-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(6): 2891-2895
doi:10.5923/j.ajmms.20261606.25
Received: May 16, 2026; Accepted: Jun. 2, 2026; Published: Jun. 4, 2026

Nephrolithiasis as an Independent Factor in the Progression of Chronic Kidney Disease: Pathophysiological Cascades, Predictors and Analysis of Renal Functional Survival
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLS. S. Kariev, Sh. T. Mukhtarov, Sh. I. Giyasov, B. Sh. Jumayev
Republican Specialized Scientific and Practical Medical Center of Urology, Tashkent, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The aim of the study was to assess the impact of primary and recurrent nephrolithiasis on the pattern and rate of decline in estimated glomerular filtration rate (eGFR) in young patients, to identify independent prognostic clinical and laboratory criteria influencing the progression of chronic kidney disease, and to conduct an actuarial analysis of the stability of renal filtration capacity. Background. Chronic kidney disease has firmly held its place as one of the most threatening non-communicable pandemics of the 21st century over the past few decades. The paradigm of pathogenetic monitoring in standard therapeutic and nephrological practice has traditionally focused on systemic metabolic and hemodynamic predictors of renal fibrosis, such as type 2 diabetes mellitus, essential hypertension, as well as secondary hypertension. Materials and methods. The main clinical cohort of the study consisted of 143 patients. The primary inclusion criteria were the presence of a persistent and continuously progressive decline in eGFR to the level corresponding to Stage IIIa–IV chronic kidney disease. There were 109 (76.2%) men and 34 (23.8%) women in the study group. Results. In the primary nephrolithiasis group (n = 46), the annual decline in eGFR was controlled and averaged 1.2–1.7 mL/min/1.73 m² per year. In the recurrent nephrolithiasis group (n = 97), a sharp acceleration in the rate of eGFR decline was observed—averaging 2.80 to 4.50 mL/min/1.73 m² per year (p < 0.01). Discussion. The results of this study provide compelling evidence that nephrolithiasis (particularly its recurrent forms) acts as a powerful independent predictor of a rapid decline in eGFR, doubling the risk of chronic kidney disease progression regardless of traditional therapeutic factors. The controlled decline in eGFR observed in the primary nephrolithiasis group (1.2–1.7 mL/min per year) is consistent with fundamental epidemiological data from the Mayo Clinic, according to which an isolated calculous episode without signs of persistent obstruction does not have a fatal impact on overall renal parenchymal function. Conclusion. The results of our study provide compelling evidence that nephrolithiasis is a significant independent predictor of progressive renal function decline. Moreover, the recurrent nature of urolithiasis acts as a catalyst for nephrosclerosis, accelerating the annual decline in eGFR by 3–4 times compared to the rate of natural age-related involution of renal tissue.
Keywords: Chronic kidney disease, Nephrolithiasis, Estimated glomerular filtration rate
Cite this paper: S. S. Kariev, Sh. T. Mukhtarov, Sh. I. Giyasov, B. Sh. Jumayev, Nephrolithiasis as an Independent Factor in the Progression of Chronic Kidney Disease: Pathophysiological Cascades, Predictors and Analysis of Renal Functional Survival, American Journal of Medicine and Medical Sciences, Vol. 16 No. 6, 2026, pp. 2891-2895. doi: 10.5923/j.ajmms.20261606.25.
