Agababyan L. R., Kamalov A. I.
Samarkand State Medical University, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
The article highlights the results of an analysis aimed at assessing maternal and perinatal mortality rates in the Republic of Uzbekistan for 2020-2024 from the point of view of organizational management of obstetric care processes. The purpose of the study is to identify the factors associated with the organization of medical care in the occurrence of maternal and perinatal mortality, the system of routing, compliance with the rules of time, early risk assessment, and a comprehensive assessment of the preparedness of emergency obstetric care. Based on the methods of organizational-statistical and retrospective analysis, a comparative study of the results of the review of documents, clinical audit materials, and perinatal cases was conducted. During the analysis, it was shown that such management shortcomings as timely detection of dangerous situations, late referral to a high-level institution, disruptions in transportation and multidisciplinary cooperation, and shortcomings in compliance with protocols are priorities. As a conclusion, practical proposals were made to strengthen perinatal audit, standardize triage and routing, improve resuscitation preparation, and implement digital monitoring tools.
Keywords:
Maternal mortality, Perinatal mortality, Obstetric care, Organizational management, Routing, Triage, "Time" rules, Clinical audit, Quality control, Emergency obstetric care
Cite this paper: Agababyan L. R., Kamalov A. I., Analysis of Maternal and Perinatal Death in the Republic of Uzbekistan from the Point of View of Organizational Management of Obstetric Processes (2020-2024), American Journal of Medicine and Medical Sciences, Vol. 16 No. 6, 2026, pp. 2809-2813. doi: 10.5923/j.ajmms.20261606.09.
1. Introduction
Maternal and perinatal mortality are considered the ultimate adverse outcomes of obstetric and perinatal care processes, which develop at various stages of pregnancy, childbirth, and the postpartum period. Their rates and structures reflect the specific features of how medical care is organized, the timeliness of complication detection, the adequacy of patient referrals, adherence to time-based protocols, and the effectiveness of management decisions. Unlike clinical studies focused on analyzing the nosological structure of pregnancy and childbirth complications, an organizational analysis concentrates on the processes of medical care delivery. This includes the timely identification of high-risk situations, appropriate patient referrals, compliance with time regulations, the alignment of a medical facility's level with the level of clinical risk, and the readiness of personnel to act in critical situations. The objective of this research is to analyze maternal and perinatal mortality in the Republic of Uzbekistan from 2020 to 2024 from the perspective of the organizational management of obstetric and perinatal care processes, to identify manageable (modifiable) organizational deficiencies that contribute to mortality, and to develop practical organizational recommendations for their elimination.
2. Materials and Methods
