-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(6): 2862-2867
doi:10.5923/j.ajmms.20261606.20
Received: Apr. 26, 2026; Accepted: May 20, 2026; Published: Jun. 3, 2026

Prognostic Description of the Role of Environmental Factors in the Emergence of COVID-19-Related Lung Injuries
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMarkhabo Tursunova1, Nematjon Mamasaliev2, Khatam Tursunov2, Zohidjon Mamasaliev3, Burhonjon Usmonov2
1Department of Propaedeutics of Internal Medicine, Andijan State Medical Institute, Andijan, Uzbekistan
2Department of Internal Medicine, Cardiology and Emergency Medicine, Andijan State Medical Institute, Andijan, Uzbekistan
3Department of Ophthalmology, Andijan State Medical Institute, Andijan, Uzbekistan
Correspondence to: Markhabo Tursunova, Department of Propaedeutics of Internal Medicine, Andijan State Medical Institute, Andijan, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

COVID-19–associated lung injury represents a complex and multifactorial clinical condition, with premorbid and environmental risk factors playing a critical role in disease progression and severity. The aim of this study was to evaluate the prevalence, premorbid background, clinical manifestations, and pharmacoepidemiological characteristics of COVID-19–associated lung injury, and to develop an effective predictive and preventive framework. The study was based on epidemiological, clinical, laboratory, immunological, and statistical methods, including analysis of venous blood and serum biomarkers in infected patients. A population-based assessment (n = 1409, aged 18–74 years) was conducted to determine the prognostic role of key premorbid risk factors. The results demonstrated that the combined influence of premorbid factors significantly increased the risk of developing various forms of COVID-19–associated lung injury, with mild pneumonia (37.2%) and severe pneumonia (23.3%) being the most prevalent outcomes. The overall risk increased by more than 54% under the cumulative effect of premorbid conditions. Five major determinants—cardiovascular diseases, hypertension, smoking, physical inactivity, and immune alterations—were identified as key predictors of adverse outcomes. Based on these findings, a mathematical model for risk stratification was developed, enabling classification of patients into very high, high, low, and very low risk categories. In addition, a regional preventive programme was proposed, demonstrating its applicability for reducing complications and improving clinical outcomes. The study confirms that integrated epidemiological and predictive modelling approaches are essential for early risk identification and effective prevention of COVID-19–associated lung injury.
Keywords: COVID-19, Lung injury, Premorbid factors, Epidemiology, Risk modelling, Prevention, Comorbidity
Cite this paper: Markhabo Tursunova, Nematjon Mamasaliev, Khatam Tursunov, Zohidjon Mamasaliev, Burhonjon Usmonov, Prognostic Description of the Role of Environmental Factors in the Emergence of COVID-19-Related Lung Injuries, American Journal of Medicine and Medical Sciences, Vol. 16 No. 6, 2026, pp. 2862-2867. doi: 10.5923/j.ajmms.20261606.20.
Article Outline
1. Introduction
- The emergence and rapid global spread of coronavirus disease 2019 (COVID-19), caused by the novel severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has become one of the most significant public health challenges of the twenty-first century. Since its initial detection in December 2019, the infection has demonstrated an unprecedented transmission rate, leading the World Health Organization to declare a global pandemic in early 2020. Within a few months, millions of confirmed cases were reported across more than 160 countries, highlighting the urgent need for coordinated scientific, clinical, and preventive responses [1–5].Over the course of the pandemic, a substantial body of research has been generated, covering epidemiology, clinical management, and therapeutic strategies. These studies have provided important insights into disease mechanisms and have facilitated the development of evidence-based clinical guidelines. At the same time, growing attention has been directed towards preventive approaches, particularly those aimed at identifying high-risk populations and mitigating disease severity [6–10].COVID-19 primarily affects the respiratory system, although its clinical manifestations vary widely, ranging from mild symptoms to severe pneumonia and acute respiratory distress syndrome. Importantly, pulmonary complications may persist long after the acute phase of infection, contributing to the development of post-COVID syndrome and long-term functional impairment [11–13]. These findings underline the need for a comprehensive understanding of both acute and chronic forms of COVID-19–associated lung injury.Previous studies have demonstrated that coronaviruses possess strong pathogenic potential in the respiratory tract, contributing to the development of bronchial obstruction and other pulmonary complications. Evidence from clinical investigations has confirmed a clear association between SARS-CoV-2 infection and a wide spectrum of respiratory disorders, including bronchial obstruction, inflammatory syndromes, and impaired pulmonary function [14–18]. In this context, the role of pre-existing (premorbid) conditions and environmental risk factors has become increasingly important in determining disease progression and clinical outcomes.In recent years, particular emphasis has been placed on the interaction between premorbid background, comorbid conditions, and external risk factors such as smoking, physical inactivity, and environmental exposures. These determinants are believed to significantly influence the severity and prognosis of COVID-19–associated lung injury, yet their combined predictive value remains insufficiently explored [19–22]. Moreover, the rapid expansion of pharmacological interventions during the pandemic has introduced additional challenges, including the risk of adverse drug reactions and iatrogenic complications, which further complicate clinical management [23,24].Despite the growing volume of international research, there remains a lack of region-specific epidemiological studies addressing the complex interplay of premorbid factors, clinical manifestations, and pharmacoepidemiological characteristics of COVID-19–associated lung injury, particularly in Central Asian settings such as Uzbekistan. The absence of such data limits the development of targeted preventive strategies and evidence-based healthcare planning at the regional level.Therefore, there is a clear need to develop integrated approaches that combine epidemiological analysis, clinical assessment, and predictive modelling to improve early diagnosis, risk stratification, and prevention of COVID-19–associated lung injury. The establishment of such frameworks is expected to provide not only clinical benefits but also broader social and economic advantages by reducing disease burden and healthcare costs.The aim of this study is to evaluate the prevalence, premorbid background, clinical manifestations, and pharmacoepidemiological characteristics of COVID-19–associated lung injury, and to identify effective preventive strategies based on predictive assessment models.
