-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(5): 2739-2742
doi:10.5923/j.ajmms.20261605.98
Received: Apr. 20, 2026; Accepted: May 17, 2026; Published: May 30, 2026

Optimization of Diagnostic Tactics for Necrotizing Enterocolitis in Newborns
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLFoziljonzoda Maftuna, Atakulov Jamshed Ostonokulovich, Garifulina Lilya Maratovna
Department of Children's Surgery No.1, Samarkand State Medical University, Samarkand, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Necrotizing enterocolitis (NEC) remains one of the most severe pathologies of the neonatal period, accompanied by high mortality and the risk of severe complications. The aim of this study was to optimize diagnostic tactics for NEC in newborns based on a comprehensive assessment of C-reactive protein (CRP), fecal calprotectin, and transvesical intra-abdominal pressure (ITP). The study included 68 newborns suspected of NEC, divided into the main and control groups. It has been established that the combined use of biochemical and instrumental markers increases the sensitivity of early disease diagnosis to 93.4%. A statistically significant correlation was identified between an increase in calprotectin levels, CRO, and an increase in intra-abdominal pressure. The results obtained confirm the high diagnostic value of a comprehensive approach in the early detection and prognosis of NEC severity.
Keywords: Necrotising enterocolitis, C-reactive protein, Calprotectin, Transvesical intra-abdominal pressure, Newborns, Diagnosis
Cite this paper: Foziljonzoda Maftuna, Atakulov Jamshed Ostonokulovich, Garifulina Lilya Maratovna, Optimization of Diagnostic Tactics for Necrotizing Enterocolitis in Newborns, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2739-2742. doi: 10.5923/j.ajmms.20261605.98.
1. Introduction
- Necrotizing enterocolitis (NEC) is one of the most severe and socially significant diseases of the neonatal period, characterized by the development of inflammatory-necrotic lesions of the intestinal wall with a high risk of perforation, sepsis, and death. The disease is primarily found in premature newborns and children with extremely low birth weight, which determines the particular relevance of the problem in modern neonatology and pediatric surgery [1]. Despite significant achievements in the field of intensive neonatal therapy, improvement of artificial lung ventilation methods, parenteral nutrition, and antibacterial therapy, morbidity and mortality rates in NEC remain consistently high. According to various studies, the incidence of NEC development among premature infants ranges from 5 to 15%, and mortality in severe forms of the disease can reach 30-50%. A particularly unfavorable prognosis is observed in newborns with extremely low body weight, pronounced hypoxia, septic complications, and multi-organ failure. The pathogenesis of necrotizing enterocolitis is multifactorial and has not been fully studied to date. The disease is based on disorders of intestinal perfusion, immaturity of the immune system and intestinal barrier function, dysbiosis, and an excessive inflammatory reaction of the newborn's body [2]. Significant role is played by hypoxic-ischemic lesions of the intestinal wall, impaired microcirculation, and activation of pro-inflammatory cytokines, leading to the progression of necrotic changes. Clinical diagnosis of NEC in the early stages of the disease presents significant difficulties due to the nonspecific nature of the symptoms. Initial manifestations of the disease may include abdominal bloating, delayed evacuation of gastric contents, unstable body temperature, episodes of apnea, lethargy, and signs of intestinal dysfunction, which are often encountered in other pathological conditions of the neonatal period. In this regard, the timely diagnosis of NEC remains one of the most complex tasks in neonatology [3].Traditional diagnostic methods, including laboratory indicators of inflammation and radiological signs, often identify the disease at the stage of pronounced morphological changes in the intestinal wall. Classic radiological symptoms, such as intestinal wall pneumatosis, portal venous gasemia, and free gas in the abdominal cavity, are relatively late manifestations of the pathological process. This significantly limits the possibilities for early initiation of pathogenetically grounded treatment. In recent years, special attention has been paid to the search for highly sensitive biomarkers of early inflammatory intestinal damage [4,11]. One of the promising laboratory indicators is C-reactive protein (CRP), which is a protein of the acute phase of inflammation. An increase in CRP levels reflects the activity of the systemic inflammatory process and can be used to assess the severity of NEC and the effectiveness of the therapy