In recent years, a multi-level system of obstetric care has been formed in the Republic of Uzbekistan, national clinical protocols for the management of complicated pregnancy and childbirth have been approved, and modern methods of intensive care and surgical intervention have been introduced. However, the persistence of maternal and perinatal mortality, as well as pronounced regional variability of indicators, indicate the presence of systemic defects in the organization of medical care, which cannot be eliminated only by clinical measures. Thus, in this study, maternal and perinatal mortality is considered not as a result of individual clinical errors, but as a result of general regulated processes that can be analyzed and corrected within the framework of the organizational and functional model.This chapter is based on the analysis of official statistical data of the Ministry of Health of the Republic of Uzbekistan for 2020-2024, as well as specially developed tools for individual data collection on each case of maternal and perinatal mortality. [1]Used as data sources:• state statistical reporting on maternal and perinatal mortality;• regional generalized data;• forms of expert assessment of deaths.The main methodological difference of this study is the inclusion of organizational-temporal parameters in the analysis, in particular:• level of the medical and preventive institution (I-III);• status, stage, and frequency of patient transfer;• time from admission to the start of medical care;• time from the onset of complications to the start of qualified assistance;• use of air ambulance;• conducting a clinical consultation;• expert assessment of mortality prevention. [2]
3. Research Results
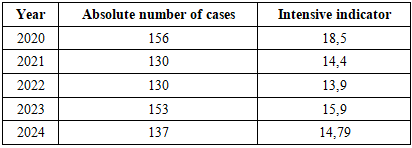
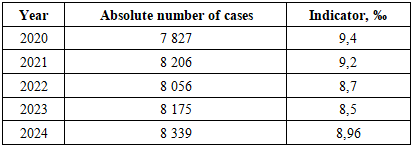
According to official statistics, 706 cases of maternal mortality were registered in the Republic of Uzbekistan during 2020-2024 (Table 1).Table 1. Dynamics of maternal mortality in the Republic of Uzbekistan
 |
| |
|
Analysis of the dynamics shows the absence of a steady downward trend. After a decline in the indicator in 2021-2022, an increase in the intensive indicator by 14.4% was recorded in 2023, which indicates the instability of the achieved results. In 2024, a partial decline was observed, but the indicator did not reach the minimum values of previous years. Such fluctuations in the availability of approved clinical protocols and organizational structures indicate inconsistencies in the implementation of management decisions at the regional and institutional levels. [3]One of the main parameters of the organizational analysis is the level of the medical institution where the patient was at the time of the development of a life-threatening complication. Reconstructed analysis of the distribution of maternal mortality by levels of medical institutions showed the following (Fig. 1):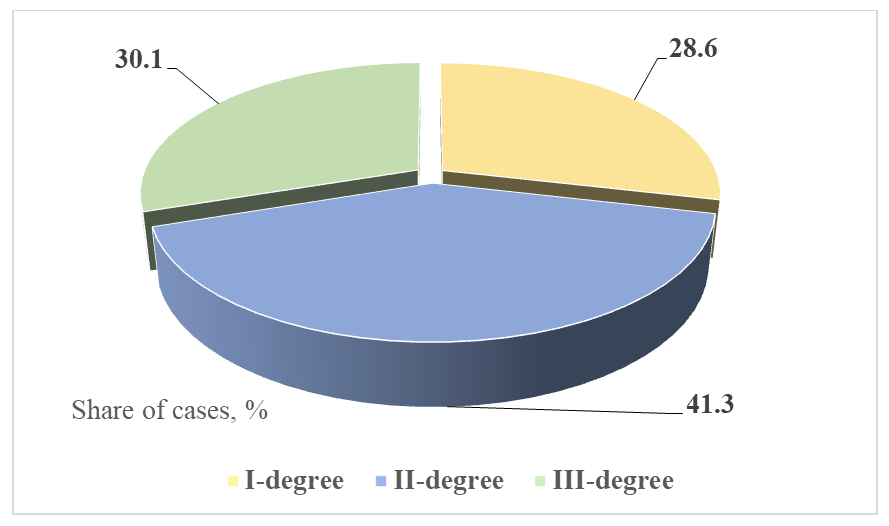 | Figure 1. Distribution of maternal mortality by level of PHC |
Thus, despite the fact that in most cases the clinical condition of patients requires specialized care, 69.9% of deaths occurred outside of third-degree institutions. Complications associated with I-II degrees were most often noted:• massive obstetric bleeding; [4]• severe forms of preeclampsia and eclampsia;• septic conditions.The fact of transfer of a patient between medical institutions was recorded in 57.4% of cases of maternal mortality (Fig. 2).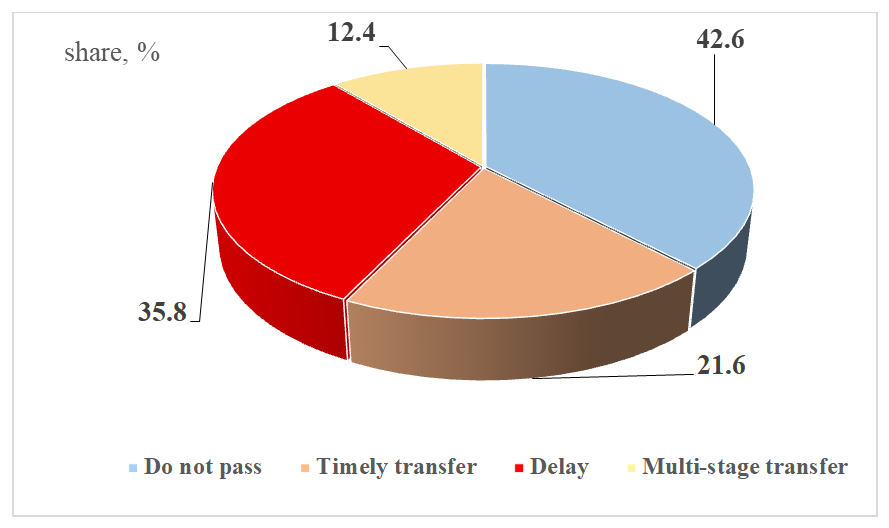 | Figure 2. Description of transfer in maternal mortality |