Article Outline
1. Introduction
- Chronic kidney disease (CKD) has firmly established itself over the past few decades as one of the most threatening noncommunicable pandemics of the 21st century. According to data from large-scale international epidemiological consortia, the global prevalence of CKD among the world’s adult population ranges from 10% to 14%, which entails enormous socioeconomic costs for national health care systems and exponentially increases cardiovascular mortality rates [1-2]. The paradigm of pathogenetic monitoring in standard medical and nephrological practice has traditionally focused on systemic metabolic and hemodynamic predictors of renal fibrosis, such as type 2 diabetes mellitus, essential and secondary hypertension, obesity, and primary immune-inflammatory glomerulopathies [3-4]. At the same time, urological diseases, among which nephrolithiasis (urolithiasis) occupies a leading place, were considered by clinicians in isolation for a long time. As part of the routine approach, the calculus process was viewed as a discrete, purely surgical pathology requiring immediate relief of the obstruction and elimination of acute pain (renal colic), after which the patient was often discharged without adequate interdisciplinary follow-up [5-6].However, the landscape of views on the systemic consequences of urolithiasis has undergone fundamental changes over the past fifteen years. Large-scale, long-term population registries and cohort studies initiated by leading global centers (in particular, the Mayo Clinic’s long-term projects and the NHANES national screening databases) have identified a consistent, statistically significant independent association between a history of nephrolithiasis and the risk of a forced decline in glomerular filtration rate (GFR) [7-8]. It has been established that the presence of stones in the renal pelvis is associated with a 1.5–2.2-fold increased risk of developing moderate to severe chronic kidney disease (CKD), with the likelihood of developing end-stage kidney disease (ESKD), requiring lifelong scheduled hemodialysis or peritoneal dialysis, increasing by an average of 60–70% [9-10]. The risk of renal atrophy is particularly significant in the middle-aged cohort (40–50 years), as in these patients, involutive processes in the parenchyma begin to overlap with the cumulative damaging effects of a calculous history creating a synergistic destructive impact [11].Despite the obvious epidemiological link, modern uronephrology has not yet clearly differentiated the trajectories of decline in renal function in patients who have experienced a primary (single) isolated attack of stone formation and individuals with an aggressive, repeatedly recurring course of urolithiasis. The majority of existing clinical guidelines (from both the European Association of Urology [EAU] and the American Urological Association [AUA]) provide detailed recommendations on metaphylactic therapy to prevent stone recurrence; however, algorithms for long-term nephron preservation and the preventive interception of CKD in these patients remain the least well-developed area [12-13]. The latent and fluctuating nature of the loss of renal filtration capacity means that practitioners often miss the critical therapeutic window for nephroprotection. The problem is complicated by the fact that the contribution of various clinical and physicochemical phenotypes of nephrolithiasis to the rate of decline in estimated glomerular filtration rate (eGFR) in adult patients has not yet been comprehensively and systematically covered in domestic and international scientific literature [14-15].The pathophysiological pathway linking localized salt precipitation in the tubules to widespread organ sclerosis involves several destructive cascades that occur in parallel. The first and most well-studied macroscopic factor is retrograde hydrodynamic obstruction of the urinary tract [16]. Obstruction of the renal pelvis or ureter caused by the migration of a calculus triggers an immediate surge in intraluminal pressure. It reverse barometric pressure is transmitted unimpeded upward through the collecting ducts directly into Bowman’s capsule, deforming it and reducing the efficient ultrafiltration pressure to zero [17]. Mechanical overstretching of the tubule walls inevitably leads to compression of the adjacent peritubular capillary bed. Under conditions of acute or subacute microvascular compression, a local ischemic cascade unfolds: tissue hypoxia of the parenchyma triggers massive lipid peroxidation, the release of free radicals, and, as a result, programmed cell death (apoptosis) of the tubular epithelium [18-19]. In cases of frequent recurrent obstruction, the parenchyma is subjected to repeated ischemic-reperfusion injury, leading to a mosaic loss of functioning nephrons. In the early stages of the disease (the first 5–7 years), estimated glomerular filtration rate (eGFR) values may remain within the subnormal range for an extended period. It is because intact, undamaged nephrons undergo compensatory hypertrophy and take on the filtration load of the lost areas, functioning under conditions of forced intraglomerular hypertension [20]. The aim of the study was to assess the impact of primary and recurrent nephrolithiasis on the pattern and rate of decline in estimated glomerular filtration rate (eGFR) in young patients, to identify independent prognostic clinical and laboratory criteria influencing the progression of chronic kidney disease, and to conduct an actuarial analysis of the stability of renal filtration capacity.
