-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(6): 2841-2845
doi:10.5923/j.ajmms.20261606.16
Received: Apr. 23, 2026; Accepted: May 20, 2026; Published: Jun. 2, 2026

Osteosynthesis of Distal Femur Fractures Depending on the Degree of Deformity
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAziz Pulatovich Alimov1, Sadulla Nabievich Abdurakhimov2, Ekhsondavlat Mingziyaevich Shukurov3, Zinnat Egamberdievich Sapaev3
1Doctor of Medical Sciences, Head of the Department of Adult Traumatology, Republican Specialized Scientific and Practical Medical Center of Traumatology and Orthopedics
2Postgraduate Student, Department of Adult Traumatology, Republican Specialized Scientific and Practical Medical Center of Traumatology and Orthopedics
3Staff Member, Department of Adult Traumatology, Republican Specialized Scientific and Practical Medical Center of Traumatology and Orthopedics
Correspondence to: Aziz Pulatovich Alimov, Doctor of Medical Sciences, Head of the Department of Adult Traumatology, Republican Specialized Scientific and Practical Medical Center of Traumatology and Orthopedics.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Background. Distal femur fractures are relatively rare, but represent one of the most complex and clinically significant types of injuries. In this type of fractures, complications such as pseudoarthrosis, delayed bone union, and limitation of knee joint motion occur with high frequency. Epidemiological studies show that distal femur fractures are more common in two main populations. The first group consists of young and working-age individuals exposed to high-energy trauma. These cases are mainly associated with road traffic accidents, industrial injuries, and sports trauma. The second group includes elderly patients, in whom these fractures most often occur as a result of osteoporosis and low-energy trauma. Effective treatment of such fractures, early mobilization of patients, and restoration of quality of life are among the important tasks of modern medicine. Aim of the study. In this article, we evaluated the outcomes of surgical treatment of distal femur fractures by selecting the method of osteosynthesis based on the bone axis and the degree of diastasis. Materials and Methods. In the Department of Adult Traumatology of the Republican Scientific and Practical Medical Center of Traumatology and Orthopedics, 48 patients with distal femur fractures were treated using this method during the period 2022–2024. Surgical procedures were performed using both open and closed techniques with locking plates and retrograde intramedullary nails. Based on radiological and CT examinations of distal femur fractures, bone deformities were classified into the required categories. An algorithm was developed that allows selection of the surgical method depending on the degree of deformity. According to this algorithm, among the observed patients, 8 underwent osteosynthesis using open reduction and plating, 17 underwent osteosynthesis using open or closed reduction with locking intramedullary nails and screws, and 23 patients were treated with minimally invasive osteosynthesis using a distractor and retrograde locking nail. Results. According to our results based on the VAS (Visual Analog Scale), in surgeries performed using closed techniques, the level of pain decreased twofold within 3–7 days. According to the LEFS (Lower Extremity Functional Scale), functional activity reached 54.3 ± 3.8 points at 1 month after surgery, which is significantly higher compared to patients treated with conventional methods (45.2 ± 4.7). According to the SF-36 (Short Form (36) Health Survey), the components of physical activity, pain, and mental condition were recorded above 70 points in the main group. Conclusion. The effectiveness of the developed algorithm in practice lies in the fact that it can help determine
Keywords: Distal femur fractures, Osteosynthesis, Degree of deformity, Bone axis, Diastasis, Minimally invasive osteosynthesis
Cite this paper: Aziz Pulatovich Alimov, Sadulla Nabievich Abdurakhimov, Ekhsondavlat Mingziyaevich Shukurov, Zinnat Egamberdievich Sapaev, Osteosynthesis of Distal Femur Fractures Depending on the Degree of Deformity, American Journal of Medicine and Medical Sciences, Vol. 16 No. 6, 2026, pp. 2841-2845. doi: 10.5923/j.ajmms.20261606.16.
Article Outline
1. Introduction
- Distal femur fractures are relatively rare in the field of traumatology and orthopedics; however, they represent one of the most complex and clinically significant types of injuries. These types of fractures most often occur as a result of high-energy trauma and present considerable challenges in treatment due to their comminuted structure, involvement of the articular surface, and complications associated with soft tissue damage [1]. Epidemiological studies indicate that distal femur fractures are more common in two main populations. The first group consists of young and working-age individuals exposed to high-energy trauma. These cases are mainly associated with road traffic accidents, industrial injuries, and sports trauma [2]. The second group includes elderly patients, in whom these fractures most often occur as a result of osteoporosis and low-energy trauma [1,3]. Effective treatment of such fractures, early mobilization of patients, and restoration of quality of life are among the important tasks of modern medicine.The topic of surgical treatment of distal femur fractures encompasses a very wide range of information, and it is a difficult task to fully cover all its aspects.The main principles of treatment are carried out in the following stages: if the articular surface is disrupted as a result of the fracture, the joint must first be restored. In the surgical field, the knee joint surface of the distal femur must be free and mobile. At the next stage, the problem of eliminating displacement of the epiphysis and metaphysis of the distal femur is addressed [4].With the historical development of medicine, the treatment of such fractures has transitioned from conservative methods to operative methods using various implants [5]. However, the selection of the optimal implant remains a challenging issue that requires evidence-based decision-making. Currently, the most widely used methods are osteosynthesis using retrograde intramedullary nails and locking plates with screws. Both methods have certain advantages and disadvantages [6]. There are limited studies directly comparing modern implants. Differences between implants may depend on the treatment method, fracture type, and the prevalence of implant use [7]. In extra-articular fractures, both implant methods are used with approximately equal frequency [8]. In intra-articular and periprosthetic fractures, treatment with locking plates is more commonly used [9] [10].Such fractures are characterized by a high degree of injury severity, limited mobility, and delayed union. Even when widely applied, complication rates remain high, and according to the literature, the rate of nonunion can reach up to 22% [11].Effective treatment of such fractures, early mobilization of patients, and restoration of quality of life remain important tasks of modern medicine.In recent years, minimally invasive osteosynthesis techniques have been widely introduced [12,13]. These methods allow repositioning of bone fragments and their fixation through small incisions [14;15]. Minimally invasive osteosynthesis is distinguished from traditional open methods by reduced soft tissue injury, lower blood loss, faster recovery, and a lower rate of infectious complications [16].From this perspective, the present study was conducted with the aim of improving osteosynthesis outcomes in order to reduce complications in distal femur fractures.
2. Materials and Methods
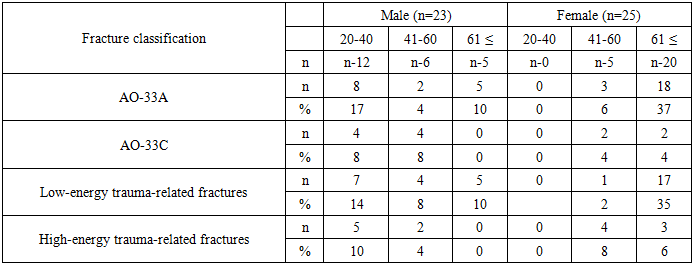
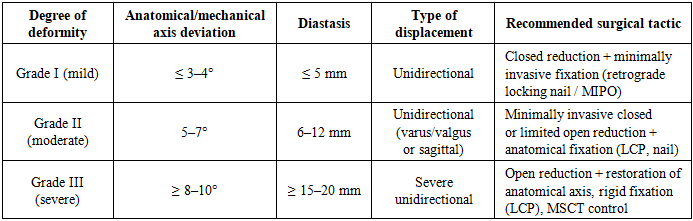
- In this study, as clinical material, data from 48 patients diagnosed with distal femur fractures were observed and analyzed over a period of 24 months. All patients were treated and monitored in inpatient settings at the Department of Adult Traumatology of the Republican Specialized Scientific and Practical Medical Center of Traumatology and Orthopedics during the period from 2022 to 2024. The condition of these patients and the treatment processes were comprehensively collected through full medical documentation, including medical history (anamnesis), surgical procedure protocols, radiological imaging (radiography, MSCT), results of functional assessments, osteodensitometry data, and statistical analyses comparing preoperative and postoperative conditions. These data not only ensured the scientific validity of the study but also enabled the development of precise recommendations in the clinical decision-making process.The age of the patients ranged from 20 to 84 years. Patients who could not be followed up due to various reasons (loss of contact, failure to return for follow-up, etc.) were excluded. The most common age group was 39–79 years, representing the working and physically active population. This indicates that distal femur fractures most often occur either on the background of osteoporosis or as a result of mechanical trauma.In our observations, the gender distribution of patients showed a predominance of males. Males: 23 patients (47.8%); Females: 25 patients (52%) (Table 1). The higher incidence among older women compared to younger women is mainly explained by postmenopausal osteoporosis.
|
|
|

