-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(6): 2827-2831
doi:10.5923/j.ajmms.20261606.13
Received: May 8, 2026; Accepted: May 22, 2026; Published: Jun. 2, 2026

Integrated Computed Tomography and Biomarker Evaluation of Myosteatosis Associated with Sarcopenia in Palliative Oncogynecological Patients
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLShakhanova Shakhnoza Shavkatovna1, Khoshimov Bakhodir Bakhromovich2, Ibragimova Leyla Ilkhomovna3
1Associate Professor, Department of Oncology, Samarkand State Medical University, Samarkand, Uzbekistan
2Research Applicant, Department of Oncology, Samarkand State Medical University, Samarkand, Uzbekistan
3Student, Samarkand State Medical University, Samarkand, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Background: Myosteatosis and sarcopenia are important manifestations of cancer-associated muscle deterioration, particularly in palliative oncology patients, and are associated with poor clinical outcomes. Objective: To evaluate the diagnostic value of computed tomography in detecting myosteatosis associated with sarcopenia in palliative patients with oncogynecological malignancies. Materials and Methods: A prospective single-center study included 65 patients with advanced oncogynecological malignancies receiving palliative care. CT-based body composition assessment was performed at the L3 vertebral level with evaluation of skeletal muscle index (SMI), skeletal muscle density (SMD), and intermuscular adipose tissue (IMAT). Laboratory markers included albumin, CRP, and IL-6. Results: Sarcopenia was identified in 63.1% of patients, myosteatosis in 55.4%, and the combined phenotype in 47.7%. Patients with myosteatosis had significantly lower SMI (34.2 ± 4.1 vs 41.8 ± 3.7 cm²/m²), lower SMD (27.4 ± 6.2 vs 39.1 ± 5.4 HU), higher IMAT (14.8 ± 3.6 vs 7.1 ± 2.2 cm²), lower albumin, and higher CRP and IL-6 levels (p < 0.05). Conclusion: CT assessment at the L3 level is an effective method for diagnosing myosteatosis in palliative oncogynecological patients. Myosteatosis is associated with systemic inflammation, nutritional deficiency, and severe muscle deterioration, making it a clinically relevant prognostic biomarker.
Keywords: Myosteatosis, Sarcopenia, Computed tomography, Oncogynecology, Palliative care
Cite this paper: Shakhanova Shakhnoza Shavkatovna, Khoshimov Bakhodir Bakhromovich, Ibragimova Leyla Ilkhomovna, Integrated Computed Tomography and Biomarker Evaluation of Myosteatosis Associated with Sarcopenia in Palliative Oncogynecological Patients, American Journal of Medicine and Medical Sciences, Vol. 16 No. 6, 2026, pp. 2827-2831. doi: 10.5923/j.ajmms.20261606.13.
1. Introduction
- Modern clinical oncology is increasingly focused not only on the morphological characteristics of the tumor process but also on the objective assessment of the patient’s functional and metabolic status, which significantly determines treatment effectiveness and disease prognosis. One of the most significant manifestations of tumor-associated metabolic disorders is sarcopenia, characterized by a progressive decline in skeletal muscle mass, strength, and functional capacity. In oncological practice, sarcopenia is regarded as an independent predictor of increased systemic therapy toxicity, postoperative complications, impaired quality of life, and reduced overall survival [8,11].According to current concepts, myosteatosis is considered not merely a morphological alteration of muscle tissue, but also an independent biological marker of systemic metabolic dysfunction, chronic inflammation, and cancer cachexia [3,6]. International studies report that the prevalence of myosteatosis among oncology patients ranges from 25% to 78%, depending on tumor type, patient age, disease stage, and diagnostic criteria applied [1,2,3]. The presence of myosteatosis has been associated with a significantly increased risk of postoperative complications, systemic chemotherapy toxicity, infectious complications, prolonged hospitalization, and decreased overall survival [2,11].Recent studies suggest that qualitative muscle deterioration may have greater prognostic significance than isolated muscle mass reduction. Daly et al. demonstrated that reduced skeletal muscle radiodensity measured by computed tomography is an independent predictor of adverse outcomes in cancer patients, even in cases with relatively preserved skeletal muscle volume [4]. Similar findings were reported by Xiao et al., who showed that myosteatosis is closely associated with the severity of systemic inflammatory response and functional impairment in oncology patients [5].The pathogenesis of myosteatosis in cancer patients is multifactorial. Chronic tumor intoxication, hypercatabolism, protein metabolism disturbances, mitochondrial dysfunction, insulin resistance, and persistent inflammation contribute to the progressive replacement of muscle tissue with lipid components [6,9]. Pro-inflammatory cytokines, particularly interleukin-6 (IL-6), tumor necrosis factor-alpha (TNF-α), and C-reactive protein (CRP), play a crucial role by activating proteolytic pathways and disrupting myogenesis [6]. Chronic inflammation is considered one of the central mechanisms underlying the development of the sarcopenic phenotype in malignant diseases [6].This issue is of particular clinical relevance in gynecologic oncology. Patients with cervical cancer, ovarian cancer, endometrial cancer, and other malignancies of the female reproductive system represent a high-risk group for metabolic disturbances due to the combined effects of tumor burden, surgical treatment, polychemotherapy, radiotherapy, chronic pain, nutritional deficiency, and forced physical inactivity [6,9]. According to Rutten et al., sarcopenia is detected in 20–54% of patients with ovarian cancer and significantly worsens treatment outcomes [7]. Similar observations indicate the adverse impact of muscle degradation on the clinical course of endometrial and cervical cancers [7,11].Despite growing interest in sarcopenia in oncology, the diagnostic approach to myosteatosis in gynecologic oncology remains insufficiently standardized. Most clinical studies primarily focus on the quantitative assessment of muscle mass, whereas qualitative structural alterations in skeletal muscle remain considerably less investigated. Computed tomography is currently considered one of the most objective methods for body composition assessment, as it enables simultaneous evaluation of skeletal muscle area and radiological muscle density, reflecting the degree of fatty infiltration [4,5,10].Aim of the studyTo evaluate the diagnostic value of computed tomography-based assessment of myosteatosis associated with sarcopenia in palliative patients with oncogynecological malignancies and to determine its relationship with inflammatory and nutritional-metabolic parameters.