2. Material and Methods
- The main clinical cohort of the study was consisted from 143 patients who underwent examination, outpatient or inpatient treatment for clinically -radiologically confirmed nephrolithiasis at the Republican Specialized Scientific and Practical Medical Center of Urology of the Republic of Uzbekistan and the Republican Specialized Scientific and Practical Medical Center of Surgery named after academician V. Vakhidov during the period from June 2010 to May 2023. The main inclusion criterion was the presence of a persistent and continuously progressive decline of eGFR to the level of stage IIIa–IV chronic kidney disease. The mean age of patients in the selected overall cohort was 43.8 ± 5.4 years (age range was 18 to 65 years). Meanwhile, 77 patients (53.8%) belonged to the most socially active age group (18–44 years). Middle-aged people (aged 45 to 59) accounted for 56 (39.2%) cases, while the proportion of patients in the older age group (aged 60–65) consisted of 10 (7.0%) cases. There were 109 (76.2%) men and 34 (23.8%) women in the study groups.All patients were divided proportionally into two groups based on the nature of disease course:• Primary nephrolithiasis group: n=46 (32.2%)—patients with a history of a single episode of clinically and radiologically confirmed nephrolithiasis, with no recurrence of nephrolithiasis during the follow-up period.• Recurrent nephrolithiasis group: n=97 (67.8%)—patients with a history of two or more episodes of clinically and radiologically confirmed recurrent nephrolithiasis.In this context, calcium oxalate and mixed types of stone formation predominated in the mineral composition of the stones, which were identified in 90.9% of patients (n=130) against a background of endogenous metabolic disorders. The non-calcium physicochemical types were distributed as follows: uric acid (urate) nephrolithiasis associated with early uricosuria — 5.6% (n=8), infectious (struvite) nephrolithiasis — 2.8% (n=4), cystine nephrolithiasis — 0.7% (n=1).Changes in renal filtration capacity were monitored annually using eGFR values calculated by the international CKD-EPI formula based on changes in serum creatinine levels. Mathematical and statistical data analysis was performed using multivariate logistic regression analysis to identify systemic enzyme disorders and determine the odds ratio and 95% confidence interval for independent urological parameters. Indicators of long-term renal function preservation (maintenance of eGFR ≥ 30 mL/min/1.73 m²) were calculated using Kaplan-Meier survival curves. The significance of the differences between the renal function curves was verified using the log-rank test at a significance level of p < 0.05.
3. Results
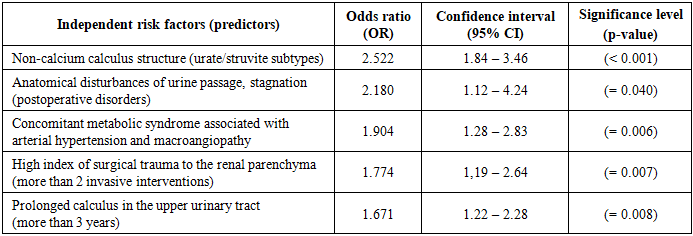
- An analysis of long-term clinical and laboratory data revealed that signs of progressive deterioration in renal filtration, consistent with the criteria for stages IIIa–IV of chronic kidney disease, developed in 19.3% of verified cases among patients with urolithiasis, demonstrating the role of nephrolithiasis as an independent trigger of renal function degradation. When analyzing the rates of decline in eGFR separately, the following fundamental differences were identified between the clinical groups:• In the primary nephrolithiasis group (n = 46), the annual loss of eGFR was within a controlled range, averaging 1.2–1.7 mL/min/1.73 m² per year, which is slightly faster than the rate of natural age-related decline in renal filtration capacity (physiological parenchymal involution) in a healthy individual, which normally amounts to approximately 1.0 mL/min per year after age 40. The prognosis for the development of severe uremia in this patient group is considered favorable if dietary restrictions are followed.• In the group with recurrent nephrolithiasis (n = 97), a sharp acceleration in the rate of decrease of eGFR was recorded—on average, from 2.80 to 4.50 mL/min/1.73 m² per year (p < 0.01). The most unfavorable prognostic course has been observed in patients with a high incidence of calculous obstruction of the upper urinary tract (more than 3 acute episodes of obstruction associated with attacks of secondary pyelonephritis), where the annual decline in filtration reached critical levels—8.64 mL/min/1.73 m² per year (p <0.005).A multifactorial regression model was constructed to verify urological parameters as independent risk factors of nephro-sclerosis. After standardization and adjustment for age, sex, and baseline blood pressure, key isolated markers of high risk of falling eGFR were identified (Table 1).
