-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(6): 2832-2834
doi:10.5923/j.ajmms.20261606.14
Received: Apr. 18, 2026; Accepted: May 20, 2026; Published: Jun. 2, 2026

Assessment of Early Markers of Kidney Damage in Military Personnel Suffering from Arterial Hypertension and Comorbid Diseases
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLUsmanova D. U.1, Mukhamedova M. G.2, Alimov U. S.3
1Center for the Development of Professional Qualifications of Medical Workers, Tashkent, Uzbekistan
2Military Medical Institute of the University of Military Security and Defense of the Republic of Uzbekistan, Tashkent, Uzbekistan
3Tashkent State Medical University, Tashkent, Uzbekistan
Correspondence to: Usmanova D. U., Center for the Development of Professional Qualifications of Medical Workers, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The article presents the results of assessing the prognostic significance of early markers of kidney damage-albuminuria and glomerular filtration rate (GFR) – in military personnel with arterial hypertension and comorbid pathology. 70 military personnel were examined (38 of them with arterial hypertension, without concomitant comorbid conditions; 32 with arterial hypertension and comorbid pathology). Albumin-creatinine ratio (ACR) and GFR were measured in all subjects. In the group with comorbid pathology, albuminuria occurred in 62.5% of cases, and in the AH group without comorbid conditions—in 26.3% (p=0.002). The average GFR in the comorbid group was lower than in the first group (87.52 vs. 98.74 ml/min/1.73 m2; p=0.004). Conclusion: in military personnel with comorbid pathology, early markers of kidney damage are much more common, so this category needs more regular screening.
Keywords: Arterial hypertension, Military personnel, Cardiorenal syndrome, Glomerular filtration rate, Albuminuria, Microalbuminuria
Cite this paper: Usmanova D. U., Mukhamedova M. G., Alimov U. S., Assessment of Early Markers of Kidney Damage in Military Personnel Suffering from Arterial Hypertension and Comorbid Diseases, American Journal of Medicine and Medical Sciences, Vol. 16 No. 6, 2026, pp. 2832-2834. doi: 10.5923/j.ajmms.20261606.14.
1. Introduction
- Cardiorenal syndrome (CRS) refers to the interrelated dysfunction of the cardiovascular and renal systems, which is one of the urgent problems of modern medicine [1,2]. Recent studies have shown that such markers of kidney damage as albuminuria and decreased glomerular filtration rate (GFR) are already evident at the initial stages of the cardiorenal continuum [3,4].Albuminuria, especially microalbuminuria, is a reliable marker of early damage to the glomerular system of the kidneys. According to the international recommendations of KDIGO (2024), GFR and albuminuria levels are the basis for determining the stage of chronic kidney diseases, while these indicators play a key role in the stratification of cardiorenal risk [5].The contingent of military personnel is a special risk group for the development of cardiovascular diseases. Such factors as high psychoemotional stress, irregular physical activity, sleep disorders, and post-traumatic stress are factors that determine the early development of arterial hypertension (AH), obesity, diabetes mellitus, and coronary heart disease (CHD) in military personnel [6,7,8].Currently, early markers of kidney damage in military personnel with hypertension and comorbid pathology are insufficiently studied. The available literature mainly presents data on the general population, while there are few adapted recommendations for the military contingent [9,10].Purpose of the studyTo assess early markers of kidney damage-albuminuria (ACS) and glomerular filtration rate (GFR) – in military personnel with arterial hypertension and comorbid pathology (obesity, diabetes mellitus, coronary heart disease).
2. Material and Methods
- The study was conducted in a cross-sectional, observational analytical design. The study included 70 military personnel aged 19-55 years who were examined and treated in the Cardiorheumatology Department of the Central Military Clinical Hospital of the Ministry of Defense of the Republic of Uzbekistan in 2024-2025. All patients were divided into two groups: Group 1 (AH group, n=38): military personnel with grade I-III arterial hypertension, but without concomitant comorbid pathology (diabetes mellitus, coronary heart disease). Group 2 (AH + comorbid, n=32): patients with arterial hypertension in combination with comorbid pathology (type 2 diabetes mellitus, obesity and / or coronary heart disease).
3. Results
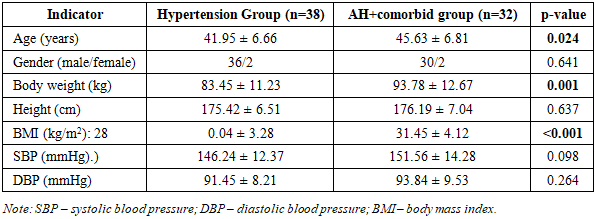
- Clinical and demographic characteristics of groups. As shown in Table 1, the mean age of patients in the AH + comorbid group was significantly higher (45.63±6.81 vs. 41.95±6.66 years; p=0.024) and they also had a higher body mass index compared to the AH group (31.45±4.12 vs. 28.04±3.28 kg/m2; p<0.001). The mean SBP and DBP values in the AH + comorbid group were slightly higher than in the AH group (151.56 ± 14.28 versus 146.24 ± 12.37 and 93.84 ± 9.53 versus 91.45 ± 8.21, respectively), although this difference was statistically insignificant. There were no statistically significant differences in gender composition between the groups (p=0.641).
|
|

