-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(6): 2896-2898
doi:10.5923/j.ajmms.20261606.26
Received: May 19, 2026; Accepted: May 29, 2026; Published: Jun. 4, 2026

Urolithiasis vs. Chronic Upper Urinary Tract Obstruction: A Comparative Analysis of Their Impact on the Progression of Chronic Kidney Disease
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLS. S. Kariev, Sh. T. Mukhtarov, Sh. I. Giyasov, B. Sh. Jumayev
Republican Specialized Scientific and Practical Medical Center of Urology, Tashkent, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The aim of this systematic review was to compare molecular, hemodynamic and kinetic parameters of renal function decline in patients with kidney stones disease and chronic noncalculous upper urinary tract obstruction. Background. The progression of chronic kidney disease in the context of urological conditions is heterogeneous in nature. The development of chronic kidney disease in patients with kidney stones disease and chronic upper urinary tract obstruction was long considered to be identical; however, recent data point to fundamental differences in their molecular mechanisms. Methods. A systematic search of publications in the Scopus and PubMed databases was conducted up to May 2026. The analysis included clinical studies evaluating long-term renal prognosis, markers of fibrosis, and the rate of decline in eGFR for various phenotypes of kidney stones disease and obstructive disorders. Results. It was found that in cases of upper urinary tract obstruction, the decline of kidney function is linear in nature due to hydrostatic stress. In contrast, the decline in eGFR in patients with kidney stones disease is nonlinear and depends on the frequency of urolithiasis recurrences, the composition of the stones, and the severity of concomitant calculous pyelonephritis. Due to the rate of fibrosis, genetic forms of kidney stones disease (such as primary hyperoxaluria) approach obstruction of the upper urinary tract. Conclusion. The renal prognosis in cases of upper urinary tract obstruction depends on the speed of decompression, whereas in cases of kidney stones disease urolithiasis, personalized metaphylactic therapy and recurrence management are of key importance.
Keywords: Chronic kidney disease, Urolithiasis, Kidney stones disease, Obstructive uropathy, Glomerular filtration rate, Tubulointerstitial fibrosis
Cite this paper: S. S. Kariev, Sh. T. Mukhtarov, Sh. I. Giyasov, B. Sh. Jumayev, Urolithiasis vs. Chronic Upper Urinary Tract Obstruction: A Comparative Analysis of Their Impact on the Progression of Chronic Kidney Disease, American Journal of Medicine and Medical Sciences, Vol. 16 No. 6, 2026, pp. 2896-2898. doi: 10.5923/j.ajmms.20261606.26.
Article Outline
1. Introduction
- The development and progression of chronic kidney disease (CKD) in the context of interstitial and obstructive lesions plays a significant role in modern urological nephrology [1]. Among these pathologies, kidney stones disease and chronic upper urinary tract obstruction (UUTO) are the most common triggers of renal dysfunction. [2]. It was long believed that the degeneration of the renal parenchyma in kidney stones disease was exclusively obstructive in nature, caused by a transient or persistent blockage of the urinary tract by a calculus [3].However, recent epidemiological studies show that kidney stones disease is a systemic metabolic disorder in which the kidney is injured even in the absence of macroscopic occlusion [1,4].Timely evaluation of CKD risks requires a clear understanding of how the pathogenesis of non-occlusive forms of kidney stones disease differs from the total hydrodynamic pressure typical for true upper urinary tract obstruction [5,6]. The aim of this systematic review was to conduct a comparative analysis of molecular, hemodynamic and kinetic parameters of renal function decline in patients with kidney stones disease and chronic non-calculous upper urinary tract obstruction.
2. Material and Methods
- Publications were filtered and selected in accordance with the methodology of systematic reviews in the peer-reviewed Scopus, PubMed/MEDLINE, and Embase databases. The time frame covered publications up to May 2026. Search queries were generated based on combinations of the following keywords: “urolithiasis,” “nephrolithiasis,” “chronic kidney disease,” “ureteral obstruction”.The inclusion criteria were prospective and retrospective cohort studies of adult patients in which the dynamics of the estimated glomerular filtration rate (eGFR) were assessed in the context of kidney stones disease or upper urinary tract obstruction [2,3]. Experimental studies (including models of unilateral ureteral obstruction) were used to elucidate the molecular differences in fibrogenesis between upper urinary tract obstruction and crystal-induced inflammation typical of kidney stones disease [6].