Late and multi-stage transplants were accompanied by deterioration of the patients' condition, the development of multiple organ failure, and the loss of therapeutic time. [5]As can be seen from Figure 3, in 62.3% of cases, the time before the start of qualified assistance exceeded the regulated values, which is a direct indicator of an organizational defect. Instructions for calling more qualified personnel for assistance via air ambulance were available in 31.5% of cases, while actual use was 2.5 times less, i.e., 14.2%. Consultations with relevant specialists and qualified doctors were conducted in 48.7%, however, changes in treatment tactics after the consultation were noted only in 22.9% of cases. [6]The results of the expert assessment of the prevention of OJ cases are presented in Figure 3.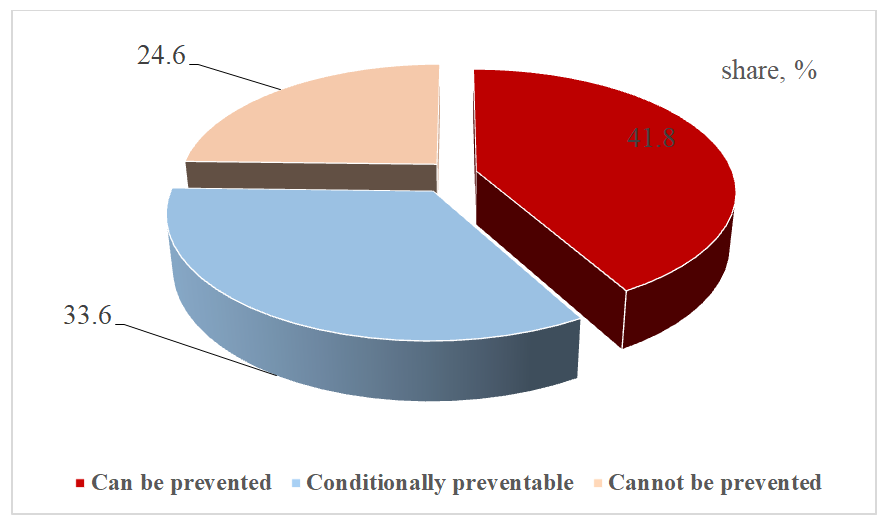 | Figure 3. Maternal mortality prevention |
The total share of preventable cases was 75.4%, which indicates the predominance of managed organizational factors in the structure of adverse outcomes and indicates the presence of a significant reserve for reducing maternal mortality by optimizing the processes of providing obstetric care, patient referral, and adherence to timing rules. [7]Perinatal mortality is an integral indicator formed under the influence of the quality of antenatal observation, timely hospitalization, the level of the maternity hospital, as well as the readiness of the neonatal service to provide intensive care to newborns. [8]According to official statistics, 40,603 cases of perinatal death were registered in the Republic of Uzbekistan in the period 2020-2024 (Table 2).Table 2. Dynamics of perinatal mortality in the Republic of Uzbekistan
 |
| |
|
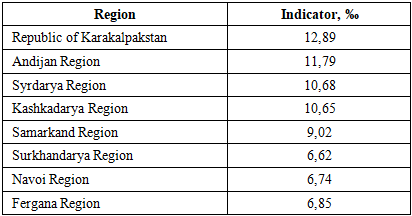
Despite a relative decrease in the indicator per thousand in 2022-2023, an increase of 5.4% compared to the previous year was noted in 2024. The absolute number of perinatal losses remained consistently high, which indicates the limited effectiveness of the measures being implemented. From the point of view of the organization of care, it is very important that more than 60% of perinatal losses are formed at the antenatal and intranatal stages, i.e., before the provision of specialized neonatal care. [9]This circumstance emphasizes the decisive role of the quality of antenatal observation and organization of delivery in the formation of perinatal outcomes. The predominance of losses at the preclinical and intranatal stages indicates the insufficient effectiveness of the system of early detection of high-risk pregnancy, timely hospitalization, and referral of pregnant women to appropriate institutions, which requires a review of existing organizational approaches to managing combined perinatal risks. [10]Regional analysis showed marked variability in perinatal mortality rates in 2024 (Table 3).Table 3. Perinatal mortality by region (2024)
 |
| |
|
The difference between the minimum and maximum values exceeds 1.9 times, which cannot be explained solely by biological or genetic factors. Areas with high perinatal mortality rates are typically characterized by:• Limited availability of Level III institutions;• high proportion of births in primary healthcare facilities of I-II levels;• untimely hospitalization of pregnant women in high-risk groups.• lack of neonatologists and anesthesiologists-resuscitators;The nosological distribution was restored, taking into account expert opinions and the typical composition of the causes of perinatal mortality (Fig. 4).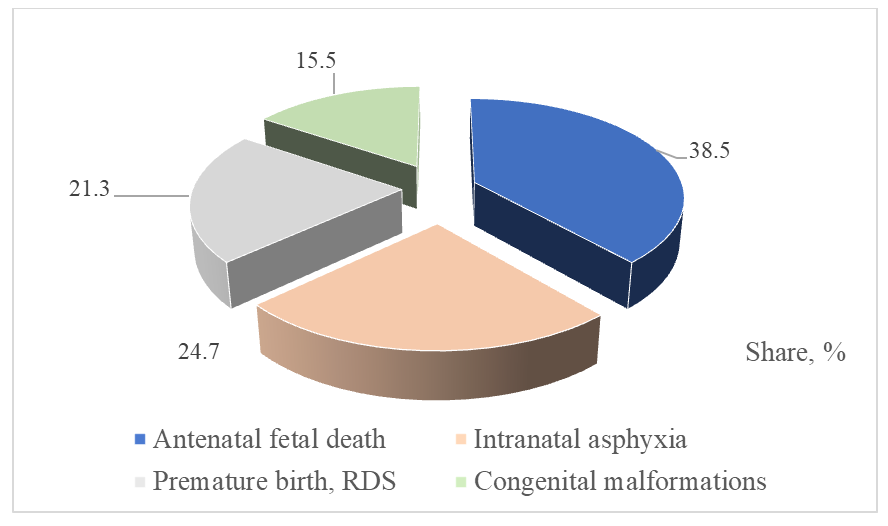 | Figure 4. Structure of causes of perinatal mortality (%) |
