-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(6): 2783-2791
doi:10.5923/j.ajmms.20261606.04
Received: May 1, 2026; Accepted: May 26, 2026; Published: Jun. 1, 2026

Mechanisms, Diagnosis, and Management of Progressive Multifocal Leukoencephalopathy
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLSamiev A. S.1, Bobomurodov G. A.2, Khushvaktov N. Z.2, Samiyev B. A.2
1Samarkand State Medical University, Samarkand, Uzbekistan
2Samarkand Branch of the Republican Scientific and Practical Medical Center of Emergency Care, Samarkand, Uzbekistan
Correspondence to: Samiev A. S., Samarkand State Medical University, Samarkand, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Progressive multifocal leukoencephalopathy (PML) is a rare and potentially fatal demyelinating disease caused by the reactivation of the JC virus (JCV), primarily affecting immunocompromised individuals. This study aims to evaluate the current treatment approaches for PML, focusing on immune reconstitution therapies, antiviral strategies, and emerging therapies such as pembrolizumab. A comprehensive review was conducted from 2022 to 2025, incorporating data from clinical trials, case reports, and therapeutic outcomes in immunosuppressed patients, including those with HIV, multiple sclerosis, and autoimmune disorders. Immune reconstitution remains the cornerstone of PML management, particularly in HIV-infected individuals who respond well to antiretroviral therapy. The cessation of immunosuppressive drugs, such as natalizumab and fingolimod, is also crucial for reversing immune suppression. Antiviral therapies, including cidofovir and foscarnet, have shown limited effectiveness, with the need for more potent agents. Pembrolizumab, an immune checkpoint inhibitor, has emerged as a promising treatment by enhancing T-cell responses and controlling JCV replication. Furthermore, biomarkers such as neurofilament light chain and JC virus-specific T-cell responses are increasingly being recognized for their potential in early diagnosis and monitoring of disease progression. The findings highlight the need for a multidisciplinary approach, integrating immune reconstitution, antiviral therapy, and novel immune-modulating agents to improve outcomes for PML patients. Ongoing research into new biomarkers and therapies is essential to optimizing treatment strategies and enhancing patient survival rates.
Keywords: Progressive multifocal leukoencephalopathy, JC virus, Immune reconstitution, Pembrolizumab, Biomarkers, Antiviral therapy
Cite this paper: Samiev A. S., Bobomurodov G. A., Khushvaktov N. Z., Samiyev B. A., Mechanisms, Diagnosis, and Management of Progressive Multifocal Leukoencephalopathy, American Journal of Medicine and Medical Sciences, Vol. 16 No. 6, 2026, pp. 2783-2791. doi: 10.5923/j.ajmms.20261606.04.
Article Outline
1. Introduction
- Progressive multifocal leukoencephalopathy (PML) is a rare, often fatal, demyelinating disease that results from the reactivation of the JC virus (JCV) in patients with a compromised immune system. The disease mainly targets the central nervous system (CNS), with progressive demyelination in the white matter of the brain and spinal cord, resulting in neurological impairment. PML has gained significant attention in the field of neurology over the past few decades, especially in the era of increasing immunosuppression, such as in patients with multiple sclerosis (MS), autoimmune diseases, and cancer. PML is a significant disease in the differential diagnosis of central nervous system symptoms in patients taking immunosuppressive medications, requiring prompt recognition and treatment to enhance patient outcomes [2,4,11-12].The link between PML and immunosuppression has been established. For example, treatment with natalizumab, a monoclonal antibody for the treatment of MS, has been associated with an increased risk of PML, with many cases reported [6]. This association with therapy is of particular concern as it demonstrates the trade-off between the effectiveness of treatment and the risk of side effects. In addition, PML is also of interest in the HIV/AIDS population, where it continues to be a major complication of severe immunodeficiency [8,9]. So-called HIV-associated PML occurs as a result of the profound T-cell deficit seen in HIV infection and AIDS.In addition to infections, PML has been reported in patients treated with biologic agents, such as rituximab and fingolimod, that are used for the treatment of autoimmune diseases. While these drugs are effective at treating disease, they can increase the risk of PML by altering immune responses and the capacity to control JCV infection [2,9]. Therefore, the clinical relevance of PML spans infectious and therapeutic approaches, highlighting the importance of vigilant monitoring in high-risk populations.Due to its severe consequences and potential for misdiagnosis, it is essential for neurologists and other clinicians who treat immunosuppressed patients to be aware of the aetiology, clinical features, and management of PML. The increasing use of new therapies and immune-modulating agents is likely to result in increased rates of PML, so ongoing work in understanding the mechanisms, diagnosis, and treatment of PML is needed [4,7].