|
4. Discussion
- The obtained results of the study convincingly prove that nephrolithiasis (especially its recurrent forms) acts as a powerful autonomous predictor of forced decline of eGFR, doubling the risk of CKD progression regardless of traditional therapeutic factors.The observed controlled decline of eGFR (1.2–1.7 mL/min per year) in the primary nephrolithiasis group is consistent with the Mayo Clinic’s fundamental epidemiological data, according to which an isolated episode of calculi without signs of persistent obstruction does not have a fatal impact on overall renal parenchymal function [7,10]. In contrast, the sharp acceleration of eGFR decline we observed in middle-aged patients with recurrent stone formation (2.80 –4.50 mL/min per year) and the sharp downward shift in the slope of the Kaplan-Meier curve to 81.0% observed within a 7–8-year period of calculous history serves as clinical confirmation of Brenner’s hyperfiltration concept [20].During the first 5 years, a period of subclinical hemodynamic compensation is observed: nephrons lost due to microobstruction are masked by the compensatory intraglomerular hypertension of the intact glomeruli. At the same time, prolonged intraglomerular hypertension depletes the functional reserve of surviving nephrons, leading to secondary glomerulosclerosis and a rapid loss of clearance capacity in the later stages, as confirmed by the literature [9-10].The high nephrotoxic potential of non-calcium stones identified in the regression model (OR = 2.522) is pathophysiologically explained by the specific nature of their metabolic and microbial profiles. Uric acid nephrolithiasis is induced by a persistent decrease in urinary pH and associated tissue insulin resistance, which act as triggers of intracellular metabolic stress. Struvite stones, in turn, serve as a constant reservoir of infection, leading to chronic obstructive pyelonephritis. The cascade of crystal-induced stromal fibrosis occurs through mechanisms validated in recent immunobiological studies: crystalline structures are taken up by nephrons via endocytosis, triggering the assembly and activation of the intracellular multiprotein NLRP3 complex. It results in paracrine overproduction of interleukin-1β (IL-1β) and TNF-α, which recruit macrophages and trigger irreversible tubulointerstitial fibrosis [21,22].The index of surgical trauma of the renal parenchyma (the iatrogenic component of decompensation) deserves special attention. The proven independent significance of a high operational workload index (OR = 1.774) is consistent with the findings of Torres-SanMiguel (2022) [23]. Every surgical intervention (whether it involves cavitational rupture of microvessels during extracorporeal shock wave lithotripsy or the mechanical creation of a percutaneous nephrostomy tract during percutaneous lithotripsy) leaves an ischemic mark that is organized into a fibrous scar, thereby mechanically reducing the number of functioning nephrons. The synergistic effect of urological injury and concomitant comorbidities (OR = 1.904) in middle-aged patients (mean age 43.8 years) points to the need for a fundamental reevaluation of treatment strategies. Shifting the focus from surgical stone removal to early monitoring of the longitudinal trend in renal filtration function and implementing rigorous anti-relapse metaphylactic measures is the only way to extend the prognostic window for renal function.
5. Conclusions
- The results of this study provide compelling evidence that nephrolithiasis is a significant independent predictor of progressive renal dysfunction. Moreover, the recurrent nature of the course of urolithiasis acts as a catalyst for nephrosclerosis, accelerating the annual decline in eGFR by 3–4 times compared to the rate of natural age-related involution of renal tissue.The established two-phase nature of the functional decline, marked by a sharp drop in filtration survival after 5 years of disease, underscores the insidious nature of the latent period of interstitial fibrosis. The current management strategy for patients with urolithiasis needs to be completely overhauled: surgical fragmentation and removal of stones represent only the initial stage of treatment. Prevention of CRF in this category of patients requires mandatory regular monitoring of eGFR (according to the CKD-EPI formula), early implementation of extended metabolic screening of 24-hour urine and the introduction of continuous personalized metaphylaxis.
Ethical Approval and Consent to Participate
- Our institution's research ethics board does not require review or approval of case reports.Our investigation is conducted in accordance with the World Medical Association's Code of Ethics (Declaration of Helsinki).
Source of Funding
- Each author has reviewed and approved this manuscript. None of the authors has any conflict of interest, financial or otherwise. This manuscript is original, no part of it has been previously published, and it is not being considered for publication elsewhere. The corresponding author agrees to take full responsibility for authorship during the submission and review stages of the manuscript.
Conflict of Interests
- The authors declare no conflict of interest. This study does not include the involvement of any budgetary, grant or other funds. The article is published for the first time and is part of a scientific work.
ACKNOWLEDGEMENTS
- The authors express their gratitude to the management of the multidisciplinary clinic of Republican Specialized Scientific and Practical Medical Center of Urology of the Republic of Uzbekistan and the Republican Specialized Scientific and Practical Medical Center of Surgery named after academician V. Vakhidov for the material provided for our study.