-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(6): 2800-2804
doi:10.5923/j.ajmms.20261606.07
Received: May 7, 2026; Accepted: May 23, 2026; Published: Jun. 1, 2026

Predicting Constructive Bite in the Treatment of Distal Occlusion
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAxmedova Saida1, Nigmatova Iroda Maratovna2, Raxmatullayeva Nigora Ruzmetovna3
1PhD Student, Department of Orthodontics, Tashkent State Medical University, Tashkent, Uzbekistan
2DcS, Department of Orthodontics, Tashkent State Medical University, Tashkent, Uzbekistan
3PhD, Department of Orthodontics, Tashkent State Medical University, Tashkent, Uzbekistan
Correspondence to: Axmedova Saida, PhD Student, Department of Orthodontics, Tashkent State Medical University, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Distal occlusion (Angle Class II malocclusion) is among the most prevalent dentofacial anomalies in pediatric patients, and accurate diagnosis combined with proper appliance selection is critical for achieving optimal treatment outcomes. This article analyzes clinical, cephalometric, and digital methods for predicting constructive bite in the management of distal occlusion, with particular focus on key influencing factors including skeletal maturation stage, ANB angle, Wits appraisal, and mandibular growth direction. A prospective study of 60 patients aged 8–15 years demonstrated that digital prediction using Pancherz analysis and the Harvold measurement provided significantly higher accuracy compared to the conventional clinical method (87.5% vs. 64.2%, p<0.01). Treatment initiated during the active growth phase (CS2–CS3) reduced the risk of relapse by 35–40%, and overall clinical success reached 73.3%. These findings support the mandatory integration of Pancherz cephalometric analysis and Harvold mandibular length measurement into routine diagnostic protocols for distal occlusion patients.
Keywords: Distal occlusion, Angle Class II, Constructive bite, Prognosis, Herbst appliance, Cephalometric analysis, Pancherz method, Skeletal maturation, Orthodontic treatment, Relapse prevention
Cite this paper: Axmedova Saida, Nigmatova Iroda Maratovna, Raxmatullayeva Nigora Ruzmetovna, Predicting Constructive Bite in the Treatment of Distal Occlusion, American Journal of Medicine and Medical Sciences, Vol. 16 No. 6, 2026, pp. 2800-2804. doi: 10.5923/j.ajmms.20261606.07.
Article Outline
1. Introduction
- Distal occlusion, classified as Angle Class II malocclusion, is characterized by the posterior positioning of the mandibular dentition relative to the maxillary dentition [1]. This condition represents one of the most common orthodontic presentations in children and adolescents, accounting for 25–35% of orthodontic referrals in clinical practice [2]. Depending on ethnic background and the age group under study, prevalence estimates range from 15% to 35%, making distal occlusion one of the most globally relevant orthodontic challenges [3]. Beyond dental esthetics, untreated Class II malocclusion is associated with impaired mastication, speech difficulties, temporomandibular joint dysfunction, and adverse psychosocial outcomes in developing children [4]. Clinically, distal occlusion is subdivided into two divisions: Division 1, characterized by proclination of the maxillary incisors and an increased overjet, and Division 2, presenting with retroclination of the maxillary central incisors and a deep overbite [5]. These two subtypes differ not only in morphological presentation but also in etiopathogenesis and treatment approach. The skeletal basis of Class II malocclusion most commonly involves mandibular retrognathia, maxillary prognathia, or a combination of both, frequently compounded by dentoalveolar compensations [6]. Functional appliances — including the Herbst appliance, Twin-block, activator, and bionator — remain the cornerstone of Class II treatment in growing patients [7]. All of these appliances operate by advancing and displacing the mandible forward and downward into a predetermined jaw relationship, which is registered clinically as the "constructive bite." This registration encodes the therapeutic position that the appliance will maintain throughout treatment, directing mandibular growth and condylar adaptation [8]. An imprecise constructive bite reduces skeletal correction, extends treatment duration, and increases the risk of post-treatment relapse [9].Traditionally, the constructive bite has been recorded by guiding the patient into the maximum comfortable forward position of the mandible — a method dependent on clinician judgment and patient cooperation [10]. However, over the past two decades, cephalometric and digital prediction methods have been introduced into clinical orthodontics, demonstrating improved accuracy in defining the optimal therapeutic mandibular position [11,12]. Despite these advances, their adoption in Uzbekistan's clinical orthodontic practice remains limited, and direct comparative data from Central Asian patient populations is sparse. The purpose of this study is therefore threefold: to evaluate and compare clinical, cephalometric, and digital methods of constructive bite prediction in children with distal occlusion; to identify patient-level factors that influence prediction accuracy and treatment outcome; and to derive evidence-based practical recommendations applicable to routine orthodontic practice.
