopy in pregnancy depends strongly on examiner experience.Benign cervical findings are common in pregnancy. Cervical ectropion is often physiologic and does not require treatment unless symptoms are persistent and other causes have been excluded. Cervicitis should be evaluated according to clinical context and local protocols, with attention to microbiological diagnosis and pregnancy-compatible treatment when infection is confirmed. Cervical polyps are usually benign, but management is individualized: observation is appropriate for asymptomatic lesions with benign appearance, while removal or biopsy is considered when malignancy is suspected, bleeding is clinically significant, or the diagnosis is uncertain [17,18].A crucial optimization principle is that symptoms and visual findings should not be dismissed as physiologic without adequate evaluation. Conversely, physiologic ectropion or benign polyps should not automatically trigger destructive treatment. The safest strategy is targeted assessment: history, speculum examination, review of screening status, pregnancy-safe testing when indicated, and referral for colposcopy when risk thresholds are met or cancer is suspected.Current evidence-based management favors risk-based triage rather than rigid algorithms based only on cytology categories. The 2019 ASCCP guidelines introduced a paradigm in which management is determined by the estimated immediate and future risk of CIN3+ using current and previous test results [4]. Pregnancy does not change the natural history of HPV, and pregnant patients with abnormal screening results are generally managed using the same clinical action thresholds as nonpregnant patients, while avoiding procedures and treatments that are unsafe or unnecessary during pregnancy [6].Screening may be performed during pregnancy if the woman is due or overdue according to national or local screening recommendations. Cytology and HPV testing can be collected safely with appropriate sampling technique. However, pregnancy should not be used as a reason for excessive repeat testing in women who are already adequately screened and low risk. The aim is to detect clinically meaningful disease and ensure postpartum continuity, not to intensify screening without indication.ASCCP pregnancy-specific guidance recommends colposcopy when the immediate risk of CIN3+ is 4% or greater. Expedited treatment is not recommended in pregnancy, and excisional procedures are reserved for situations in which cancer is suspected [6]. This approach reflects a balance between the low short-term progression risk of most preinvasive lesions and the serious consequences of missing invasive cancer.Colposcopy in pregnancy should preferably be performed by an experienced colposcopist. Pregnancy-related changes can reduce specificity, and the transformation zone may be more difficult to interpret. Documentation should include gestational age, indication for referral, cytology and HPV results, transformation zone visibility, colposcopic impression, biopsy sites if taken, and the plan for surveillance or postpartum assessment.Directed cervical biopsy is considered safe in pregnancy when clinically indicated and is not generally associated with adverse surgical or obstetric outcomes [6]. Nevertheless, biopsy should be purposeful rather than routine: it is indicated when the colposcopic impression suggests high-grade disease or invasion, when cytology is high risk and a lesion is visible, or when the diagnosis will change management. Endocervical curettage and endometrial biopsy are contraindicated or unacceptable during pregnancy because of potential risk to pregnancy and because they do not align with conservative management principles [4,7].The role of pathology is central. When biopsy confirms CIN1 or low-grade disease, observation is usually sufficient. When CIN2, CIN3, or AIS is diagnosed, treatment is generally deferred, but surveillance is required. If biopsy suggests microinvasive or invasive carcinoma, the patient should be referred urgently to gynecologic oncology and maternal-fetal medicine for staging and individualized management.
|
|
4. Discussion
- The literature supports a balanced strategy. Overly aggressive management can expose pregnant patients to unnecessary procedures, bleeding, anxiety, and potential obstetric risks. Excessively passive management can delay diagnosis of invasive cancer or allow loss to follow-up. The optimal tactic is therefore neither immediate treatment nor simple postponement, but structured risk-based care.For HPV-associated lesions, the key clinical insight is that pregnancy does not substantially alter the progression risk of HPV-related precancer. Conservative management is safe when performed within a system that can reliably exclude invasion, monitor high-grade lesions, and complete postpartum evaluation. For structural cervical pathology, the logic differs: the goal is prevention of pregnancy loss and preterm birth, so decisions depend on cervical length, previous obstetric history, cervical dilation, and prior cervical surgery.Several areas require further research in Central Asian populations. These include prevalence of high-risk HPV genotypes among pregnant women, postpartum regression rates of CIN in local cohorts, barriers to postpartum colposcopy attendance, pregnancy outcomes after cervical excisional procedures, and cost-effectiveness of integrated antenatal screening review. Local data would help adapt international guidelines to regional resources and patient pathways.
5. Conclusions
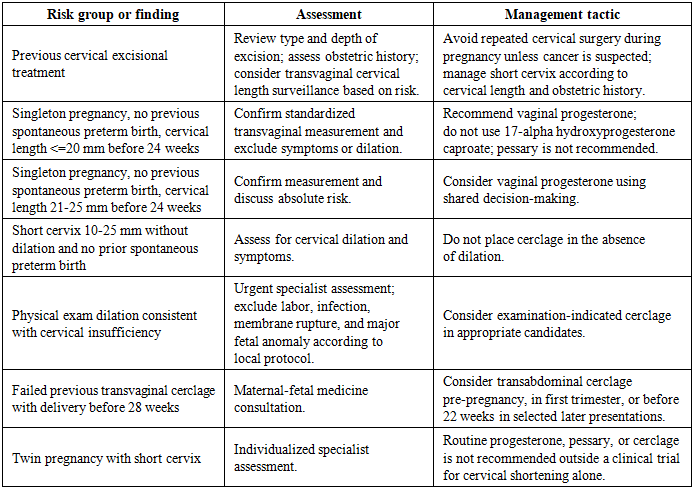
- Management of pregnant women with cervical pathology should be individualized, evidence-based, and organized around maternal safety and fetal well-being. The principal steps are: identify overdue screening, use risk-based triage, refer appropriately for expert colposcopy, perform biopsy only when clinically indicated, avoid endocervical curettage and expedited treatment, surveil CIN2/3 and AIS during pregnancy, refer suspected cancer immediately, and ensure postpartum diagnostic closure. Structural cervical pathology requires a parallel obstetric pathway based on standardized transvaginal cervical length assessment, progesterone when indicated, and selective cerclage in high-risk patients.The proposed optimized pathway can improve quality of care by reducing unnecessary interventions, preventing missed invasive disease, and linking antenatal findings to postpartum management. In Uzbekistan, where cervical cancer prevention is developing alongside successful HPV vaccination efforts, such an approach is clinically relevant and suitable for implementation in obstetric and gynecologic practice.