being administered. However, the isolated use of this indicator is limited by its insufficient specificity. Significant scientific interest is in the study of fecal calprotectin—a calcium-binding protein of neutrophilic origin that is considered a marker of inflammatory damage to the intestinal mucosa. An increase in the concentration of calprotectin in the stool indicates the activation of neutrophilic inflammation and the disruption of intestinal barrier integrity [5,2]. A number of studies demonstrate the high sensitivity of this marker in the early diagnosis of inflammatory bowel diseases, including NEC in newborns. An additional direction of modern diagnostics is the assessment of intra-abdominal pressure. The development of abdominal hypertension in NEC is accompanied by the deterioration of microcirculation, the progression of intestinal wall ischemia, and the disruption of vital organ functions. The most informative and minimally invasive method for monitoring intra-abdominal pressure is considered to be trans-vezikal measurement, which allows for an objective assessment of the severity of intra-abdominal disorders in newborns [6,8].Despite the existence of numerous studies dedicated to specific aspects of NEC diagnostics, issues regarding the integrated use of biochemical and instrumental markers remain insufficiently studied. There are no unified algorithms for early diagnosis that allow for timely prediction of the severity of the disease's course and the risk of complications. In this regard, the development of an optimized diagnostic tactic based on a comprehensive assessment of C-reactive protein levels, calprotectin, and transvesical intra-abdominal pressure is a pressing scientific and practical task in modern neonatology and pediatric surgery. Implementing such an approach will increase the effectiveness of early diagnosis, improve treatment outcomes, and reduce mortality rates in newborns with necrotizing enterocolitis [7,12].Setting the taskThe aim of the study is to develop an optimized diagnostic tactic for neonatal necrotizing enterocolitis based on a comprehensive analysis of: C-reactive protein levels; fecal calprotectin; and transvesical intra-abdominal pressure.Research objectives: to evaluate the diagnostic significance of CRO in NEC; to study changes in calprotectin levels in newborns; to determine the relationship between intraperitoneal pressure and disease severity; and to develop a comprehensive diagnostic algorithm.
2. Research Methodology
- This study is dedicated to optimizing diagnostic tactics for neonatal necrotizing enterocolitis based on a comprehensive assessment of C-reactive protein levels, fecal calprotectin, and transvesical intra-abdominal pressure.The study was of a prospective clinical and laboratory nature and was conducted in the conditions of the neonatal intensive care and resuscitation department, as well as the pediatric surgery department. The analysis covered the observation period of newborns with clinical signs of necrotizing enterocolitis. The study included 68 newborns receiving inpatient treatment. All patients were divided into two groups:The main group consisted of 38 newborns with a confirmed diagnosis of necrotizing enterocolitis;The control group consisted of 30 newborns without clinical and laboratory signs of NEC.The diagnosis of necrotizing enterocolitis was established based on clinical manifestations, laboratory data, and instrumental research methods according to the modified Bell classification.
3. Research Results
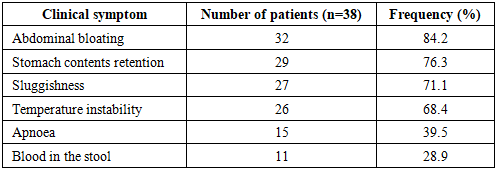
- During the study, the clinical, laboratory, and instrumental indicators of 68 newborns included in the study were analyzed. The main group consisted of 38 newborns with a confirmed diagnosis of necrotizing enterocolitis, while the control group consisted of 30 children without signs of inflammatory-necrotic intestinal lesions. Among the newborns in the main group, premature infants with low and extremely low birth weight predominated. The average gestational age was 31.4±2.6 weeks, and the average body weight was 1560±320 g. NEC was most frequently diagnosed in children who had undergone intrauterine hypoxia, respiratory disorders, and prolonged parenteral nutrition [9,10].Clinical resultsUpon admission, most newborns in the main group exhibited pronounced signs of intestinal dysfunction and a systemic inflammatory reaction. The most common clinical symptoms were:abdominal bloating - in 84.2% of patients;delayed evacuation of gastric contents - in 76.3%;instability of body temperature - 68.4%;lethargy and decreased motor activity - 71.1%;episodes of apnoea - 39.5%;hemorrhagic impurities in the stool - 28.9%.It was established that the severity of clinical manifestations was directly dependent on the stage of NEC according to the Bell classification.