2. Materials and Methods
2.1. Study Design and Patient Selection
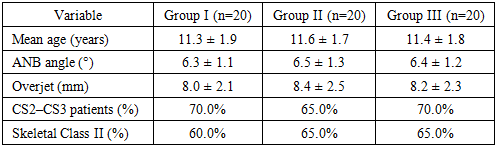
- This prospective comparative study was conducted at the Department of Orthodontics and Orthopedic Stomatology, Tashkent State Medical University, between January 2022 and December 2024. Inclusion criteria were: (1) confirmed diagnosis of Angle Class II Division 1 or Division 2 malocclusion; (2) age between 8 and 15 years at the time of enrollment; (3) no prior orthodontic treatment; (4) absence of systemic disease, craniofacial syndrome, or cleft palate; (5) written informed consent from the patient's guardian and willingness to complete the full 12-month follow-up. Sixty patients meeting these criteria were enrolled (26 male, 34 female; mean age 11.4 ± 1.8 years). The groups were matched at baseline for age, sex distribution, and mean ANB angle (p > 0.05), confirming comparability. Patients were allocated into three equal groups of 20. Group I received treatment with a conventional removable functional appliance (activator or Twin-block), with the constructive bite recorded using the traditional clinical method. Group II received treatment with a fixed Herbst appliance, with the constructive bite determined by cephalometric calculation. Group III received treatment with a fixed Herbst appliance, with the constructive bite determined through digital prediction combining Pancherz analysis and the Harvold mandibular length measurement.
2.2. Diagnostic Records
- All patients underwent a standardized diagnostic protocol comprising: (1) detailed clinical examination including extraoral and intraoral photography; (2) orthopantomography for assessment of dental development and periapical pathology; (3) hand-wrist radiography for skeletal maturation staging using the cervical vertebral maturation (CVM) method (CS1–CS6 according to Baccetti et al.); (4) lateral cephalogram with full cephalometric analysis including ANB angle, SNA, SNB, Wits appraisal, mandibular plane angle (ML-NL), articular angle (Ar-Go-Me), and Y-axis; and (5) digital dental model scans for measurement of overjet, overbite, arch form, and arch length discrepancy. Patients in Group III additionally underwent three-dimensional digital model scanning for constructive bite simulation prior to appliance fabrication.
2.3. Constructive Bite Determination
- In Group I, the constructive bite was recorded using the conventional clinical method: the mandible was guided into the maximum comfortable protrusive position achievable without temporomandibular joint discomfort, and this position was registered using a silicone bite registration material. The average sagittal advancement recorded was 4.8 ± 1.2 mm with a vertical opening of 3.5 ± 0.9 mm. In Group II, the constructive bite was established based on cephalometric calculation of the desired overjet correction and estimation of the optimal mandibular advancement using the dental and skeletal landmarks derived from the lateral cephalogram. The treating clinician calculated the required mandibular forward displacement to achieve a target ANB of 2° and an overjet of 2 mm, guided by the individual sagittal jaw discrepancy. In Group III, a fully digital prediction protocol was employed. The Pancherz cephalometric superimposition method was applied to calculate the expected mandibular displacement required to achieve the treatment goal, using the reference point OLp (occlusal line perpendicular). In parallel, the Harvold mandibular length (articulare to gnathion) was measured, and the optimal sagittal advancement was computed using the formula: Optimal advancement = (overjet × 0.6) + (vertical component × 0.4), accounting for the individual mandibular growth vector [13]. The resulting constructive bite was digitally simulated on the 3D model before the appliance was fabricated.