2. Methods
- A structured literature search was conducted in PubMed/MEDLINE, Scopus, Web of Science, and Google Scholar to identify studies relevant to progressive multifocal leukoencephalopathy (PML), John Cunningham virus (JCV), immunosuppression, diagnosis, and treatment. The search covered publications from 2000 to 2026, with priority given to recent reviews, clinical guidelines, cohort studies, case series, and mechanistic studies directly related to PML. Search terms included: “progressive multifocal leukoencephalopathy,” “PML,” “JC virus,” “JCV reactivation,” “PML treatment,” “immune reconstitution,” “PML-IRIS,” “natalizumab-associated PML,” “HIV-associated PML,” “pembrolizumab,” “maraviroc,” and “mirtazapine.” Studies were included if they addressed PML pathogenesis, clinical presentation, diagnostic approaches, therapeutic interventions, or outcomes. Publications not directly related to PML, JCV biology, or clinically relevant immunosuppression were excluded to maintain the scientific focus of the review.
3. Pathophysiology
- PML is caused by the reactivation of the JCV, a common human polyomavirus that is usually latent in the kidneys and other tissues of healthy individuals. But in individuals with immune deficiencies, especially those receiving immunosuppressant treatments, the virus can be reactivated and lead to extensive demyelination in the CNS [1,2,13,16]. JCV infects oligodendrocytes, which are the cells that form myelin in the CNS, resulting in demyelination of the CNS and the clinical presentation of PML.JCV gains entry to the CNS by breaching the blood-brain barrier. JCV then infects oligodendrocytes and starts replicating. Viral replication interferes with the cell's normal functions and ultimately results in cell death. This not only affects oligodendrocytes, but other glial cells as well and leads to inflammation. The viral infection also causes a focal and often unilateral demyelination, commonly observed in the subcortical white matter of the brain [1,6,17,19].Immunosuppression plays a crucial role in PML's development. The JCV virus is normally latent, due to efficient immune surveillance, including the presence of CD8+ T cells that block its reactivation. But immunosuppression, which can be caused by biologic therapies (e.g., natalizumab, rituximab) and immunosuppressive medications (e.g., methotrexate, fingolimod), impair the immune system's capacity to modulate latent viral infections. For instance, natalizumab, an antibody used to treat multiple sclerosis, blocks the trafficking of immune cells to the CNS and results in the reactivation of JCV in the brain [6,7]. Likewise, fingolimod, which is used to treat MS by blocking sphingosine-1-phosphate receptors, prevents the recirculation of the immune cells and the immunosurveillance that would usually block JCV replication in the CNS [9,10,22].Immune suppression is not the only factor that may increase the risk of PML; genetic factors may also play a role. Studies have demonstrated that certain variants in the gene that codes for the vitamin D receptor (VDR) increase the risk of JCV reactivation in the brain, especially in immunodeficient patients [5]. In addition, in HIV patients, the loss of CD4+ T cells plays a direct role in the loss of control over JCV infection, leading to the spread of the virus within the CNS [2,8,23].Inflammation is a complex aspect of PML. Although JCV infection causes direct virus-induced damage to oligodendrocytes, the inflammation in the CNS can contribute to the damage. But research has shown that the inflammation in PML is not as marked as in other demyelinating conditions, such as multiple sclerosis. Rather, the inability of the immune system to effectively respond to the virus caused by immunosuppression leads to the spread of the virus [7,8,25].Further, the relationship between the immune system and viral replication implies that although immunosuppression is a key risk factor, it is not the only factor involved in the development of PML. Other variables, including individual immune status, duration and degree of immunosuppression, and the type of immune-modulating agents used, all contribute to PML risk. For example, the duration of immunosuppressive treatment or the use of multiple immunosuppressive agents may increase the risk of PML in a more than additive fashion [6,9,10].Overall, the development of PML is complex, with the reactivation of JCV in the CNS as a result of inadequate immune surveillance, especially during immunosuppressive treatment, playing a key role. The replication and cytopathic effect of the virus on oligodendrocytes leads to demyelination, and other variables including genetic susceptibility and the type of immunosuppression also contribute to the development and severity of PML. These processes are essential for recognizing susceptible populations and approaches to prevent or treat PML [6,9,10].