2. Materials and Methods
- A single-center prospective clinical study was conducted at the oncology palliative care department.The study included 65 patients with morphologically confirmed advanced oncogynecological malignant neoplasms.
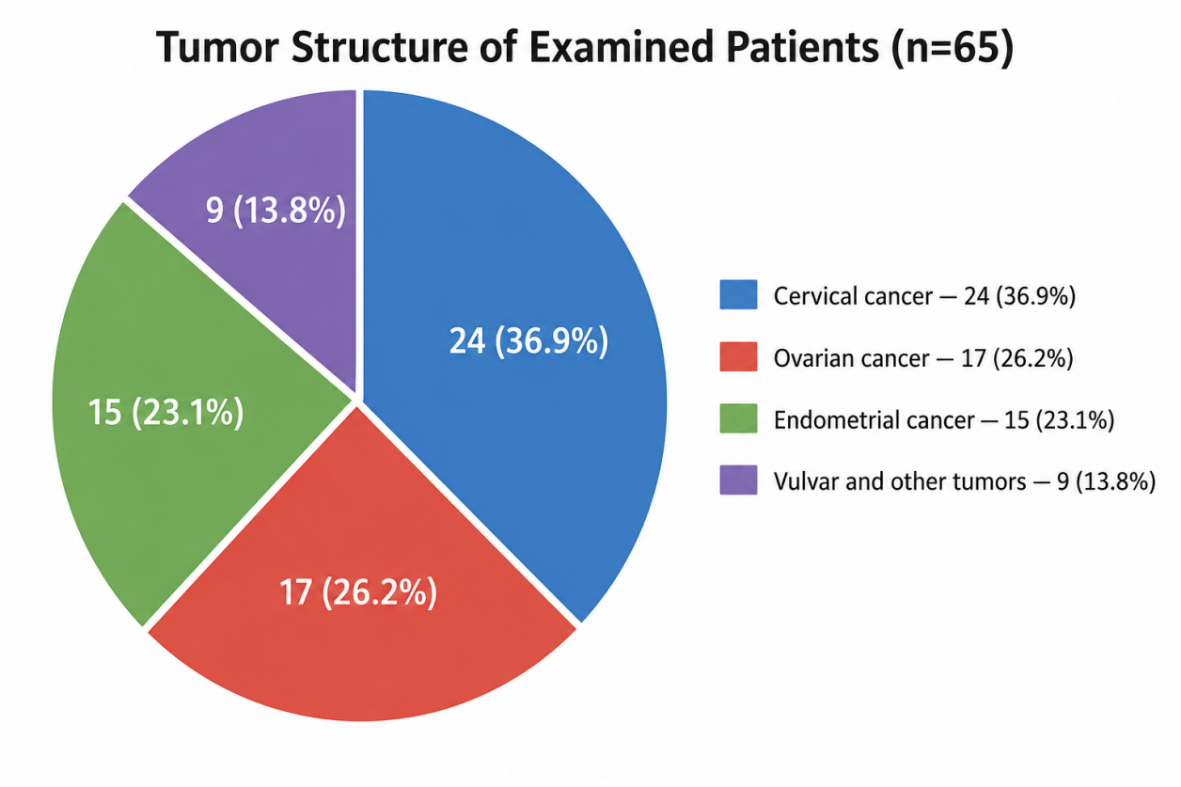 | Figure 1. Distribution of examined patients according to tumor localization (n = 65) |
3. Results
- Sarcopenia was diagnosed in 41 patients (63.1%).Myosteatosis was identified in 36 patients (55.4%).The combined phenotype of sarcopenia and myosteatosis was observed in 31 patients (47.7%).
|
4. Discussion
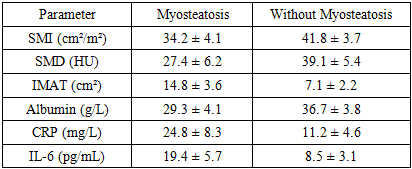
- The obtained results demonstrate a high prevalence of skeletal muscle composition abnormalities among palliative patients with oncogynecological malignancies. Sarcopenia was diagnosed in 63.1% of the examined patients, myosteatosis in 55.4%, while the combined phenotype was identified in nearly half of the cohort (47.7%). These findings indicate that skeletal muscle alterations in patients with advanced oncogynecological malignancies are characterized not only by quantitative muscle loss but also by pronounced qualitative structural deterioration.The high prevalence of sarcopenia in this patient population is expected, as malignant disease progression is accompanied by severe hypercatabolism, systemic inflammatory response, reduced physical activity, nutritional deficiency, and cancer-associated cachexia. However, particular clinical interest is associated with myosteatosis, which reflects pathological fatty infiltration of skeletal muscle and is currently recognized as an independent adverse prognostic factor in oncology patients.Comparative analysis of computed tomography parameters revealed a statistically significant reduction in the skeletal muscle index (SMI) in patients with myosteatosis compared with those without evidence of fatty muscle degeneration (34.2 ± 4.1 vs 41.8 ± 3.7 cm²/m²; p < 0.05). This finding confirms the close pathophysiological relationship between quantitative muscle depletion and qualitative structural muscle deterioration. Reduced SMI in patients with myosteatosis suggests more severe muscle wasting and profound metabolic decompensation.The most indicative marker of qualitative muscle impairment was the reduction in skeletal muscle radiodensity (SMD). In patients with myosteatosis, the mean SMD was 27.4 ± 6.2 HU, whereas in patients without myosteatosis it reached 39.1 ± 5.4 HU (p < 0.05). Reduced muscle density reflects intramuscular lipid accumulation and serves as an objective CT-based marker of myosteatosis. These alterations indicate significant disruption of muscle architecture, diminished contractile capacity, and progressive functional impairment of the muscular system.Additional confirmation of severe fatty degeneration was provided by the increased volume of intermuscular adipose tissue (IMAT), which was more than twofold higher in patients with myosteatosis compared with the control group (14.8 ± 3.6 vs 7.1 ± 2.2; p < 0.05). Increased IMAT reflects not only localized fat redistribution but also systemic metabolic disturbances associated with chronic inflammation, insulin resistance, and impaired lipid metabolism.