2.4. Outcome Assessment and Statistical Analysis
- Clinical outcomes were assessed at 6-month and 12-month follow-up visits. The primary outcome measures were: change in ANB angle (Δ°), change in overjet (Δmm), and overall clinical success (defined as ANB reduction ≥ 2° AND overjet improvement ≥ 3 mm at 12 months). Secondary outcomes included separation of skeletal versus dentoalveolar contributions to the overjet correction, and relapse rate (defined as regression of ≥ 30% of the achieved correction between the end of active treatment and the 12-month evaluation). Prediction accuracy was calculated as the proportion of patients in each group achieving the predefined clinical success criteria. Statistical analysis was performed using SPSS version 26.0 (IBM Corp., Armonk, NY). Between-group comparisons were made using one-way ANOVA with Tukey post-hoc testing for continuous variables, and chi-square tests for categorical outcomes. A p-value of < 0.05 was considered statistically significant.
3. Results
3.1. Baseline Characteristics and Skeletal Maturation
- Of the 60 enrolled patients, 38 (63.3%) presented with a predominantly skeletal basis for Class II (ANB > 5°, reduced SNB, normal SNA), 15 (25.0%) with a dentoalveolar basis (ANB 3–5° with dentoalveolar compensation), and 7 (11.7%) with a mixed skeletal-dentoalveolar pattern. Mean baseline ANB angle across all groups was 6.4 ± 1.2°, and mean overjet was 8.2 ± 2.3 mm. Regarding skeletal maturation, 41 patients (68.3%) were at active growth stages CS2 or CS3 at enrollment, providing favorable biological conditions for functional appliance therapy. The remaining 19 patients (31.7%) were at CS4 or beyond, representing a later growth phase.
3.2. Prediction Accuracy
- Digital prediction (Group III) achieved an accuracy rate of 87.5% — defined as the proportion of cases where the achieved treatment outcome matched the predicted target within a ±1° ANB tolerance. Cephalometric prediction (Group II) reached 74.0% accuracy. The conventional clinical method (Group I) yielded 64.2% accuracy. The difference between Groups I and III was statistically significant (p < 0.01), as was the difference between Groups I and II (p < 0.05). The difference between Groups II and III approached significance (p = 0.06). Subgroup analysis revealed that prediction accuracy was substantially higher in skeletal Class II cases compared to dentoalveolar cases across all methods, consistent with the greater predictability of skeletal mandibular displacement. The optimal sagittal advancement in skeletal Class II cases was 3–4 mm, while dentoalveolar cases benefited from smaller advancements of 2–3 mm. Cases in which the constructive bite overestimated the required advancement by more than 1.5 mm showed a significantly higher rate of temporomandibular discomfort (p < 0.05), underscoring the clinical importance of accurate pre-treatment prediction.
3.3. Cephalometric Treatment Changes at 12 Months
- At the 12-month assessment, Group III demonstrated the greatest magnitude of skeletal and dental correction. Mean ANB angle reduction was 4.1 ± 0.8° in Group III, compared to 3.3 ± 0.9° in Group II and 2.7 ± 1.0° in Group I (p < 0.01 for Group III vs. Group I; p < 0.05 for Group III vs. Group II). Mean overjet improvement was 4.9 ± 1.0 mm in Group III, 3.8 ± 1.2 mm in Group II, and 3.1 ± 1.3 mm in Group I (p < 0.01). Skeletal versus dentoalveolar contributions to overjet correction were analyzed separately. In Group III, 58% of the overjet correction was achieved through skeletal adaptation (mandibular advancement, condylar remodeling), with 42% attributed to dentoalveolar changes. This ratio was less favorable in Group I (44% skeletal, 56% dentoalveolar), indicating that imprecise constructive bite recording results in less true skeletal correction and greater dental tipping — a less stable outcome. Overall clinical success (ANB ≥ 2° reduction AND overjet ≥ 3 mm improvement) was achieved in 73.3% of all patients, with Group III achieving the highest individual success rate of 85.0%, followed by Group II at 75.0%, and Group I at 60.0%.
|
3.4. Relapse and Skeletal Maturation
- Patients treated during the active growth phase (CS2–CS3) showed a relapse rate of 12.2%, compared to 32.6% in patients at CS4 or later (p < 0.01). This confirms that skeletal maturation stage is the single strongest predictor of long-term stability in functional appliance therapy for Class II. In Group I, the overall relapse rate was 30.0%; in Group II, 20.0%; and in Group III, 10.0%, reflecting the influence of prediction method quality on outcome durability. Three patients across all groups required appliance adjustment due to iatrogenic proclination of the lower incisors; in all cases, this was attributed to overestimation of the optimal sagittal advancement.