2. Material and Methods
- This study was designed as a comprehensive observational and analytical investigation aimed at assessing the epidemiological, clinical, and predictive characteristics of COVID-19–associated lung injury. The research was conducted on a representative population of adult patients diagnosed with COVID-19, covering a broad age range and varying clinical presentations.The object of the study included venous blood and serum samples obtained from patients with confirmed SARS-CoV-2 infection. Biological samples were collected under standardized clinical conditions and processed for biochemical and immunological analyses. Laboratory assessments focused on evaluating key indicators associated with inflammatory response, immune status, and metabolic alterations relevant to pulmonary complications.The methodological framework of the study integrated multiple complementary approaches. Epidemiological methods were applied to assess disease prevalence, distribution patterns, and the influence of premorbid and comorbid factors on the development of lung injury. Clinical methods were used to evaluate patient history, symptomatology, and disease severity, with particular attention to respiratory manifestations and associated complications.Instrumental diagnostic techniques were employed to identify and characterise pulmonary involvement, including imaging-based assessment of lung tissue damage and functional impairment. Laboratory methods encompassed a range of biochemical and immunological tests aimed at identifying markers of systemic inflammation, immune dysregulation, and disease progression.In addition, immunological analysis was conducted to evaluate the functional status of the immune system and its role in the pathogenesis of COVID-19–associated lung injury. This allowed for a more detailed understanding of host response mechanisms and their contribution to disease severity.Statistical analysis constituted a central component of the study. Quantitative data were processed using standard statistical methods to determine the significance of observed differences and relationships. Risk ratios, confidence intervals, and comparative indicators were calculated to assess the predictive value of premorbid factors and clinical variables. The analytical approach enabled the identification of key determinants influencing the development and progression of lung injury, as well as the construction of a predictive framework for risk stratification.Overall, the combination of epidemiological, clinical, laboratory, immunological, and statistical methods provided a robust and integrated basis for evaluating COVID-19–associated lung injury and developing evidence-based preventive and predictive strategies.
3. Results
3.1. Distribution and Prognostic Role of Premorbid Factors
- The analysis of the obtained data demonstrated that premorbid background plays a significant role in the development and progression of COVID-19–associated lung injury in the studied population aged 18–74 years. The overall distribution of clinical forms and their association with premorbid factors are presented in Figure 1 and Table 1.