4. Risk Factors
- Risk of developing PML is driven by a complex interaction of immunosuppressive medications, genetics, and immunocompromising conditions. The primary risk factor for developing PML is the administration of immunosuppressive therapies, such as those commonly used for autoimmune conditions, multiple sclerosis (MS), and malignancy. While these therapies are effective at treating disease, they often result in a dysfunctional immune response, which can leave patients susceptible to infections, including JCV reactivation in the CNS [2,4,10].Biologic agents, disease-modifying antirheumatic drugs (DMARDs), and other immunosuppressive drugs that raise the risk of PML include immunosuppressive therapies. Natalizumab, a monoclonal antibody that blocks α4-integrin and blocks leukocyte trafficking across the CNS, is one of the most important risk factors for PML. Natalizumab is used to treat multiple sclerosis and Crohn's disease, but has been strongly linked to the development of PML, particularly in people who have been infected with the JC virus. Natalizumab suppresses the immune response, allowing the JC virus to reactivate and cause damage to the CNS [6,1,4].Likewise, another therapeutic immunosuppressant, fingolimod, has been associated with PML. Fingolimod works by trapping lymphocytes in lymph nodes, thereby decreasing their presence in the bloodstream and diminishing their ability to monitor the CNS. This modifies the immune milieu and promotes JCV reactivation. Research has demonstrated the occurrence of PML in fingolimod-treated MS patients, especially those with a history of prior immunosuppression [9,10]. Other immunosuppressive medications, including methotrexate and rituximab, have also been linked to increased PML risk; however, the mechanisms of action differ for each medication [7,2,26]. Rituximab, a monoclonal antibody that targets B cells, has been reported to induce PML in patients with autoimmune conditions and hematologic cancers, highlighting the role of immune cell targeting in PML development [27-30].Although most PML cases are associated with immunosuppression, genetic predispositions could also play a role in PML development. Certain genetic variants in immune-related genes, such as the vitamin D receptor (VDR) gene, have been associated with the risk of JCV reactivation. Research has demonstrated that some variants in the VDR gene may lead to changes in immune function, potentially compromising the ability to respond to viral infections such as JCV [5]. Furthermore, mutations in genes that regulate immune responses or the blood-brain barrier may also contribute to individual susceptibility to PML, although further research is required to better understand these genetic influences [11,12,31].Besides immunosuppressive treatment and genetic factors, the presence of coexisting conditions is a key factor in the development of PML. For example, the risk of PML is greatly elevated in patients with HIV/AIDS, as a result of the marked loss of CD4+ T cells, which are important in regulating latent viruses. PML is a common complication of advanced HIV infection and its prevalence has decreased considerably with the introduction of antiretroviral therapy, which improves immune response [8,9]. But JCV reactivation can be problematic in patients with HIV who have low CD4+ T cell counts [2,9,32].Other risk factors for PML include transplant recipients who must remain on long-term anti-rejection therapy. These patients, especially those with kidney, liver, and bone marrow transplants, are at a greater risk of developing PML due to the immunosuppressive agents needed to prevent graft rejection. Likewise, patients with cancers who receive immunosuppressive therapy, such as chemotherapy or monoclonal antibodies (e.g., rituximab), are at increased risk of developing PML as the treatment lowers the patients' immunity and makes it difficult to manage JCV infection [6,7].Age and sex are other factors that affect the risk of PML. PML is more prevalent in older individuals, which is probably due to the normal decrease in immune function with age. Elderly adults (aged 50 years or older) are more susceptible to PML following exposure to immunosuppressive agents, perhaps due to compromise of the immune system's ability to control latent infections as a result of normal aging [2]. Additionally, male gender has been recognized as a risk factor, with men being more susceptible to PML than women, particularly in the setting of MS and HIV infection [1,6,28].The major risk factors for PML include exposure to immunosuppressive drugs, especially natalizumab, fingolimod, and rituximab, which suppress immune responses, leading to JCV reactivation in the CNS. Genetic factors, such as polymorphisms in the vitamin D receptor gene, may also play a role in predisposing to PML. Moreover, other medical conditions such as HIV/AIDS, organ transplantation, and neoplasia, add to the risk of PML, particularly in patients treated with immunosuppressive drugs. In addition, other individual characteristics, including age and sex, play a role in the incidence of this debilitating infection, highlighting the need for a tailored approach in the management of patients at risk for PML [1,6,7,9,33].
5. Clinical Presentation and Diagnosis
- PML is a lethal demyelinating disease resulting from the reactivation of the JCV in immunodeficient patients. PML typically presents as a subacute, slowly progressive disease, with onset of symptoms ranging from weeks to months. Focal neurological signs and symptoms are the most common presenting symptoms of PML, including motor weakness, visual impairment, ataxia, cognitive impairment, and dysarthria. Initial symptoms can be mild and non-specific, such as mild weakness or mild cognitive changes, but as PML develops, patients often develop more severe and debilitating neurological symptoms. PML is characterised by the rapid onset and progression of these symptoms, with patients rapidly declining over weeks to months [1,7].PML can also result in psychiatric symptoms, such as depression, personality changes or confusion, which can initially make diagnosis challenging, particularly in immune-compromised individuals [3,5].PML diagnosis is clinical, but it is greatly assisted by neuroimaging and laboratory investigations. PML is best diagnosed using MRI, but it shows up as non-enhancing white matter lesions in the brain, especially in the subcortical areas (parietal, occipital, and frontal lobes). These lesions are usually poorly demarcated, giving them a "fuzzy" appearance, which can help to differentiate them from other types of demyelination, such as multiple sclerosis (MS). But the presence of these lesions does not necessarily confirm a diagnosis of PML and can be seen in other diseases, such as HIV encephalopathy or toxic leukoencephalopathy [8,4].Besides MRI, confirmation of PML diagnosis is achieved by the detection of JC virus DNA in the cerebrospinal fluid (CSF) through the use of polymerase chain reaction (PCR). JCV PCR is highly specific, and can detect the virus in the CNS, which is an important diagnostic criterion. But PCR is not always positive in the early phase of PML or in cases with low viral load, so a negative PCR test cannot exclude PML. A biopsy of the affected brain tissue may sometimes be needed to confirm PML, but it is rarely used because of the availability of non-invasive tests, such as PCR [6,9,33-36].Role of NeuroimagingPML is also diagnosed by neuroimaging, particularly magnetic resonance imaging (MRI). The characteristic imaging finding in PML is the presence of unenhanced (early in the disease course) and asymmetrically distributed white matter lesions. The lesions are usually found in the subcortical regions of the brain and commonly affect the occipital and parietal lobes, becoming progressively more extensive in the latter stages of the disease. Apart from conventional MRI, specialised imaging modalities, such as diffusion-weighted imaging (DWI) and fluid-attenuated inversion recovery (FLAIR), may help to further characterise the lesions. Although MRI is sensitive in the diagnosis of PML, it is not specific, and other demyelinating diseases also appear similar to PML on MRI. The MRI appearance of PML can be similar to that of other demyelinating diseases, such as multiple sclerosis (MS) or viral encephalitis, so it’s important to take into account the patient’s medical history and risk factors, along with the MRI findings [12,37-41].Brain imaging can also be used to track the progression of disease and determine the extent of involvement in the brain. Repeated MRI may be used to assess the degree of demyelination and to monitor changes in lesion size and/or location over time. This knowledge is essential for clinicians to gauge disease activity and make treatment decisions, especially in those patients who are being considered for immune reconstitution therapy or other forms of treatment. However, while helpful, neuroimaging cannot definitively rule out PML from other diseases that share its imaging pattern, therefore a patient's diagnosis should be made in conjunction with PCR and clinical diagnosis [13,35,44].Differential DiagnosisPML can be difficult to distinguish from a number of other diseases due to its clinical presentation, and therefore, a wide differential diagnosis should always be considered in a patient with suspected PML. The most common condition to be considered in the differential diagnosis of PML is multiple sclerosis (MS), an autoimmune disease with demyelination of the CNS. PML and MS both cause focal neurological symptoms including weakness, visual changes, and ataxia. But the lesions in MS are typically symmetrical, in the periventricular white matter, and contrast-enhance on MRI, which is not common in PML. Also, the MS lesions are often more white matter-periventricular and discrete, whereas the PML lesions are more diffuse and commonly include the cortical-subcortical junctions [14,31,41].HIV-associated encephalopathy is another possible diagnosis, which can present with cognitive impairment, motor weakness, and personality changes, just like PML. In HIV-positive patients, HIV-associated encephalopathy may be present, but the MRI changes in HIV-associated encephalopathy are usually diffuse cortical atrophy and non-specific white matter changes, as opposed to the focal, asymmetric lesions of PML. And CSF PCR testing for JC virus would be positive in PML but negative in HIV-associated encephalopathy, which may help to distinguish the two [2,10].Toxoplasmosis is another infectious disease that may be confused with PML, particularly in immunocompromised patients such as those with HIV/AIDS. Toxoplasmosis can cause focal neurological symptoms and can have a similar appearance to PML on MRI. But toxoplasmic lesions typically contrast-enhance on MRI and may have a ring-like appearance. Furthermore, CSF PCR for Toxoplasma gondii would be positive in toxoplasmosis, but negative in PML, another helpful diagnostic feature [15,42,43].Other differential diagnoses to consider include cerebral vasculitis, which can present with a range of neurological symptoms and MRI findings similar to PML, and viral encephalitides such as herpes simplex virus (HSV) encephalitis, which also cause focal neurological signs. But viral encephalitis may cause significant contrast enhancement on MRI, which is not usually seen in PML, which tends to be non-enhancing in its early stages [44-46].Although MRI and PCR for JC virus are the key elements in the diagnosis of PML, it's essential to be aware of the various differential diagnoses that may have similar clinical and radiological presentations. Timely diagnosis of PML is essential, especially as the disease can progress quickly and the management of PML patients with known or suspected immunosuppression requires specific considerations.
6. Treatment Approaches
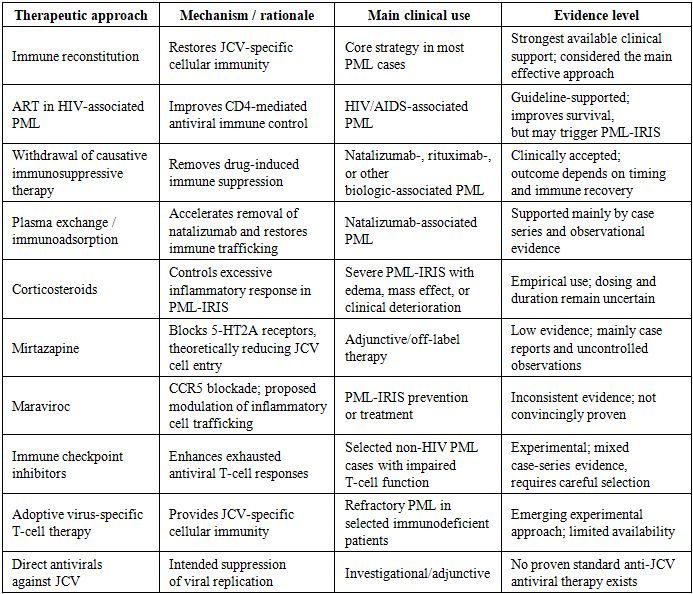
- PML is a challenging condition to manage, especially in immunocompromised individuals, where early treatment is essential to prevent irreversible brain damage. Treatment aims to re-establish the immune response and halt the spread of JCV. Since PML arises in the background of immune suppression, the most successful therapeutic strategies involve addressing the immune dysregulation and, if feasible, suppressing the virus. While there is no specific cure for PML, various approaches have been shown to be beneficial [14,23].Immune Reconstitution TherapyA primary therapeutic approach in the treatment of PML, especially in HIV-infected individuals or those receiving treatment for autoimmune diseases, is immune reconstitution. Immune reconstitution is important because PML results from a breakdown of immune surveillance, leading to reactivation of JCV and subsequent damage to the CNS. Antiretroviral therapy (ART) to reconstitute the immune system is the mainstay of treatment in HIV-infected patients. Successful ART results in an increase in the number of CD4+ T cells, essential for the suppression of JCV. There are numerous reports of successful treatment of PML in HIV patients through immune reconstitution with ART. In fact, starting ART has been shown to result in a reduction in JCV load and stability or even improvement in neurological symptoms, although this recovery can be slow and incomplete, depending on the damage that has been done by the time treatment is initiated [5,16].In non-HIV immunosuppressed patients, immune reconstitution aims to withdraw or change the immunosuppressive treatment associated with PML. For example, patients treated with natalizumab or fingolimod can benefit from ceasing these therapies in an attempt to restore immune function. For example, in patients with MS, withdrawal of natalizumab may result in some degree of immune reconstitution, but the outcome depends on the timing of natalizumab treatment and the extent of CNS damage [30,11]. Similarly, recovery of the immune response after withdrawal of rituximab treatment in patients with autoimmune disease may help reduce the effects of JCV reactivation. In some instances, immune reconstitution may also involve the administration of intravenous immunoglobulin (IVIG); however, this requires further study and is somewhat controversial [3,26,47-49].Antiviral TherapiesWhile immune reconstitution is the primary treatment for PML, direct antiviral therapy to treat JC virus is not currently considered a cure. JCV is a highly adapted virus, and its capacity to latent in immune-privileged areas such as the CNS makes the direct antiviral treatment difficult. But a number of antiviral approaches have been investigated, some of which have shown some promise for PML.Cidofovir, a potent DNA polymerase inhibitor, has been tested for the treatment of PML. Cidofovir has shown some effectiveness in decreasing JCV replication in vitro and animal models of PML. But the role of cidofovir in the treatment of PML in humans is unclear, with mixed results reported in case studies. It also has a risk of nephrotoxicity, which can be an issue for some patients [18,7]. Leflunomide is another potential antiviral drug being studied, which has demonstrated some efficacy against JCV in vitro and in animal models but its effectiveness in PML patients remains uncertain [21,6]. Leflunomide may be combined with immune reconstitution to try and manage the viral infection while the immune system is restored [2,13].
|
7. New Therapies and Biomarkers
- PML is a rare and devastating condition caused by the JC virus (JCV). The recent research on PML has involved improving immune reconstitution and new therapies to treat the virus itself. While there is no clear antiviral therapy, new therapies have been explored, especially with regard to immunosuppressive and immunotherapies [3,15].A recent very promising development in PML therapy is the use of pembrolizumab, an anti-PD-1 monoclonal antibody, which enhances immune responses by blocking the PD-1 pathway. PD-1 is an immune checkpoint protein that downregulates T-cell function, and blocking it can lead to improved T-cell responses to tumors and pathogens. Immune suppression plays a major role in the development of PML, as the immune system is unable to effectively control JCV. Pembrolizumab, through activation of T-cells, has been found to restore immune function and suppress JCV replication in early-phase clinical trials. While the evidence is still preliminary, pembrolizumab may be an effective treatment for PML, especially in patients who have failed other immune reconstitution therapies [7,9,19].A further emerging treatment strategy is the use of immune-modulating drugs such as lenalidomide, which has been shown to have efficacy in restoring immune function by enhancing T-cell responses and decreasing the viral burden. Recent studies have indicated that lenalidomide, when combined with immune reconstitution strategies, may have a positive impact on PML patients, especially those receiving immunosuppressive treatment such as rituximab or natalizumab. Although still under investigation, the role of lenalidomide as an adjunctive therapy to improve immune function is an exciting development in the treatment of PML patients [6,18].Alongside these immune-modulators, antiviral drugs like foscarnet and cidofovir are also being investigated for their capacity to block JCV replication. Although they have demonstrated limited effectiveness in PML, there are ongoing trials to determine their potential to reduce the viral load, especially when used in conjunction with immune reconstitution approaches. While these agents have demonstrated some effectiveness against JCV in laboratory settings, their utility in treating PML patients is still unclear and needs to be explored [10,14,5].There have also been considerable advances in the quest for biomarkers for early diagnosis and monitoring of PML. JCV DNA polymerase chain reaction (PCR) remains the diagnostic test of choice for detecting viral DNA in cerebrospinal fluid (CSF). But there is growing interest in identifying additional biomarkers that may predict the risk of developing PML or be used as early markers of disease. For example, serum neurofilament light chain (NfL) is a potential biomarker for assessing neuroaxonal damage in several neurological diseases, including PML. Increased CSF concentrations of NfL have been associated with disease severity and may be used to monitor disease progression or treatment response in PML patients [8,10,22].Other possible biomarkers include soluble CD14 and JCV-specific T-cell responses, which could offer clues to the immune response needed to prevent JCV reactivation. Assessing these biomarkers could potentially help clinicians detect the development of PML before symptoms manifest, enabling early treatment and potentially improved patient outcomes [7,21].
8. Conclusions
- PML continues to be a devastating and often fatal infections in immunocompromised patients, but new treatments and biomarker research provide a reason for optimism. Immune reconstitution strategies, such as antiretroviral drugs for HIV patients and the withdrawal of immunosuppressive drugs, such as natalizumab, remain the key approach to PML management, highlighting the need to rebuild the immune system. Furthermore, new therapies like pembrolizumab, lenalidomide and antiviral drugs may directly address the role of JC virus reactivation, and its viral load, but more research is needed to validate their use.The discovery of biomarkers for early detection and monitoring is another key advancement. Biomarkers like neurofilament light chain and JCV-specific T-cell responses could potentially lead to earlier diagnosis of PML, improved monitoring of disease progression, and more accurate assessment of treatment response. These developments may facilitate individualised treatment approaches and improve the overall outcome of PML patients.Overall, the mechanisms, diagnosis and treatment of PML are complex, especially in the immunocompromised setting. Continued research is needed to better understand the mechanisms of JCV reactivation, to discover new targets for treatment and to establish biomarkers for the early diagnosis and monitoring of the disease. Healthcare professionals should be alert to the early symptoms of PML, especially in susceptible groups, and collaborate with neurologists and infectious disease experts to provide optimal treatment strategies. As our understanding grows, it's important to continue to improve the management of PML and enhance the quality of life for affected patients with timely and appropriate interventions.