|
3. Results
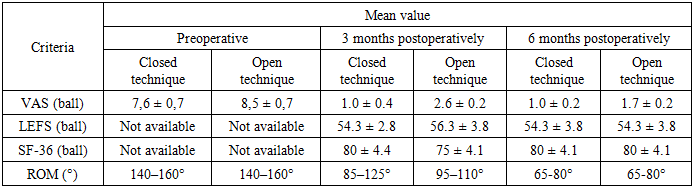
- Significant changes were identified in the preoperative and postoperative results according to the VAS scale. It was not possible to assess preoperative results using the LEFS and SF-36 criteria; however, improvements in outcomes were observed during follow-up examinations at 3–6 months after surgery (Table 5). Within 2–3 weeks after surgery, knee joint mobility was restored to 90%, and this process was observed earlier in younger patients. However, in patients treated for intra-articular fractures, recovery of knee joint function progressed more slowly compared to others.
|
|

4. Discussion
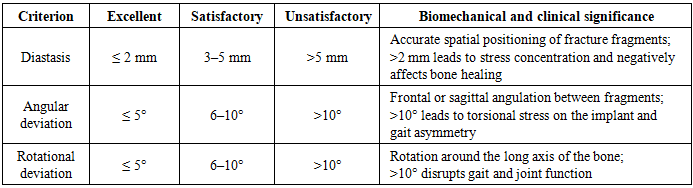
- Scientific studies indicate that neglecting changes in bone axes and diastasis resulting from fractures when selecting the osteosynthesis method leads to a decrease in positive functional outcomes. Minimally invasive osteosynthesis allows preservation of periosteal blood supply and soft tissue envelope with minimal disruption. Due to the load-sharing characteristics of intramedullary osteosynthesis performed using minimally invasive or open methods, gradual weight-bearing on the operated limb is recommended to prevent complications.
5. Conclusions
- In the osteosynthesis of distal femur fractures using a closed retrograde method, analysis of surgical outcomes taking into account the bone axis and diastasis revealed a higher proportion of positive results. In patients belonging to the first and second degree deformity groups, minimally invasive procedures with anatomical near-reduction of bone fragments increased the likelihood of faster functional recovery and a complication-free course. In patients with third-degree deformity, surgical outcomes achieved by open correction of deformity showed significantly better results compared to procedures performed without anatomical restoration.
Conflict of Interest
- The authors declare that there is no conflict of interest.
Ethical Approval and Consent
- Informed consent was obtained from all participants included in the study.