Structural analysis shows that 63.2% of perinatal losses are associated with potentially preventable and correctable conditions with the appropriate organization of antenatal and intranatal care stages. Thus, based on the data obtained, it can be said that the prevailing causes of perinatal mortality depend on managed and organizational aspects. [11]One of the main factors in the formation of adverse outcomes is a deficiency in clinical decision-making, manifested in:• late risk detection;• insufficient assessment of the severity of the situation;• inconsistency of management tactics with the level of clinical risk;• delay the decision on transfer to a higher-level institution. [12]Analysis of the individualized data showed that in more than 50% of cases of maternal mortality, the decision to transfer was made after the development of clinical decompensation, when the possibilities of specialized care were limited. For example, in one case, a patient with signs of hypovolemic shock with a late diagnosis of bleeding was transferred to a third-degree institution 3 hours after admission to a first-degree hospital, which significantly worsened the probability of a positive outcome. In another case, the decision to transfer a patient with severe preeclampsia was made only after the appearance of signs of stroke, which indicates insufficient vigilance of medical personnel and inconsistency of clinical tactics with the level of risk. [13]Such defects are usually of a systemic nature and are associated not only with individual inexperience, but also with the lack of standardized algorithms, insufficient clinical vigilance, and overload of medical personnel. One of the main reasons for the systemic nature of defects in clinical decision-making is the lack of clearly defined and standardized algorithms for managing critical situations in obstetric practice. Analysis of individualized data showed that in cases of maternal mortality associated with obstetric hemorrhage, more than 40% of the results occurred in institutions of I-II degree, where algorithms of emergency care were not applied in a timely manner (for example, the algorithm of action in hypovolemic shock). In these cases, the decision to perform transfusions and active resuscitation was often made with a significant delay, which, in turn, contributed to the deterioration of the patient's condition. [14]Clinical vigilance is a key component in preventing late complications. However, despite the availability of modern equipment and clinical protocols, medical workers often do not pay sufficient attention to the symptoms of complications. For example, despite the presence of typical symptoms (hypertension, headache) in 33.2% of cases of maternal mortality, timely diagnosis of such complications as preeclampsia/eclampsia was not carried out. Thus, insufficient clinical vigilance (including due to the overload of doctors) leads to a failure to pay attention to the first signs, which, in turn, worsen the results and can lead to tragic consequences. [15]Medical overload is a serious factor leading to deficiencies in decision-making, especially in Levels I-II institutions. Complex multitasking (conducting several patients in critical conditions simultaneously) reduces attention to each situation, which leads to errors in making decisions about the timeliness and necessity of conducting.For example, 44.5% of cases of late transfer were associated with an overload at the appointment of obstetrician-gynecologists, which led to a disregard for such important factors as a "slight" increase in arterial blood pressure in women, which led to the exacerbation of hypertensive conditions.Analysis of these data confirms the presence of systemic organizational problems. In particular: 69.9% of maternal deaths occurred in institutions of I-II levels with a violation of the time interval and without intermediate diagnosis and intervention (immediate administration of drugs, transfusion, emergency