-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(6): 2822-2826
doi:10.5923/j.ajmms.20261606.12
Received: Apr. 24, 2026; Accepted: May 15, 2026; Published: Jun. 2, 2026

Reconstructive and Restorative Interventions on the Right Ventricular Outflow Tract and Pulmonary Artery Trunk in Patients with Tetralogy of Fallot with Pulmonary Valve Annulus Hypoplasia
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLIsmailov S. M.1, Kobiljonov B. Kh.2, Abralov Kh. K.3, Kholmuratov A. A.4, Tashpulatov M. G.5
1MD, DSc (Medicine), Professor – Director, Republican Specialized Scientific and Practical Medical Center of Surgery named after Acad. V. Vakhidov (RSPC of Surgery)
2Resident Physician, Department No. 1 of Congenital Heart Surgery, RSPC of Surgery
3MD, DSc (Medicine), Professor, Department of General Surgery I, Center for the Development of Professional Qualifications of Medical Personnel
4MD, PhD (Medicine) – Head of Department No. 1 of Congenital Heart Surgery, RSPC of Surgery
5Master’s Degree Student, Republican Specialized Scientific and Practical Medical Center of Surgery named after Acad. V. Vakhidov
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Malformations of the right ventricular outflow tract (RVOT) and the fibrous ring of the pulmonary artery (PA annulus) account for a significant percentage of congenital heart defects. In recent years, there has been an increase in the number of patients requiring reinterventions due to insufficiency or stenosis of reconstructed segments at various postoperative intervals. Modern approaches to RVOT and PA annulus reconstruction involve the use of new biological and synthetic materials. The aim of this study is to analyze the relevance and trends in the development of contemporary surgical reconstruction techniques for the RVOT and main pulmonary artery, with a focus on improving the outcomes of radical correction and reducing the frequency of reoperations. This analysis is based on the use of modern diagnostic tools such as echocardiography (ECHO) and multislice computed tomography (MSCT).
Keywords: Radical correction, Main pulmonary artery, Reconstruction techniques
Cite this paper: Ismailov S. M., Kobiljonov B. Kh., Abralov Kh. K., Kholmuratov A. A., Tashpulatov M. G., Reconstructive and Restorative Interventions on the Right Ventricular Outflow Tract and Pulmonary Artery Trunk in Patients with Tetralogy of Fallot with Pulmonary Valve Annulus Hypoplasia, American Journal of Medicine and Medical Sciences, Vol. 16 No. 6, 2026, pp. 2822-2826. doi: 10.5923/j.ajmms.20261606.12.
1. Introduction
- The right ventricular outflow tract and the fibrous pulmonary annulus play a key role in intracardiac hemodynamics, especially in patients with congenital heart defects such as Tetralogy of Fallot, pulmonary atresia, truncus arteriosus, and others. Surgical correction strategies for these anomalies have significantly improved over recent decades. However, problems persist, particularly pulmonary valve apparatus insufficiency following transannular patch reconstruction and general pulmonary valve incompetence.The causes of functional valve insufficiency include structural disruption of the fibrous annulus framework, dissected valve leaflets, suboptimal performance of leaflets created from autologous or xenogeneic materials, implant degeneration, calcification, and size mismatch — all of which often lead to the need for reintervention.According to clinical registry data, up to 50%–57% of patients who undergo correction of defects involving the right ventricular outflow tract (RVOT) and/or the pulmonary artery (PA) annulus require reoperation within 10–15 years after the initial procedure.The main causes include:Functional insufficiency of the implanted valve structuresSize mismatch between the implanted materials (autologous or xenopericardial patches, conduits) and the patient’s somatic growthCalcification and stenosis of reconstructed segmentsDegeneration of biological materials used in homografts and bioprosthesesThus, there is a clinically significant need for new approaches to reconstruction that can ensure durability, functional competence, and adaptability in patients with Tetralogy of Fallot, particularly those with infundibular obstruction of the right ventricular outflow tract (RVOT) and hypoplasia of the fibrous annulus and main pulmonary artery trunk.This study focuses on reconstructive and restorative interventions of the RVOT and pulmonary artery trunk in patients with Tetralogy of Fallot, infundibular stenosis, and hypoplasia of the pulmonary valve annulus.The article also reviews modern diagnostic techniques aimed at detecting and accurately assessing the severity of infundibular stenosis, the degree of hypoplasia, and the dimensions of the pulmonary annulus.The diagnostic value of echocardiography and multislice computed tomography (MSCT) is discussed in the context of perioperative anatomical evaluation, surgical planning, and assessment of transannular patch (TAP) reconstruction of the RVOT and pulmonary artery trunk.Tetralogy of Fallot (TOF) is one of the most common congenital heart defects, characterized by four anatomical components: a ventricular septal defect (VSD), overriding aorta, obstruction of