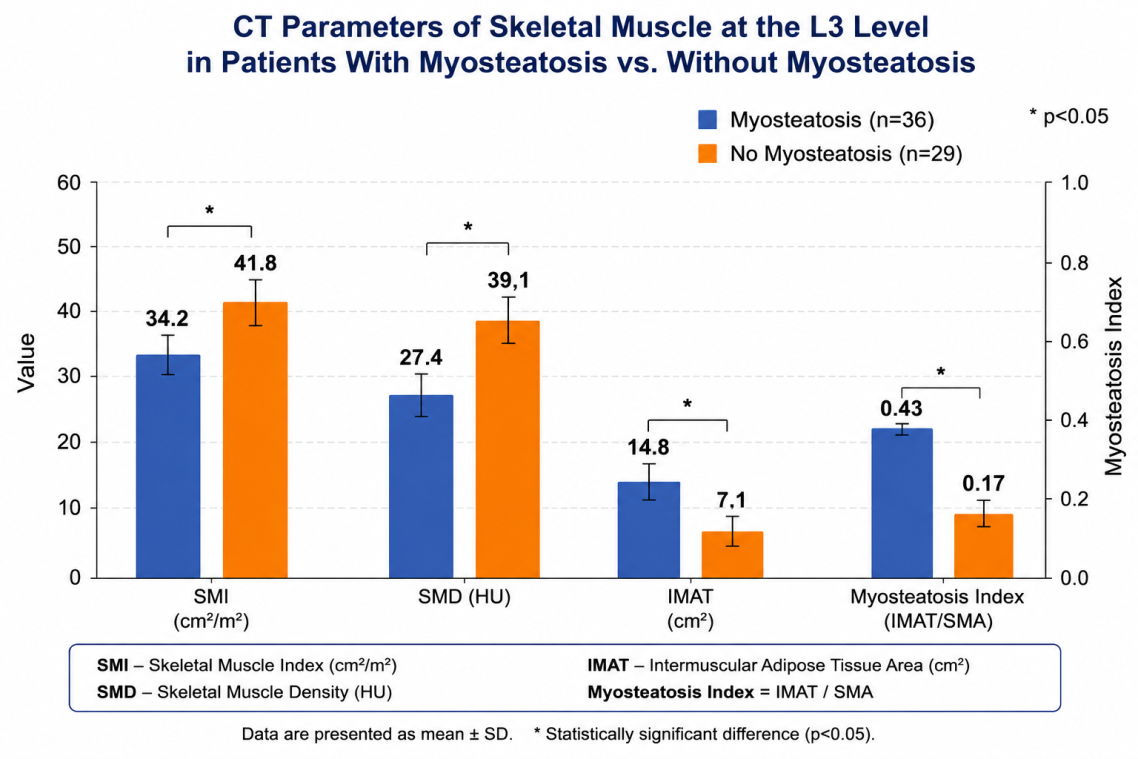 | Figure 2. Comparative CT assessment of skeletal muscle parameters at the L3 vertebral level in patients with and without myosteatosis |
5. Conclusions
- Myosteatosis is a highly prevalent and clinically significant component of skeletal muscle deterioration in palliative patients with oncogynecological malignancies. In the present study, sarcopenia was identified in 63.1% of patients, myosteatosis in 55.4%, and the combined phenotype in 47.7%, indicating a substantial burden of cancer-associated muscle pathology.Computed tomography assessment at the L3 vertebral level demonstrated high diagnostic utility for detecting both quantitative and qualitative skeletal muscle abnormalities. Patients with myosteatosis showed significantly lower skeletal muscle index and muscle density, along with markedly increased intermuscular adipose tissue, confirming profound structural muscle degeneration.The association of myosteatosis with hypoalbuminemia, elevated CRP, and increased IL-6 levels indicates that this condition reflects not only radiological muscle alteration but also severe systemic inflammation, metabolic dysregulation, and protein-energy deficiency.Therefore, myosteatosis should be regarded as an important imaging biomarker of adverse clinical status in palliative oncogynecological patients. Integration of CT-based body composition assessment into routine palliative oncology practice may improve risk stratification, facilitate early nutritional and anti-inflammatory interventions, and support personalized supportive care strategies.