|
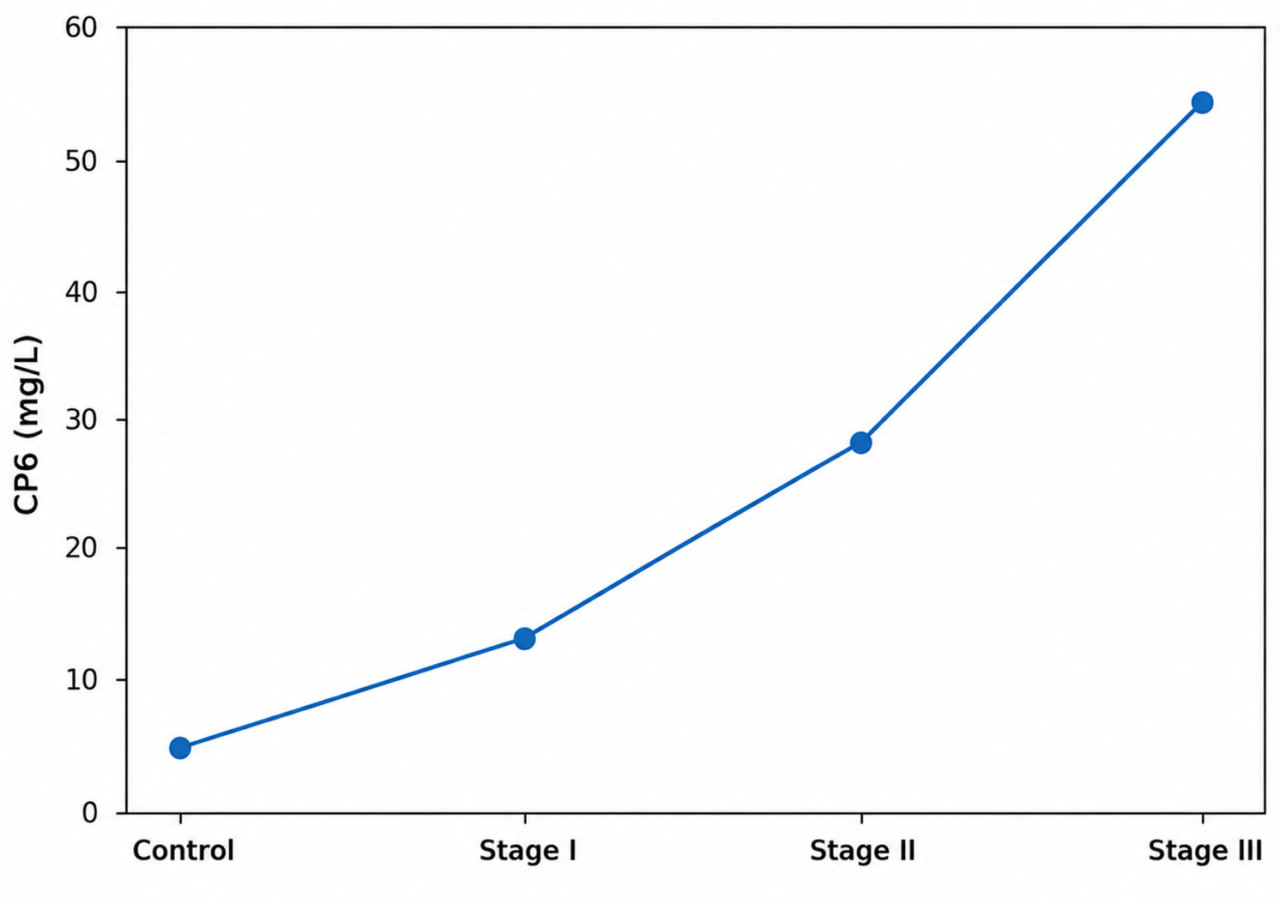 | Figure 1. Dynamics of C-reactive protein levels |
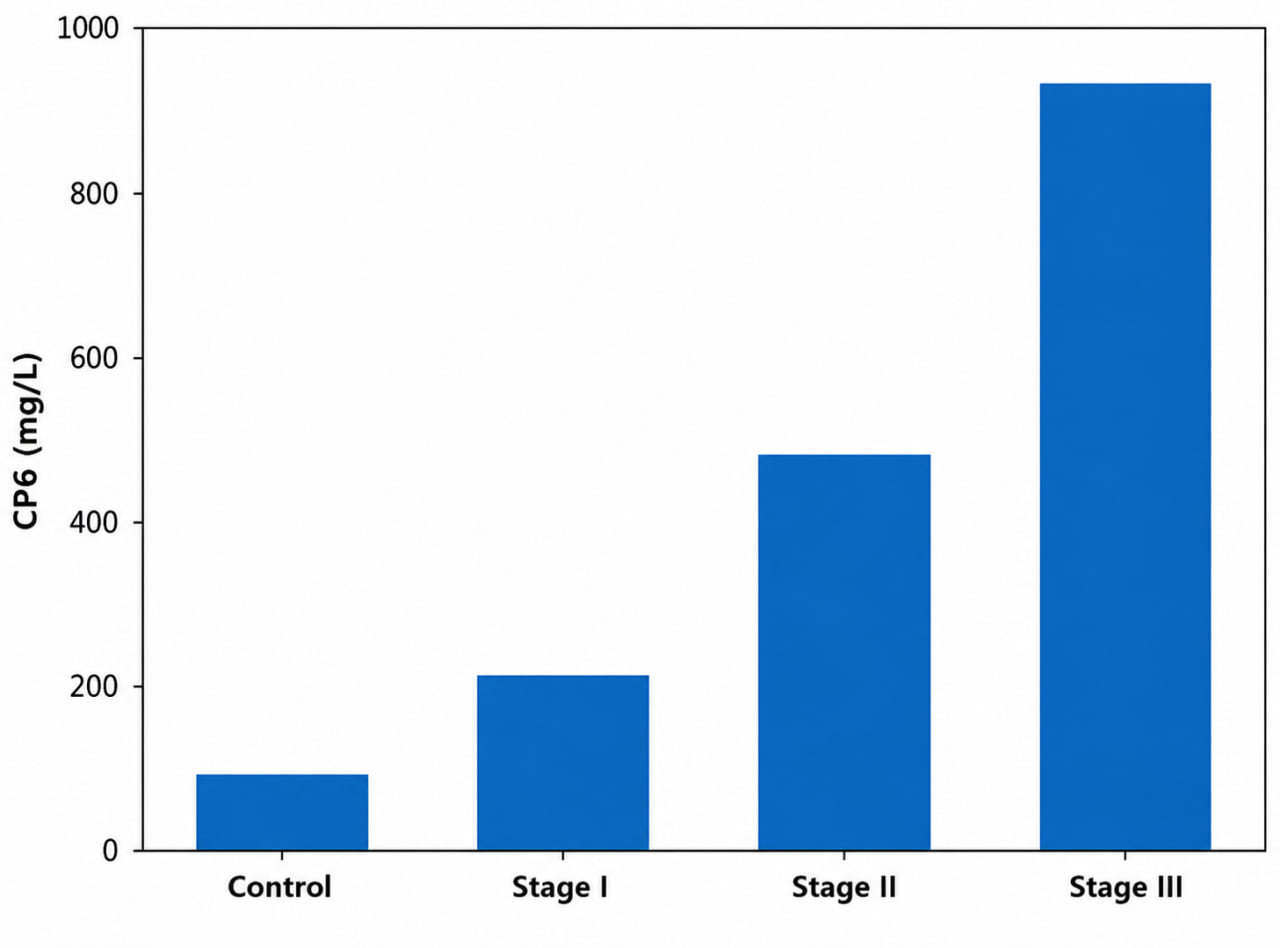 | Figure 2. Change in calprotectin levels |
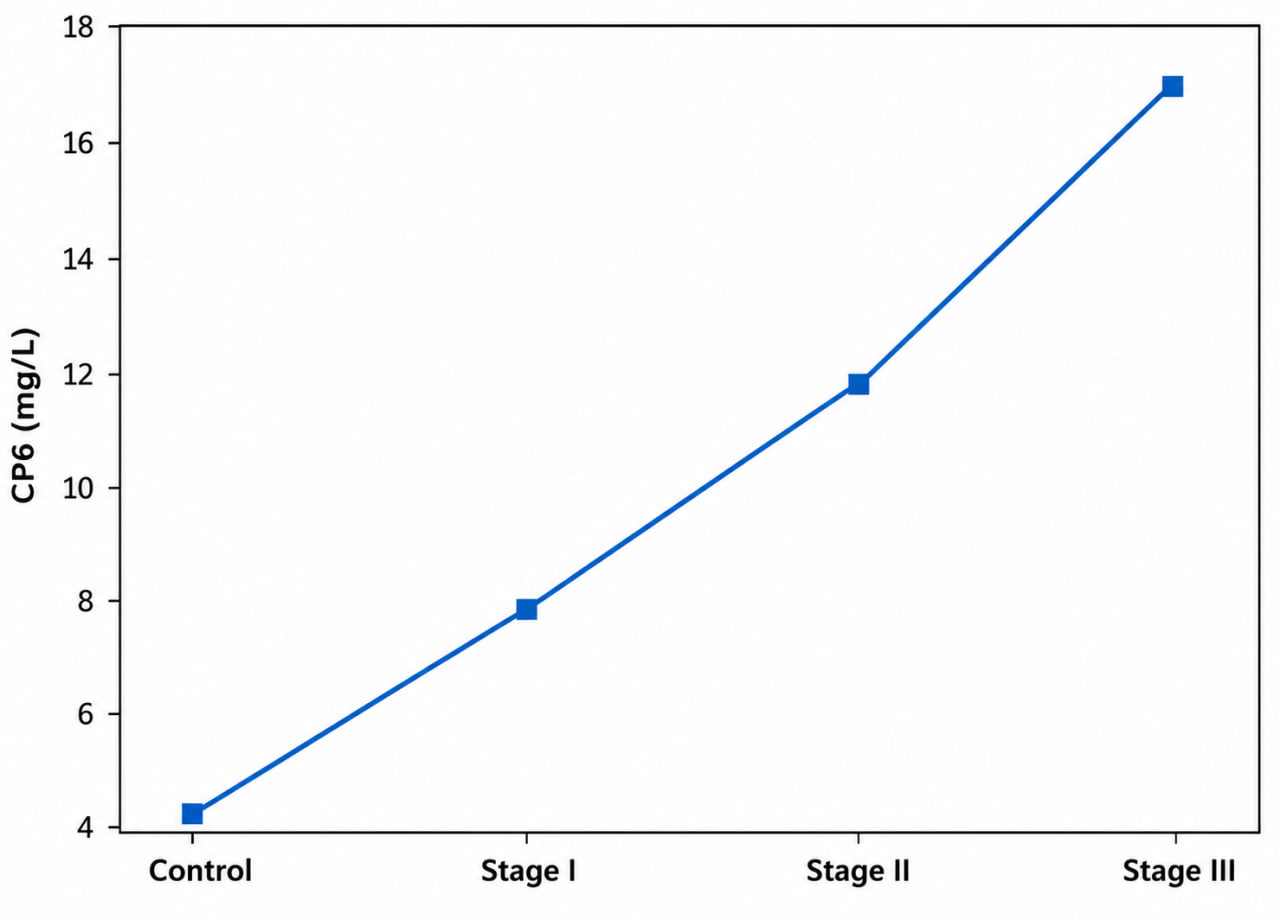 | Figure 3. Changes in intra-abdominal pressure |
|

4. Discussion
- The study results indicate the high diagnostic significance of calprotectin as an early marker of inflammatory intestinal damage. An increase in the level of this protein was noted in the early stages of NEC, which allows it to be used as a predictor of disease progression.C-reactive protein demonstrated a pronounced dependence on the degree of the inflammatory process, but its increase was primarily observed in the development of a systemic inflammatory reaction. Measuring intra-abdominal pressure made it possible to objectify the severity of abdominal disorders and identify signs of abdominal hypertension associated with a high risk of intestinal necrosis. The comprehensive use of these diagnostic criteria ensures higher informativeness compared to the application of individual methods.
5. Conclusions
- The levels of C-reactive protein, calprotectin, and intraperitoneal pressure significantly increase with the progression of necrotizing enterocolitis in newborns. Fecal calprotectin is the most sensitive early biomarker of inflammatory intestinal lesions. Transvesical measurement of intra-abdominal pressure allows for the timely detection of abdominal hypertension development.Comprehensive diagnostic tactics increase the sensitivity of early diagnosis of NEC to 93.4% and contribute to the timely selection of treatment tactics. The obtained results can be used to improve diagnostic protocols and monitoring of newborns suspected of necrotizing enterocolitis.