the right ventricular outflow tract (infundibular stenosis), and right ventricular hypertrophy.A frequent feature in patients with TOF is hypoplasia of the pulmonary valve annulus and main pulmonary artery, which further aggravates hemodynamic disturbances [1,2]. TOF accounts for up to 10% of all congenital heart defects and requires surgical correction in early childhood [3].The main goal of surgery is to eliminate the intracardiac shunt, restore adequate pulmonary blood flow, and achieve anatomical correction of cardiac anomalies [2]. However, in cases of pronounced infundibular obstruction and pulmonary annulus hypoplasia, complex reconstructive interventions are required to ensure the functional patency of the right ventricular outflow tract (RVOT) and pulmonary artery trunk.From an anatomical and functional standpoint, patients with Tetralogy of Fallot exhibit the following features:Infundibular stenosis — a narrowing of the right ventricular outflow tract caused by hypertrophy of the muscular bundles, leading to obstruction of blood flow.Hypoplasia of the pulmonary artery annulus — a congenital underdevelopment of the fibrous ring of the pulmonary valve, accompanied by a reduction in the diameter of the valve orifice and, in some cases, hypoplasia of the main pulmonary artery trunk and its branches [4,5].Among the main modern diagnostic methods, echocardiography (ECHO) and multislice computed tomography (MSCT) with contrast enhancement are widely used.1. Echocardiography (ECHO):Transthoracic echocardiography (TTE) is the primary screening method used to assess the linear and volumetric parameters of the heart and great vessels. It allows for the evaluation of the size and degree of narrowing of the right ventricular outflow tract and the measurement of the pulmonary annulus diameter. Using Doppler imaging, the systolic pressure gradient can also be determined.The next method, transesophageal echocardiography (TEE), is employed in cases of limited visualization, particularly in adolescents and adults.2. Multislice Computed Tomography (MSCT):MSCT plays an important role in the modern diagnosis of congenital heart defects, particularly Tetralogy of Fallot (TOF). It is used in the preoperative assessment of patients with TOF and is also valuable for evaluating the results of radical correction, including the visualization of shunts, stents, prosthetic materials, and the assessment of pulmonary artery patency.From a clinical perspective, the use of MSCT in the perioperative period for patients with Tetralogy of Fallot accompanied by hypoplasia of the pulmonary valve annulus and main pulmonary artery trunk provides several advantages. It yields high-precision data on the anatomical and functional parameters of the heart and great vessels, assisting in the selection of the optimal surgical approach.Based on MSCT findings, the required extent of surgical intervention can be determined, including:Isolated reconstruction of the right ventricular outflow tract (RVOT);Transannular patch (TAP) reconstruction of the RVOT and pulmonary trunk;TAP reconstruction of the RVOT and pulmonary trunk with the formation of a third neocusp, or the implantation of a conduit or angioplasty of the pulmonary artery branches, performed prior to radical correction.The aim of the present study is to analyze the outcomes of surgical treatment using transannular techniques and their specific features in patients with Tetralogy of Fallot who present with severe stenosis of the right ventricular outflow tract (RVOT), accompanied by hypoplasia of the fibrous annulus and pulmonary artery stenosis.
2. Materials and Methods
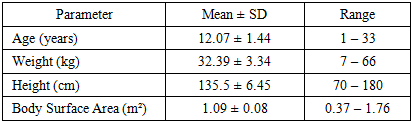
- The study presents an analysis of 28 patients who underwent reconstructive surgery with enlargement of the right ventricular outflow tract (RVOT), pulmonary valve annulus (PA annulus), and main pulmonary artery (PA trunk) using a developed and proposed transannular patch (TAP) technique for the RVOT, PA annulus, and PA trunk, involving the formation of a third neocusp of the pulmonary valve.An evaluation of early postoperative outcomes was conducted, including hemodynamic parameters, rate of complications, and need for reinterventions.From January 2018 to December 2023, at the Republican Specialized Scientific and Practical Medical Center of Surgery named after Acad. V. Vakhidov, 28 patients with Tetralogy of Fallot underwent radical correction in the Department of Congenital Heart Defects.Of these, 16 were boys and 12 were girls. In 26 patients, Tetralogy of Fallot was diagnosed, and in 3 cases, a double outlet right ventricle (DORV) of tetralogy type was identified.All patients underwent standard diagnostic protocols, including electrocardiography (ECG), echocardiography (ECHO), chest X-ray, multislice computed tomography (MSCT), and angiocardiography (ACG) when indicated. Comprehensive clinical and laboratory evaluations were also performed.The age of patients ranged from 1 to 33 years, with a mean age of 12.07 ± 1.44 years. The body weight ranged from 7.0 kg to 66 kg, with an average of 32.3 ± 3.34 kg. The anthropometric data corresponded to older age groups, which was associated with previous palliative surgeries (see Table 1).
|
|
|
|
3. Results and Discussions
- Additional resection of hypertrophied myocardial bundles in the RVOT was performed to relieve infundibular obstruction. Subsequently, ventricular septal defect (VSD) closure was carried out using a xenopericardial patch, fixed with a continuous 5-0 Prolene suture on a needle No. 13–17.The autopericardial patch was fashioned parallel to the sternum, measuring 8.0 × 1.0 cm in size.The next stage involved formation of the third cusp by duplicating and suturing the edges of the pericardial fold, creating a valve-like flap. The free edge of this flap was reinforced with interrupted 5-0 Prolene sutures, forming a frenulum (support band) of the free margin of the new cusp. [8]An additional interrupted 5-0 Prolene suture was placed at the base of the flap to fix it to the anterior wall of the pulmonary artery. In this way, a third neocusp was created, with a secured base and a frenulum supporting the free edge of the leaflet.Next, a Hegar dilator was selected according to body surface area (BSA) to determine the target diameter of the future pulmonary annulus. The dilator was inserted into the incised pulmonary trunk and annulus.Following this, the previously prepared patch was sutured along the free edge line of the newly formed third neocusp, attaching its sides to the incised edges of the pulmonary annulus. One continuous suture line was extended toward the pulmonary trunk to the end of the incision, while the other suture line was directed toward the right ventricular outflow tract (RVOT) to complete the reconstruction.The opposite edge of the RVOT, annulus, and pulmonary trunk was reconstructed in a similar manner.At the next stage, a strip of autopericardium, 3–4 mm wide and with a length corresponding to the diameter of the previously inserted Hegar dilator, was fashioned. This created a new, reconstructed pulmonary annulus with the required diameter based on BSA calculations.The edges of the pericardial strip were sutured at the level of the pulmonary annulus above the patch, in the area of the duplicated portion, using a continuous suture starting from the medial edge of the annulus and ending at its lateral edge.Thus, reconstructive enlargement of the right ventricular outflow tract (RVOT), pulmonary annulus, and pulmonary trunk through infundibular resection and transannular autopericardial patch reconstruction with the formation of a third neocusp ensures the functional competence of the pulmonary annulus and the creation of a tricuspid pulmonary valve structure. The early postoperative surgical mortality was 3.57% (1 patient). The cause of death was acute right ventricular failure combined with low cardiac output syndrome of the left ventricle, refractory to cardiotonic therapy.In three patients, right ventricular failure syndrome developed but was successfully managed with medical treatment.Reconstruction remained patent in all cases.The mean residual systolic pressure gradient between the right ventricle (RV) and pulmonary artery (PA) was 6 mmHg, and the RV/LV pressure ratio averaged 0.4. According to echocardiographic data, no pulmonary regurgitation was detected in any of the patients. The average duration of mechanical ventilation in the early postoperative period was 6 hours. All patients received cardiotonic therapy with standard doses of inotropic agents during the immediate postoperative period.
4. Conclusions
- In modern pediatric cardiac surgery, echocardiography (ECHO) and multislice computed tomography (MSCT), with high-precision determination of the Z-score for the pulmonary valve annulus and pulmonary trunk in patients with Tetralogy of Fallot, serve as both screening and decisive diagnostic tools for determining the surgical strategy. These modalities offer significant advantages and minimal limitations compared with MRI and angiocardiography (ACG), which are performed only when indicated.The developed technique of forming a third pulmonary valve neocusp during transannular patch (TAP) reconstruction allows achievement of a Z-score close to zero for the neopulmonary annulus, thereby eliminating the initial hypoplasia of the pulmonary annulus through the use of autologous pericardial tissue, while also preventing pulmonary valve regurgitation.The application of the proposed TAP technique with formation of a third neocusp and enlargement of the pulmonary fibrous annulus demonstrates favorable early postoperative outcomes, confirming its efficacy and functional reliability. Modern approaches employing valve-sparing techniques, such as the proposed method of transannular patch reconstruction (TAP) of the right ventricular outflow tract (RVOT) and pulmonary trunk (PT) with the formation of a third neocusp of appropriate dimensions and enlargement of the hypoplastic pulmonary annulus, provide both anatomically and functionally complete restoration of normal intracardiac hemodynamics.