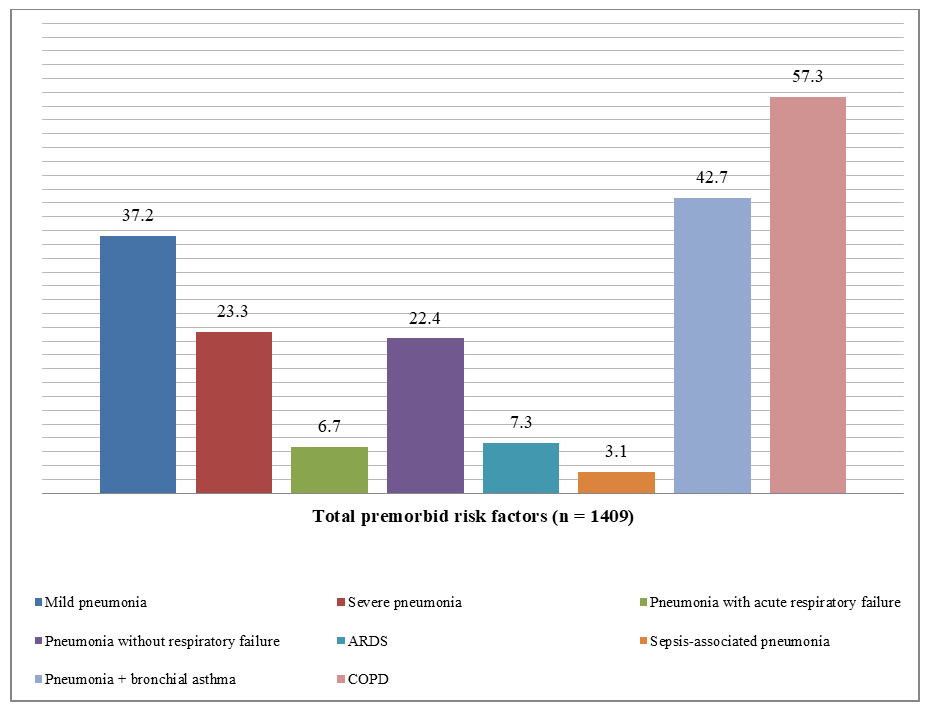 | Figure 1. Representation (%) of the predictive role of premorbid background in the formation of COVID-19–associated lung injury |
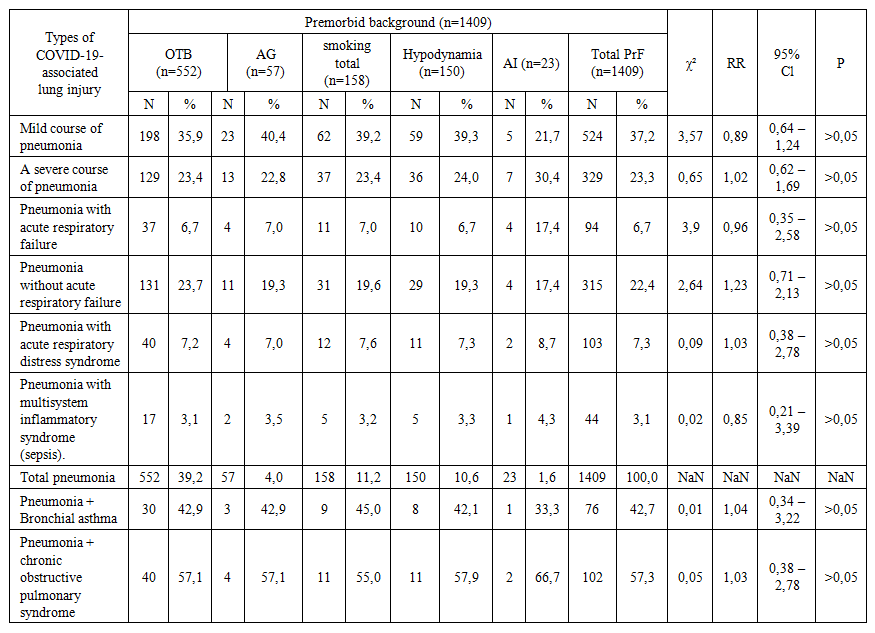 | Table 1. Predictive role of premorbid background in the occurrence of COVID-19–associated lung injury in the population aged ≥18–74 years |
3.2. Contribution of Individual Premorbid Components and Risk Stratification
- A more detailed analysis of individual premorbid components revealed that each factor contributes differently to the development of specific clinical forms of COVID-19–associated lung injury.1. For mild forms of pneumonia, the highest contributions were observed for arterial hypertension, smoking, and reduced physical activity, while immune-related conditions demonstrated a comparatively lower but still notable influence.2. In severe pneumonia, all premorbid factors showed a relatively balanced contribution, with a slightly higher impact of immune alterations.3. In cases complicated by acute respiratory failure, immune-related factors appeared to play a more pronounced role compared to other determinants.4. For pneumonia without respiratory failure, cardiovascular and lifestyle-related factors demonstrated a consistent influence pattern.5. In acute respiratory distress syndrome, all premorbid components contributed moderately, without a single dominant predictor.6. In inflammatory and septic complications, although overall prevalence was lower, the relative contribution of immune dysfunction was more evident.In addition, combined clinical conditions such as pneumonia associated with bronchial asthma and chronic obstructive pulmonary disease showed a higher prevalence, indicating the amplifying effect of comorbid respiratory disorders.Based on the integrated analysis, five key predictors were identified as having the most significant impact on disease progression and prognosis: cardiovascular diseases, arterial hypertension, smoking, physical inactivity, and immune-related alterations. These factors were subsequently used as the basis for predictive modelling and risk stratification.