3. Results
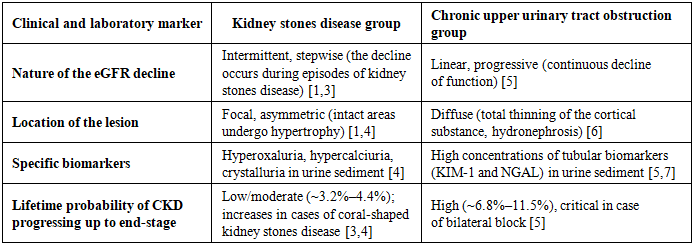
- Pathophysiological markers of kidney injury in kidney stones disease In urolithiasis, the initiation of renal injury is multifactorial, focal and primarily immune-mediated [1,4]:Crystalloid inflammation and the macrophage response: free microcrystals of calcium oxalate or calcium phosphate, typical for metabolic forms of urolithiasis, injure the membranes of tubular epithelial cells. It activates M1-phenotype macrophages, which synthesize and release interleukin-1β (IL-1β) and trigger local sclerosis [4].Formation of Randall's plaques: interstitial calcification of the papillae in kidney stones disease leads to focal ischemia. Only the nephrons associated with the Henle's loop region are injured, while the rest of the parenchyma retains its compensatory function for a long time [1].Infectious fibrosis: struvite (infectious) stones present a particular risk in kidney stones disease. The chronic calculous pyelonephritis associated with them leads to focal scarring of the renal cortex [3,4].Pathophysiological markers of kidney injury in chronic upper urinary tract obstruction (UUTO) Unlike kidney stones disease, non-calculous upper urinary tract obstruction affects the entire kidney through hydrodynamic pressure [5,6]:Epithelial-mesenchymal transition (EMT): Persistent increases of intrarenal pressure in upper urinary tract obstruction stimulate the production of TGF-β1, which causes epithelial cells of the tubules to transform into fibroblasts [6].Global ischemia: stretching of the renal pelvis compresses the arcuate and radial arteries, causing diffuse hypoxia of the entire organ, which is not observed in uncomplicated kidney stones disease [5,6].Comparative kinetics of eGFR in urolithiasis and upper urinary tract obstructionLong-term patient monitoring reveals fundamental differences in the dynamics of kidney function decline (Tab. 1, Fig. 1).
|
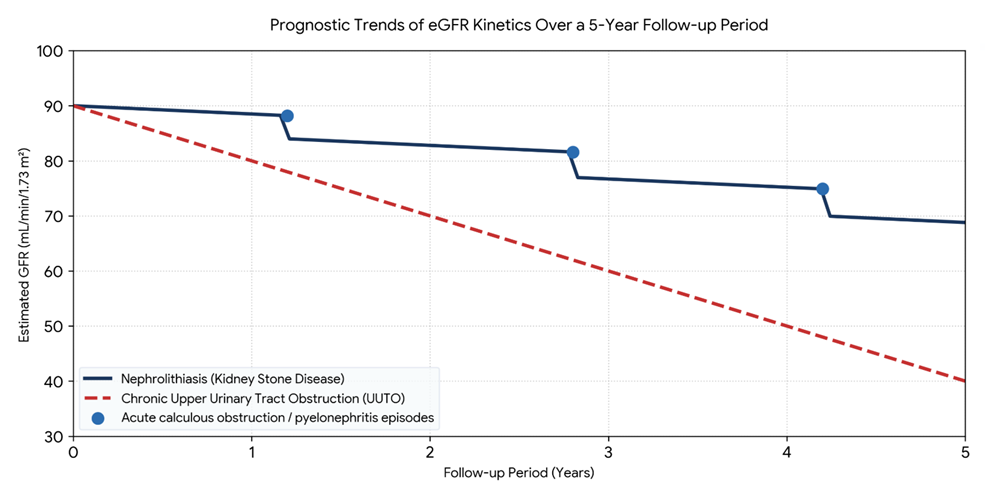 | Figure 1. Comparative changes in eGFR over the long-term observation period. Dot-dashed line (UUTO) reflects continuous nephron degradation due to persistent intrarenal hypertension [6]. The stepped curve (kidney stone disease) demonstrates relative stability of the parenchyma during the interictal period, with isolated drops in function during stone attacks or episodes of infection exacerbation [1,3] |
4. Discussion
- The results of the analysis show that kidney stone disease cannot be viewed solely as a mechanical problem. Epidemiological data confirm that patients with kidney stones have a relative risk of developing CKD of 1.52 compared to the general population [3]. However, this risk is distributed extremely unevenly. In patients with isolated episodes of calcium oxalate nephrolithiasis, kidney function may remain stable for decades due to compensatory hyperfiltration by the contralateral kidney or healthy areas of the parenchyma [1,2]. On the contrary, a progressive decline of GFR in kidney stone disease is associated with coral-shaped stones, frequent recurrences and hereditary forms (cystinuria, primary hyperoxaluria), in which the constant precipitation of crystals in the tubules through the mechanism of injury mimics chronic microobstruction [4].In true chronic UUTO, compensatory mechanisms are depleted much more rapidly [5,6]. In UUTO, the intrarenal renin-angiotensin-aldosterone system (RAAS) is activated totally, rather than focally, as in kidney stone disease [6]. If the obstruction is not surgically resolved within the first two weeks, the induced fibrogenesis becomes autonomous, and tissue degradation continues even after the blockage has been removed [6,7]. In cases of kidney stones, timely removal of the stone and appropriate preventive treatment can completely halt the decline of eGFR [1,4].
5. Conclusions
- The prognosis for CKD progression in patients with kidney stones disease is significantly more favorable than in patients with persistent UUTO.The pathogenesis of renal failure in kidney stones disease is closely associated with metabolic imbalance, local inflammation of the interstitium and recurrent infection, which determines the advisability of prolonged conservative treatment, diet therapy and metaphylaxis.Chronic UUTO is accompanied by gross irreversible deformation of anatomical structures, necessitating immediate surgical intervention for decompression, since delay leads to diffuse irreversible fibrosis of the parenchyma.
Conflict of Interests’ Statement
- The authors declare no conflict of interest. This study does not include the involvement of any budgetary, grant or other funds. The article is published for the first time and is part of a scientific work.