|

4. Discussion
- The present study shows that in military personnel with arterial hypertension and comorbid pathology, early markers of kidney damage—albuminuria and decreased GFR—are detected significantly more often than in military personnel with hypertension alone.A statistically significant decrease in GFR (87.52±18.36 vs. 98.74±14.21 ml/min/1.73 m2; p=0.004) and an increase in creatinine and urea levels in patients in the AH + comorbid group indicate a significant deterioration in renal function against the background of comorbid pathology. These results are consistent with the data obtained by Efremovtseva (2016) in patients with stage 3-4 chronic kidney disease [11].The high incidence of albuminuria deserves special attention. Thus, ACN ≥30 mg/g was detected in 62.5% of patients in the AH + comorbid group, while in the group with isolated AH, this indicator was 26.3% (p=0.002). It is especially significant that microalbuminuria (A2) in the comorbid group occurred in 50.0% of cases, which is more than twice as high as in the AH group (p=0.022).Detection of microalbuminuria is of great clinical importance. According to the KDIGO 2024 guidelines, microalbuminuria is an independent prognostic marker of not only kidney damage, but also systemic endothelial dysfunction with the development of cardiovascular complications [5,12]. The high frequency of microalbuminuria in the comorbid group in our study indicates a high risk of developing cardiorenal syndrome in these patients.It should be noted that the incidence of albuminuria was significantly higher in patients with hypertension lasting more than 5 years. This is due to the damaging effect of prolonged hypertension on the glomerular apparatus. A persistent increase in blood pressure increases the pressure in the glomerular capillaries, leading to podocyte damage and, as a consequence, to the development of albuminuria [13,14].The results of our study are consistent with data from a study published by Aletras et al. (2025). In this study, albuminuria and decreased GFR are described as early and reliable markers of kidney damage in patients with cardiorenal syndrome [15].A study conducted by Kobalava et al. (2024) also confirmed that albuminuria is an important marker of not only kidney damage, but also systemic stagnation and poor prognosis [9]. Thus, the high frequency of microalbuminuria in the comorbid group in our study indicates a high risk of cardiorenal complications in these patients.
5. Conclusions
- 1. Military personnel with arterial hypertension and comorbid pathology (obesity, diabetes mellitus, coronary heart disease) have a more pronounced decrease in kidney function compared to military personnel with isolated hypertension. GFR in the comorbid group was 87.52±18.36 ml/min/1.73 m2, which is statistically significantly lower than in the group with hypertension alone (98.74±14.21 ml/min/1.73 m2; p=0.004).2. The incidence of albuminuria (ACC ≥30 mg/g) in the AH + comorbid group was significantly higher than in the AH group (62.5% of cases, versus 26.3%, respectively; p=0.002). Microalbuminuria (A2) was detected in 50.0% of cases in the comorbid group, while in the AH group this indicator was 23.7% (p=0.022).3. Albuminuria, especially microalbuminuria, is a reliable marker for early diagnosis of cardiorenal syndrome in military personnel, and also has an important prognostic value. Military personnel with detected microalbuminuria belong to the high-risk cardiorenal group and need in-depth examination and active preventive measures.4. Regular (at least once a year) screening of renal function indicators (GFR, creatinine) and albuminuria in military personnel is recommended, especially in the presence of comorbid pathology. This will contribute to the early start of a renoprotective strategy, prevent the development of cardiorenal complications, and preserve the health and combat capability of military personnel.