4. Discussion
- The findings of the present study demonstrate that COVID-19–associated lung injury is strongly influenced by the combined effect of premorbid and comorbid factors, which significantly determine both disease severity and clinical outcomes. The observed predominance of mild and severe pneumonia, along with the presence of more complex clinical forms such as acute respiratory distress syndrome and sepsis, reflects the heterogeneous nature of pulmonary involvement in COVID-19.One of the key observations is that the cumulative impact of premorbid conditions leads to a substantial increase in the overall risk of lung injury, exceeding 50%. This finding supports the growing body of evidence suggesting that COVID-19 should not be considered solely as an acute infectious disease, but rather as a multifactorial condition in which pre-existing health status plays a decisive role in disease progression. In particular, the identified factors—cardiovascular diseases, arterial hypertension, smoking, physical inactivity, and immune-related alterations—appear to act synergistically, amplifying the severity of pulmonary complications.The relatively high prevalence of pneumonia in patients with coexisting respiratory conditions, such as bronchial asthma and chronic obstructive pulmonary disease, further highlights the vulnerability of individuals with compromised pulmonary function. These findings are consistent with the concept that structural and functional impairment of the respiratory system predisposes patients to more severe manifestations of viral infections.An important aspect of the results is the differentiated contribution of individual risk factors to various clinical forms of lung injury. While some factors demonstrated a consistent influence across all forms, others appeared to be more strongly associated with specific complications, particularly those involving respiratory failure and systemic inflammatory responses. This suggests that the pathogenesis of COVID-19–associated lung injury is not uniform, but rather depends on the interaction between host-related factors and disease mechanisms.The development of a predictive model based on the identified premorbid and comorbid factors represents a significant practical outcome of the study. The ability to stratify patients into different risk categories provides an opportunity for early intervention, targeted prevention, and optimization of clinical management strategies. In this context, the proposed approach may contribute to reducing the burden on healthcare systems by prioritizing high-risk patients and improving resource allocation.Furthermore, the results emphasize the importance of integrating epidemiological, clinical, and laboratory data in order to achieve a more comprehensive understanding of disease dynamics. Such an integrated approach allows not only for more accurate risk prediction but also for the identification of modifiable factors, such as smoking and physical inactivity, which can be addressed through preventive programmes.At the same time, certain limitations should be considered. The study was conducted within a specific regional population, which may affect the generalizability of the findings to other settings. In addition, although a wide range of factors was analysed, the potential influence of environmental exposures and genetic predisposition requires further investigation. Future studies should focus on expanding the dataset, incorporating longitudinal observations, and validating the predictive model in different populations.Overall, the findings of this study highlight the critical role of premorbid and comorbid conditions in shaping the clinical course of COVID-19–associated lung injury. The proposed predictive and preventive framework offers a promising direction for improving patient outcomes and reducing the impact of the disease at both clinical and population levels.
5. Conclusions
- The results of this study confirm that premorbid and comorbid conditions play a decisive role in the development and progression of COVID-19–associated lung injury. The integrated analysis of epidemiological, clinical, and laboratory data enabled the identification of key determinants influencing disease severity, including overweight status, arterial hypertension, smoking, physical inactivity, and immune-related alterations, as well as major comorbid conditions such as bronchial asthma, chronic obstructive pulmonary disease, cardiovascular disorders, and other systemic pathologies.Based on these findings, a mathematical model was developed to assess the combined impact of premorbid and comorbid factors and to determine their predictive significance. The proposed model allows stratification of patients into distinct risk categories, including very high, high, low, and very low risk groups, thereby providing a practical tool for early identification of vulnerable populations.Importantly, the implementation of a regionally adapted preventive programme demonstrated its potential applicability in clinical and public health practice. The proposed approach, exemplified by the Fergana Valley model, offers an effective and optimized strategy for reducing the incidence and severity of COVID-19–associated lung injury through targeted prevention, early diagnosis, and risk-oriented management.Overall, the study highlights the importance of integrating predictive modelling with preventive medicine to improve patient outcomes, reduce complications, and enhance the efficiency of healthcare systems in the context of emerging infectious diseases.
ACKNOWLEDGEMENTS
- The authors express their sincere gratitude to the leadership of Andijan State Medical Institute for their institutional support and assistance in facilitating this research. The authors also acknowledge the contribution of medical and laboratory staff involved in data collection and analysis.
DISCLOSURE
- The authors declare that there are no conflicts of interest regarding the publication of this paper.No external funding was received for this study, and no third-party individuals or organizations influenced the design, analysis, or interpretation of the results.