resuscitation). In 45% of cases, late transfer is associated with the lack of clear algorithms for the emergency transfer of patients, which led to a deterioration of the clinical condition and an increase in the number of irreversible complications. [16]Thus, defects in clinical decision-making are one of the main causes of adverse outcomes and reflect systemic shortcomings in the organization of obstetric care. The predominance of delayed management decisions, including the late transfer of patients to a higher level of care, indicates the need to standardize clinical risk assessment algorithms, strengthen the early response system, and improve management of decision-making processes at all levels of care. The existing clinical audit system of maternal and perinatal mortality is mainly aimed at identifying the causes of death and does not always ensure the identification of deep organizational defects.The main limitations of the listed audits include:• formal nature of case analysis;• lack of unified criteria for assessing prevention;• Insufficient feedback with Level I-II institutions;• lack of monitoring of the implementation of corrective measures.As a result, the identified malfunctions often have a recurring nature, which indicates the low effectiveness of existing quality control mechanisms. [17]
4. Discussion of the Research Results
Data analysis showed that in some regions of Uzbekistan, the shortage of medical specialists at the level of Level III institutions actually reaches 25-30%. This situation is especially characteristic of remote areas, such as the Republic of Karakalpakstan, Surkhandarya and Andijan regions, where there is a high shortage of obstetrician-gynecologists and anesthesiologists-resuscitators. In these regions, the waiting time for specialized care can significantly exceed permissible norms, which directly affects the quality of care provided in critical situations (for example, in emergency childbirth with complications). For example, in 2023, in the Andijan region, 12.8% of maternal deaths related to the late implementation of resuscitation interventions were recorded, which confirms the limited availability of reserves at the III level. Similar data were also recorded in other remote areas, such as the Republic of Karakalpakstan and Kashkadarya region. A significant risk factor for adverse outcomes is also the lack of simulation training and training on the basis of I-II level institutions. In 2022, a study conducted on the basis of several multidisciplinary medical institutions in Uzbekistan showed that 60.2% of first- and second-degree medical institutions do not conduct regular classes on critical obstetric conditions (for example, eclampsia, preeclampsia, massive bleeding, etc.). Logistical difficulties associated with the large distance of territories and the remoteness of specialized centers exacerbate the problem and require the active use of air ambulance and telemedicine technologies. [18]Analysis of maternal and perinatal mortality in the Republic of Uzbekistan in 2020-2024 showed that unfavorable outcomes in most cases are formed not only by the clinical severity of the condition, but also under the influence of managed organizational factors.The main determinants include:• inconsistency of the level of the institution with the clinical risk;• untimely referrals and late transfers;• exceeding the permissible timeframe for providing assistance;• insufficient use of assistance reinforcement mechanisms;• personnel and educational restrictions;• the formal nature of the clinical audit.