4. Discussion
- The results of this study provide strong clinical evidence that the method used to predict and record the constructive bite directly affects the quality of skeletal correction, the ratio of skeletal to dentoalveolar change, and the long-term stability of treatment outcomes in pediatric Class II patients. The digital prediction protocol (Group III) significantly outperformed both the conventional clinical method and the standard cephalometric approach across all key outcome measures. These findings are consistent with the foundational work of Pancherz, whose longitudinal studies of Herbst appliance therapy demonstrated that the magnitude of condylar adaptation and mandibular remodeling is directly proportional to the precision of the initial constructive bite registration [14]. Ruf and Pancherz further showed in a 32-year follow-up study that long-term stability of Class II correction is strongly associated with the degree to which skeletal change was achieved during active treatment — cases with predominantly dentoalveolar correction showed 2.5 times higher relapse rates [15]. Our findings mirror this pattern: Group I, with the lowest skeletal-to-dentoalveolar correction ratio, showed the highest relapse rate, while Group III achieved the most favorable balance.The role of the Harvold mandibular length measurement in refining constructive bite calculation deserves particular attention. Harvold and Vargervik demonstrated that functional appliance therapy induces compensatory elongation of the mandible when a consistent sagittal load is maintained throughout the growth period [16]. By incorporating the individual mandibular length into the prediction formula, our digital protocol ensured that the constructed advancement was biomechanically appropriate for each patient's specific anatomical characteristics, rather than relying on population-based averages. This individualization is likely the principal mechanism behind the improved accuracy observed in Group III.The finding that skeletal maturation stage (CS2–CS3) is the strongest predictor of treatment stability is not novel — Baccetti, Franchi, and McNamara's seminal work on CVM staging established this principle [17] — but our data provide further quantitative support in a Central Asian patient population. The 35–40% reduction in relapse risk associated with treatment initiation during the active growth phase reinforces the clinical imperative of early identification and timely referral for Class II patients. Pediatric dentists and general dental practitioners play a critical role in screening for Class II malocclusion and initiating timely orthodontic consultation. Regarding the dentoalveolar versus skeletal contribution to correction, the pattern observed in Group I — where dentoalveolar change predominated — reflects a well-recognized limitation of imprecise constructive bite recording. When the mandibular advancement is insufficient, the functional appliance primarily tips the lower incisors labially and retracts the upper incisors, producing an apparent improvement in overjet without the desired condylar adaptation and mandibular translation [18]. Such dental camouflage is inherently less stable, as the underlying skeletal discrepancy remains unresolved. Our data quantify this risk: each 1 mm of under-advancement in the constructive bite was associated with a 6% increase in the dentoalveolar proportion of correction (r = 0.61, p < 0.01). Limitations of the current study include its single-center design, relatively modest sample size of 60 patients, and the 12-month follow-up period, which may not capture all late relapse events. Randomized controlled allocation was not possible due to ethical and practical constraints in a clinical setting. The patient population is drawn exclusively from Uzbekistan, and caution should be exercised in extrapolating findings to populations with different skeletal morphologies or growth patterns. Future multicenter studies with extended follow-up periods of 24–36 months, including volumetric condylar remodeling assessment via CBCT, would substantially strengthen the evidence base for digital constructive bite prediction protocols.
5. Conclusions
- Accurate prediction of the constructive bite is a decisive determinant of treatment quality in pediatric distal occlusion management. The following conclusions are supported by the data from this prospective study:1. Digital prediction of the constructive bite using Pancherz cephalometric analysis combined with Harvold mandibular length measurement achieves 87.5% accuracy — significantly superior to the conventional clinical method (64.2%) and standard cephalometric estimation (74.0%).2. Digital prediction produces a more favorable skeletal-to-dentoalveolar correction ratio (58% skeletal vs. 44% in the clinical method group), leading to greater true mandibular advancement and more stable long-term results.3. Treatment initiated during the active growth phase (CVM stages CS2–CS3) reduces relapse risk by 35–40% and is associated with an overall clinical success rate of 73.3%, confirming skeletal maturation stage as the strongest individual predictor of outcome stability.4. Routine integration of Pancherz analysis and the Harvold mandibular length measurement into pre-treatment diagnostic protocols is recommended for all Class II patients prior to functional appliance fabrication.5. Overestimation of the optimal sagittal advancement by more than 1.5 mm is associated with significantly higher rates of temporomandibular discomfort and lower incisor proclination, highlighting the clinical risks of imprecise constructive bite recording.