-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(6): 2773-2777
doi:10.5923/j.ajmms.20261606.02
Received: Apr. 21, 2026; Accepted: May 15, 2026; Published: Jun. 1, 2026

Nursing Practices in the Prevention and Management of Post-Vaccination Adverse Effects
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLElmira A. Shamansurova1, Mokhira A. Mannapova2
1DSc, Professor, Head of the Department of Physical Education and Civil Protection, Family Medicine No. 1, Tashkent State Medical University, Tashkent, Uzbekistan
2PhD Student, Basic Doctoral Student (PhD), Department of Physical Education and Civil Protection, Family Medicine No. 1, Tashkent State Medical University, Tashkent, Uzbekistan
Correspondence to: Mokhira A. Mannapova, PhD Student, Basic Doctoral Student (PhD), Department of Physical Education and Civil Protection, Family Medicine No. 1, Tashkent State Medical University, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Vaccination is one of the most effective measures for preventing infectious diseases, although mild reactions may occur after immunization and may influence parental confidence. This study was conducted to assess the occurrence of post-vaccination reactions in children and to evaluate the role of nursing practice in their prevention and management in outpatient settings. A descriptive cross-sectional study was performed in two outpatient polyclinics located in rural (25-OP) and urban (7-OP) areas, involving a total of 100 parents (50 per clinic) selected through convenience sampling. Data were collected through parental questionnaires and review of medical documentation. Statistical analysis included descriptive methods and chi-square testing for group comparison. The results showed that the most common reactions were fever, temporary irritability, and local symptoms such as pain and redness at the injection site. Allergic reactions were observed rarely, and no severe complications were recorded. All reactions were mild and resolved without medical intervention. No statistically significant differences were identified between rural and urban clinics (p>0.05). Proper nursing practice, including pre-vaccination assessment, adherence to immunization procedures, post-vaccination monitoring, and parental counseling, plays an important role in reducing adverse reactions and ensuring vaccination safety. These findings support the overall safety of routine immunization and emphasize the importance of professional nursing support.
Keywords: Vaccination, Adverse events following immunization, Nursing practice, Vaccine safety, Preventive care
Cite this paper: Elmira A. Shamansurova, Mokhira A. Mannapova, Nursing Practices in the Prevention and Management of Post-Vaccination Adverse Effects, American Journal of Medicine and Medical Sciences, Vol. 16 No. 6, 2026, pp. 2773-2777. doi: 10.5923/j.ajmms.20261606.02.
1. Introduction
- Immunization is widely recognized as a fundamental strategy for reducing the burden of infectious diseases and improving population health [1,3]. The introduction of vaccination programs has significantly decreased morbidity and mortality associated with vaccine-preventable infections [3,10]. Although vaccines undergo rigorous safety evaluation, some individuals may experience short-term reactions after immunization [1,5]. These reactions are usually mild and temporary, such as low-grade fever or local discomfort, but they may cause concern among parents and caregivers [5,11].Public perception of vaccine safety plays an important role in maintaining adequate immunization coverage [4,7]. Misinterpretation of expected post-vaccination reactions may contribute to vaccine hesitancy and reduced adherence to recommended schedules [4,15]. In this context, healthcare professionals, particularly nurses, have a key responsibility in ensuring safe and effective immunization practices [2,9]. Their duties include maintaining appropriate storage conditions, preparing vaccines correctly, administering injections according to established protocols, and observing patients after vaccination [2,11].In addition to technical responsibilities, nurses provide essential educational support to parents and caregivers [9,14]. Clear communication regarding possible reactions, expected recovery, and warning signs requiring medical attention helps improve understanding and reduces unnecessary anxiety [14,15]. Early identification and proper documentation of post-vaccination reactions also contribute to strengthening patient safety and improving surveillance systems [1,11].Given the importance of nursing involvement in immunization services, evaluating their role in preventing and managing post-vaccination reactions is necessary [2,9]. This study was conducted to assess nursing practices related to the prevention of post-vaccination adverse effects and to examine factors influencing their effectiveness in outpatient clinical settings.
2. Materials and Methods
- A descriptive cross-sectional study was conducted to evaluate the occurrence of post-vaccination reactions in children and to examine the contribution of nursing practice to their prevention during routine immunization. The research was carried out in two outpatient polyclinics located in different settings: 25-OP in Qibray district representing a rural area, and 7-OP in Tashkent city representing an urban population. The total sample comprised 100 parents (50 from each clinic) selected through convenience sampling from parents who brought their children for routine scheduled vaccinations during the data collection period. The study included parents of children who received scheduled vaccinations according to the national immunization program. Participation was voluntary, and written informed consent was obtained from all respondents prior to data collection. The study was conducted in accordance with ethical principles for clinical research, and the research protocol received approval from the institutional ethics committee of Tashkent State Medical University prior to data collection.Information was collected using a structured questionnaire designed to assess the presence, type, and perceived severity of post-vaccination reactions. Since multiple responses were allowed, more than one reaction could be recorded for each child. In addition, relevant clinical information documented by healthcare personnel during routine practice was reviewed to ensure data completeness.The main variables of interest included common post-vaccination reactions such as fever, local symptoms at the injection site (pain and redness), irritability, and allergic manifestations. Additional variables included the type of vaccine administered and parental concerns related to possible adverse reactions. Particular attention was given to nursing activities, including pre-vaccination assessment, compliance with vaccine storage and administration standards, post-vaccination observation, documentation of reactions, and provision of recommendations to parents regarding home care and monitoring.Data processing and analysis were performed using SPSS statistical software (version 26.0). Descriptive methods were applied to calculate frequencies and percentages. Comparative analysis between the rural and urban clinics was conducted using the chi-square (χ²) test with 1 degree of freedom; 95% confidence intervals were calculated for proportions where appropriate. Statistical significance was defined as a p-value less than 0.05. It should be noted that, as a cross-sectional study design, the findings do not allow causal inferences to be drawn between nursing practices and vaccination outcomes. All collected information was anonymized, and confidentiality of participants was maintained in accordance with ethical research principles.
3. Result and Discussion
- The analysis of post-vaccination reactions was based on information obtained from parental questionnaires and medical records in two outpatient clinics representing rural (25-OP) and urban (7-OP) populations. Since multiple responses were permitted, more than one reaction could be identified in an individual child. The findings indicated that the majority of observed reactions were mild and temporary in nature.Among the reported symptoms, irritability and restlessness were the most frequently noted behavioral changes following immunization. This reaction was reported in a high proportion of children in both clinics, accounting for 44.0% in the rural setting (25-OP) and 45.8% in the urban setting (7-OP). An increase in body temperature was the most commonly reported reaction overall, affecting 78.0% of children in 25-OP and 60.4% in 7-OP (χ² = 3.24, df = 1, p = 0.072). Local reactions, including pain and redness at the injection site, were documented in both groups but occurred less frequently compared to systemic symptoms.Allergic manifestations were uncommon and were recorded in 11.1% of cases in the rural clinic and 2.9% in the urban clinic. Importantly, no severe adverse events or complications were identified during the study period. According to established international criteria, all recorded reactions were classified as mild and resolved without the need for medical intervention [1,5,11]. Comparative evaluation did not reveal meaningful differences between rural and urban populations, suggesting consistent immunization safety across both settings.Analysis according to vaccine type showed that transient reactions were more frequently reported after administration of the pentavalent vaccine. Based on parental observations, such reactions were noted in 60.0% of cases in the rural clinic and 95.8% in the urban clinic. The higher reactogenicity of the pentavalent vaccine can be explained from an immunological perspective: this combination vaccine simultaneously activates immune responses against five antigens (diphtheria, tetanus, pertussis, Haemophilus influenzae type b, and hepatitis B), resulting in a more pronounced pro-inflammatory cytokine release, particularly interleukin-6 and tumor necrosis factor-alpha, which accounts for the increased incidence of systemic reactions such as fever and irritability compared to monovalent or less complex vaccines [10,11]. In contrast, fewer reactions were associated with pneumococcal, rotavirus, and measles-containing vaccines. A notable proportion of parents reported no observable reactions following immunization, accounting for 30.0% in the rural group and 4.2% in the urban group.These findings are consistent with international evidence indicating that most post-vaccination reactions are mild and self-limiting [1,5,10]. Tafuri et al. (2014) similarly reported that fever and local site reactions constitute the most prevalent AEFI categories across different immunization settings, with rates comparable to those observed in the present study [5]. The predominance of minor symptoms such as fever and local discomfort reflects the expected physiological immune response following vaccination rather than pathological complications [5,11]. The absence of severe adverse outcomes further supports the established safety profile of routine immunization programs [1,3]. These observations align with WHO global AEFI surveillance data, which consistently indicate that severe reactions following routine childhood immunization occur at very low rates globally [1,11]. The results also highlight the important role of nursing supervision, including post-vaccination observation and parental education, in ensuring early identification and appropriate management of expected reactions, consistent with recommendations from the Immunization Action Coalition [2,9].
|
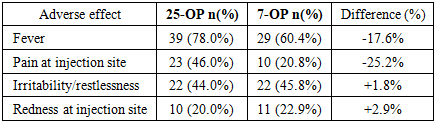
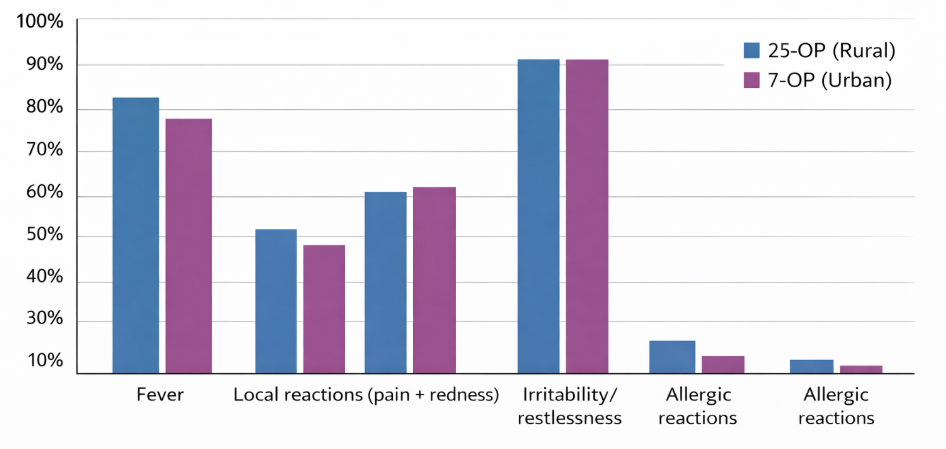 | Figure 1. Distribution of post-vaccination adverse effects in rural and urban outpatient clinics |
4. Conclusions
- The findings of the present study demonstrate that post-vaccination reactions observed in both rural and urban outpatient clinics were mainly mild, short-term, and resolved without medical intervention. No severe complications were identified, supporting the established safety of vaccines used in routine immunization programs. The results emphasize the important contribution of nursing practice in ensuring vaccination safety. Careful pre-vaccination assessment, compliance with recommended administration procedures, appropriate observation after immunization, and clear parental guidance were key factors associated with favorable outcomes. In addition, effective communication between nurses and parents contributed to improved understanding of expected reactions and appropriate home management. Strengthening professional training of nursing staff and maintaining adherence to standardized immunization protocols may further enhance patient safety and increase confidence in vaccination services. These findings highlight the essential role of nursing support as part of safe and effective immunization practice.