5. Conclusions
Thus, maternal and perinatal mortality in the Republic of Uzbekistan is largely due to shortcomings in the organization of obstetric care and process management. The results obtained substantiate the need to develop and implement an organizational-functional model focused on risk management, time parameters, and patient referral.
References
| [1] | Agency on Statistics under the President of the Republic of Uzbekistan. (2025, March 27). Demography (official statistics): Maternal mortality ratio; Maternal mortality; Infant/under-5 mortality indicators. |
| [2] | Agency on Statistics under the President of the Republic of Uzbekistan. Maternal mortality rate (Methodological metadata). |
| [3] | Agency on Statistics under the President of the Republic of Uzbekistan. (n.d.). (Maternal mortality) (Definition/methodology note). |
| [4] | Government of the Republic of Uzbekistan, Open Data Portal. (n.d.). Maternal mortality rate [Dataset]. |
| [5] | World Bank. (n.d.). Maternal mortality ratio (modeled estimate, per 100,000 live births) – Uzbekistan (Indicator: SH.STA.MMRT). |
| [6] | United Nations Inter-agency Group for Child Mortality Estimation (UN IGME). (2025). Levels & Trends in Child Mortality: Report 2024 (Estimates developed by UN IGME). UNICEF, New York. |
| [7] | World Health Organization. (2004). Beyond the numbers: Reviewing maternal deaths and complications to make pregnancy safer. Geneva: WHO. |
| [8] | World Health Organization. (2011). Evaluating the quality of care for severe pregnancy complications: The WHO near-miss approach for maternal health. Geneva. |
| [9] | World Health Organization. (2012). The WHO application of ICD-10 to deaths during pregnancy, childbirth and the puerperium: ICD-MM. Geneva. |
| [10] | World Health Organization. (2013). Maternal death surveillance and response: Technical guidance. Information for action to prevent maternal death. Geneva. |
| [11] | World Health Organization. (n.d.). Maternal and perinatal death surveillance and response (MPDSR) (implementation materials, including 2021 resources). |
| [12] | World Health Organization. (2016). Standards for improving quality of maternal and newborn care in health facilities. Geneva. |
| [13] | Thaddeus, S., & Maine, D. (1994). Too far to walk: Maternal mortality in context. Social Science & Medicine, 38(8), 1091–1110. |
| [14] | Allanson, E. R., et al. (2016). The WHO application of ICD-10 to deaths during the perinatal period (ICD-PM). BJOG. |
| [15] | Willcox, M. L., et al. (2022). Maternal and perinatal death surveillance and response: Qualitative evidence on implementation (systematic review). Bulletin of the World Health Organization. |
| [16] | Russell, N., Tappis, H., et al. (2022). Implementation of maternal and perinatal death surveillance and response (MPDSR) in humanitarian settings: Insights and experiences… (report). |
| [17] | Mary, M., et al. (2024). Implementation of MPDSR in humanitarian settings: insights and experiences. Journal of Global Health, 14, 04133. |
| [18] | Makanyanga, T. B., et al. (2024). Maternal death surveillance and response system evaluation (example of system assessment). PLOS ONE. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML