Turakulov Zoirjon Shokirovich1, Gafurov Adham Anvarovich2, Nematjonov Farrukh Zokirjon ugli3, Bozorov Shavkat Tojiddinovich4, Toshboev Sherzod Olimovich5
1Assistant, Department of Pediatric Surgery for the Faculty of Medicine, Andijan State Medical Institute, Andijan, Uzbekistan
2Doctor of Medical Science, Professor, Head of the Department of Pediatric Surgery, Andijan State Medical Institute, Andijan, Uzbekistan
3Assistant, Department of Pediatric Surgery, Andijan State Medical Institute, Andijan, Uzbekistan
4PhD., Associate Professor, Department of Pediatric Surgery, Andijan State Medical Institute, Andijan, Uzbekistan
5Department of Anesthesiology and Emergency Medicine, Andijan State Medical Institute, Andijan, Uzbekistan
Correspondence to: Turakulov Zoirjon Shokirovich, Assistant, Department of Pediatric Surgery for the Faculty of Medicine, Andijan State Medical Institute, Andijan, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
Surgical management of children born with intravesical ureterocele is usually based on open and transurethral ureterocele excision, but vesicoureteral reflux (VUR) is observed in 12-43% of cases after these procedures. Therefore, improving technical approaches to transurethral incision of intravesical ureterocele allows to reduce the risk of possible complications in the postoperative period and to reduce the number of re-surgical interventions. Methodical recommendation describes methods of increasing the effectiveness of surgical treatment by improving technical approaches to transurethral incision in determining the tactics of treatment of ureterocele in the introvesical form in children. Methodological instruction is intended for pediatric urologists, functional diagnostic specialists of urology departments of regional children's medical and preventive institutions.
Keywords:
Vesicoureteral reflux, Intravesical ureterocele, Exosonography, Resistance index, Pulsation index
Cite this paper: Turakulov Zoirjon Shokirovich, Gafurov Adham Anvarovich, Nematjonov Farrukh Zokirjon ugli, Bozorov Shavkat Tojiddinovich, Toshboev Sherzod Olimovich, Doppler Exosonography as a Method for Assessing Obstruction and Renal Hemodynamics in Children with Intravesical Ureterocele, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2732-2738. doi: 10.5923/j.ajmms.20261605.97.
1. Introduction
Intravesical ureterocele is one of the most common congenital malformations of the urinary system, with a prevalence ranging from 1:500 to 1:5000 [1,3,5,6]. This anomaly is 4-7 times more common in girls than in boys [2,4]. According to the literature, in 80% of patients, ureterocele is located in the upper ureter of the duplicated kidney. Ectopia of the ureteral orifice is detected in 60% of duplicated kidneys, and vesicoureteral reflux in the lower part of the duplicated kidney is detected in 20-40%. Ureterocele is often associated with the upper segment of the duplicated kidney and in most cases causes the development of primary obstructive megaureter [5,7,9,11]. Although there are various surgical techniques for UTI, all children with orthotopic ureterocele should undergo a transurethral incision in the postnatal period. On the contrary, in the ectopic type, transurethral correction (intravesicalization) can be performed to prevent obstruction and restore renal hemodynamics, which can be followed by simultaneous ureteral reimplantation and ureteroceleectomy at a later stage. Therefore, diagnosis by type of ureterocele is important in determining surgical tactics. Intravesical ureterocele and its complications require different surgical approaches. The postoperative rehabilitation process is also of great importance, as it directly affects the child’s quality of life [8,10,12].
1.1. Purpose of the Study
Improving the effectiveness of surgical treatment by improving technical approaches to endoscopic transurethral incision of intravesical ureterocele in children.
2. Materials and Methods
The research study analyzed statistical data on the number of patients admitted to the urology department of the Andijan Regional Children's Multidisciplinary Medical Center (ARCHMMC) with a diagnosis of IU and their additional comorbidities during 2014-2025. These analyses examined the complexity of each case, the various diagnostic tests used in the diagnosis, the surgical procedures performed, and their level of effectiveness. The results of intravesical ureterocele after surgical (control group) and endoscopic transurethral treatment (main group) were analyzed, and the most effective methods of surgical intervention were identified by analyzing the comparative results between these methods.
2.1. Study Design
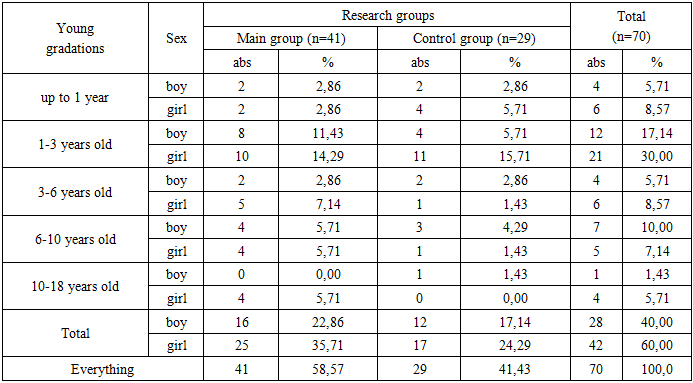
The distribution of children with intravesical ureterocele among congenital anomalies of the renal urinary tract by gender, age gradation, and study group is presented in Table 1.Table 1. Distribution of patients diagnosed with intravesical ureterocele according to sex, age gradations and research groups
 |
| |
|
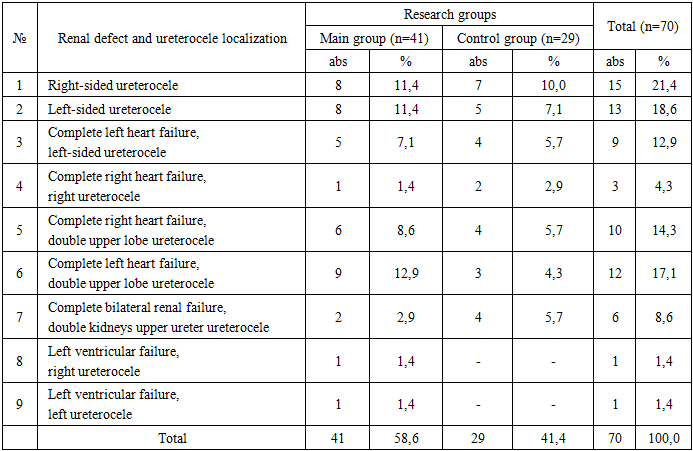
This table shows that the majority of patients admitted with intravesical ureterocele (n=33; 47.1%) were children aged 1-3 years, of whom the proportion of boys was (n=12; 17.1%) and girls (n=21; 30.0%), and their proportion was found to be higher than that of boys.Table 2. Distribution of renal failure and intravesical ureterocele according to localization in patients in the study groups (abs, %)
 |
| |
|
As can be seen from Table 2, in terms of localization of intravesical ureterocele, right-sided solitary intravesical ureterocele (n=15; 21.4%) was more common in both groups than left-sided (n=13; 18.6%) ureterocele. Complete duplication of kidneys, and ureterocele of the upper ureter with duplication of the right side (n=10; 14.3%) and left-sided (n=12; 17.1%) were more common. In the study, complete duplication of kidneys, ureterocele of the upper ureter with duplication of the kidneys, and ureterocele of the upper ureter with duplication of the kidneys were also found in 8.6%.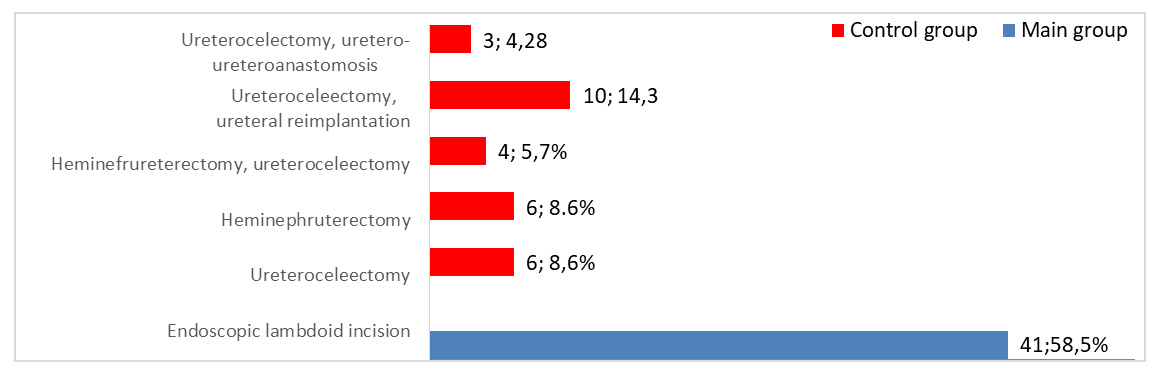 | Figure 1. Comparative analysis of the types of operations performed in research groups according to the gender of patients |
The table data revealed that among the patients in the control group, the proportion of patients who underwent ureteroceleectomy and ureteral reimplantation was higher (n=10; 14.3%). The proposed method of endoscopic transurethral incision was the lambdoid incision (n=41; 58.5%). In both groups, the proportion of girls was higher than that of boys.Based on the main goals and objectives of the guideline, a comparative analysis was conducted of the endoscopic transurethral lambdoid incision method for the intravesical form of ureterocele with traditional treatment methods in terms of the lower rate of various complications that may occur in the postoperative period. For this purpose, the results of treatment and observation of 41 patients admitted to the hospital with the diagnosis of "intravesical form of ureterocele" from among the children involved in the study were used.From the total number of patients, according to the distribution of patients according to the classification of the American Academy of Pediatrics according to the international classification, 41 patients with intravesical ureterocele underwent exosonographic, radiographic and general excretory urography examinations at MSKT. It should be noted that all X-ray examinations were carried out after 1 day of preparation after the patients were admitted to the hospital, while the sonography examination was carried out not only from the postnatal but also from the antenatal period for the purpose of exoscreening.Research methods. Along with generally accepted clinical and laboratory examination methods, echosonography and radiographic examination methods were also performed.Echosonography. Ultrasound sonography of the retroperitoneal cavity was performed on the ultrasound diagnostic system “Xario 200, TUS-X200” (Toshiba Medical system corporation, Japan) using 9-15 MHz sector, linear matrix and convex sensors of the 35С50ЕА, 35С20ЕА models. All sonogram images are performed in real time. Before the examination, the patients' gastrointestinal tract is cleared of feces and gases, and the urinary bladder is filled with urine as much as possible. 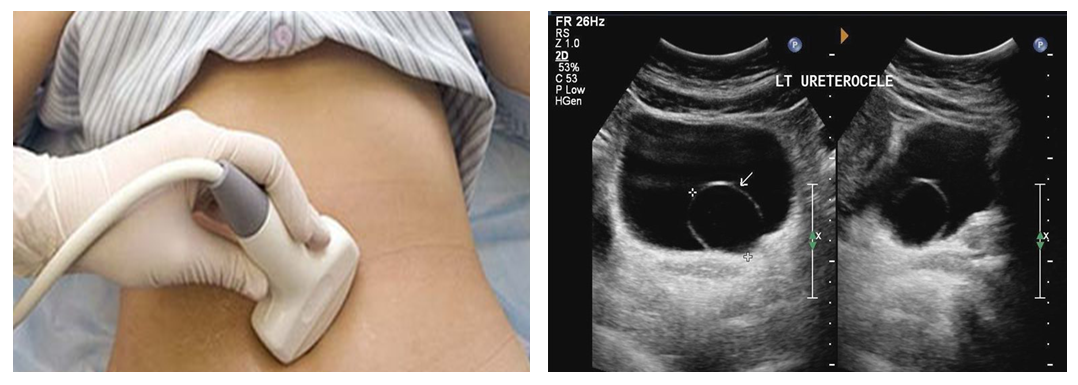 | Figure 2. Exosonography examination. Solitary intravesical ureterocele |
At the same time, one of the main tasks was to assess intrarenal arterial blood flow, determine the hemodynamic significance of the obstruction, and monitor the dynamics of postoperative recovery. To this end, standard sonography of the kidneys and urinary tract was performed, starting with color Doppler.Radiological examination methods. The examination consisted of abdominal radiography, as well as micturition cystourethrography. Radiological examination of the urinary system was performed by taking serial digital images on the Flexa Vision (Shimadzu Corporation, Japan) apparatus. Serial images were taken with the patients lying on their backs (Fig. 3).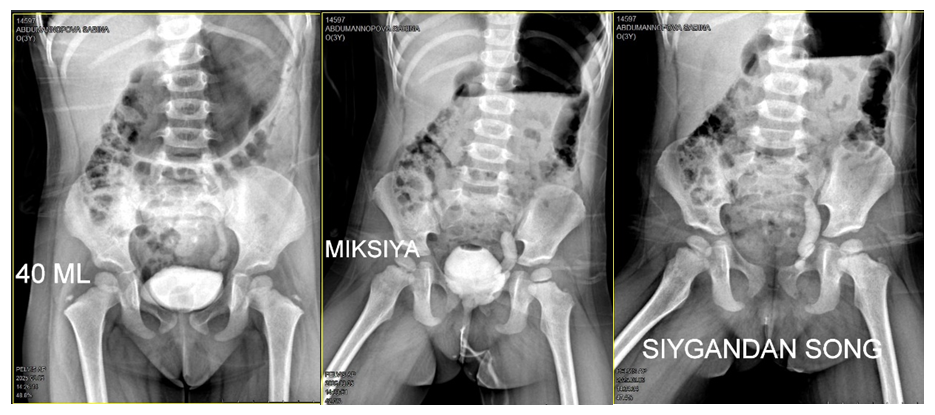 | Figure 3. Cystography (A), micturition cystography (B), after emptying the bladder (C) |
In patients diagnosed with intravesical urethrocele, micturition cystourethrography examination was performed in order to diagnose QSNR, type, and levels, to evaluate the posterior urethra.Endoscopic transurethral removal of intravesical urethrocele (lambdoid incision) technique. Endoscopic transurethral lambdoid incision of intravesical ureterocele in children was performed under the guidance of a pediatric cystoscope “4-6 Fr, optical system 0°, Karl Storz”. In all patients, the cystoscopy procedure was performed under general anesthesia, in real-time mode, by endoscopic transurethral approach. Patients were placed lithotomy without special preparation, and the surgical field was properly cleaned with the antiseptic substance “betadine”. Patients are placed lithotomy without special preparation and the surgical field is properly cleaned with the antiseptic substance "betadine". Then the pediatric cystoscope is treated with "satigel". The cystoscope is inserted transurethrally through the meatus under visual control with a stream of saline solution (0.9% NaCl, 37°C) through the urethra into the bladder and the bladder is filled with saline. During the examination, the external urethra, the mucous membrane of the bladder, and ureterocele are visualized. After a systematic examination of the walls of the ureter, a ureterocele is usually detected in the distal part of the ureter in the branch of the ureter mouth. A special diamond-shaped knife is inserted through the cystoscope irrigation system and a 3-5 mm (l) cut is made at the distal edge of the ureterocele wall (Fig. 4).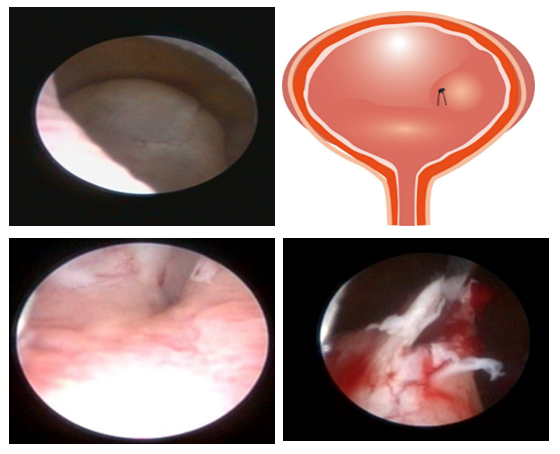 | Figure 4. Stages of endoscopic transurethral lambdoid incision technique for intravesical ureterocene |
After the lambdoid (l)-shaped incision, the upper wall of the ureterocele maintains both fixation points when it is shortened, which does not move the proximal border of the artificial opening, since it does not have a free part directed perpendicular to the axis of the urethra. Therefore, the length of the submucosal part of the urethra remains unchanged and depends only on the length of the cut section. When the upper and lower walls of the ureterocele shrink, the urethral orifice is firmly closed, which improves the anti-reflux function.Hemodynamic parameters are measured in the intrarenal arteries using spectral Doppler mode. Doppler measurements are usually performed at the level of the intrarenal interlobar or arcuate arteries.The following main velocity parameters are determined in spectral Doppler recording: maximum systolic velocity - Vs; end diastolic velocity -Vd and average velocity -Vmean.The resistance index (IR) is calculated using the following formula: This formula shows the relative difference between the systolic and diastolic phases of blood flow. If the diastolic flow decreases, the figure of the formula increases and the IR value increases. This indicates an increase in intrarenal resistance. Thus, an increase in IR indicates an increasing hemodynamic significance of the obstruction.The pulsatility index (PI) is calculated according to the following formula:
This formula shows the relative difference between the systolic and diastolic phases of blood flow. If the diastolic flow decreases, the figure of the formula increases and the IR value increases. This indicates an increase in intrarenal resistance. Thus, an increase in IR indicates an increasing hemodynamic significance of the obstruction.The pulsatility index (PI) is calculated according to the following formula: PI assesses the amplitude and oscillation of blood flow. It takes into account not only the decrease in diastolic flow, but also the average hemodynamic state over the entire cycle. Therefore, PI may in some cases reflect hemodynamic changes more sensitively than IR.
PI assesses the amplitude and oscillation of blood flow. It takes into account not only the decrease in diastolic flow, but also the average hemodynamic state over the entire cycle. Therefore, PI may in some cases reflect hemodynamic changes more sensitively than IR.
3. Statistical Analysis
Statistical processing of the obtained data was carried out on a MateBook D14 “HUAWEI” personal computer using the proprietary licensed version 27.0 of the IBM SPSS Statistics Base (https://www.ibm.com/spss) statistical package suite under Windows 10 software.Data were analyzed using descriptive statistics, and the parameters were expressed as mean and standard error. Repeated Measures ANOVA was used to assess the dynamics of hemodynamic parameters obtained before and at different time points (1-3 days, 3 months, 6 months) after surgery, and in cases where statistically significant differences were detected, pairwise comparison analysis was performed with Bonferroni correction. To assess the reliability of the results, 95% confidence intervals were calculated. Relative hazard ratio analysis was used to determine the effect of surgical techniques on the risk of complications, and ROC analysis was used to assess diagnostic and prognostic efficacy. In all analyses, statistical significance was considered reliable at p<0.05.Results of the study. As noted above, patients were divided into two groups according to treatment tactics: in the main group, 41 children underwent endoscopic surgery, and in the control group, 29 children underwent traditional open surgery. In order to assess the early postoperative results, the main indicators of renal hemodynamics, IR (resistance index) and PI (pulsatility index), were measured using Doppler before surgery and 1-3 days, 3 months, and 6 months after surgery.Absolute values of hemodynamic parameters and their changes over time are presented in Table 3.Table 3. Dynamics of IR and PI parameters in the early postoperative period in children with intravesical ureterocele (M±SD)
 |
| |
|
Table 3 shows that intrarenal hemodynamics were impaired in both groups before surgery. Preoperative IR values were 0.747±0.036 and 0.749±0.037 in the conventional and endoscopic groups, respectively, and PI values were 1.79±0.22 and 1.81±0.21. The closeness of these values at baseline suggests that the groups were hemodynamically comparable before surgery.These data show that in children with intravesical ureterocele, both surgical methods improve renal hemodynamics in the early postoperative period, but IR and PI values decrease more rapidly and significantly with endoscopic surgery than with conventional surgery.In the next step, the results of RM ANOVA were analyzed to determine the statistical significance of hemodynamic changes (Table 4).Table 4. Integral analysis of the dynamics of hemodynamic parameters in the early postoperative period in children with intravesical ureterocele (RM ANOVA)
 |
| |
|
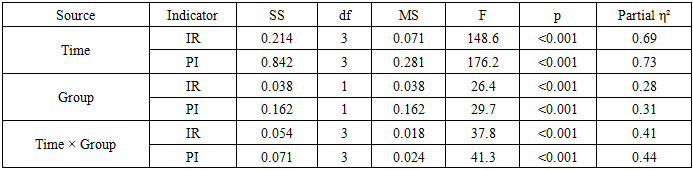
As can be seen from the table data, RM ANOVA analysis revealed several important statistical patterns in the dynamics of hemodynamic parameters in the early postoperative period.First, the effect of time was found to be highly significant (p<0.001). This means that IR and PI improved gradually over time after surgery. Secondly, the effect of surgical technique was also significant (p<0.001). This indicates that the degree of hemodynamic recovery was different between the endoscopic and conventional surgery groups.The most important result was the statistically significant interaction between time and surgical technique (p<0.001). This indicates that hemodynamic recovery after endoscopic surgery was faster than after conventional surgery. Partial eta squared indicators (measure of effect) showed a high power of effect, confirming that the surgical technique had a clinically important effect on hemodynamic recovery. This indicates that the changes in the dynamics of hemodynamic parameters are not random, but rather there are systematic differences associated with time and surgical technique.The time effect for IR was F=148.6 and p<0.001, indicating a significant difference between different time points after surgery. The most important result was the interaction between time and group. F=37.8 for IR and F=41.3 for PI, both p<0.001, indicating that the hemodynamic recovery trajectory was not the same in the two groups. In other words, recovery after endoscopic surgery was not only better, but also faster in terms of time. The partial eta squared values indicate a high strength of the effect: 0.69 for IR and 0.73 for PI indicate a very large effect size for the time effect, while interaction values around 0.41-0.44 indicate a strong interaction with clinical significance.Thus, hemodynamic recovery in the early postoperative period is strongly dependent on the timing and surgical technique, with endoscopic surgery statistically significantly leading to faster normalization of renal hemodynamics. While RM ANOVA confirmed the overall dynamics, we also evaluated pairwise comparisons and confidence intervals to determine which time points were most significant in terms of differences (Table 5).Table 5. Pairwise comparison analysis (Bonferroni) and 95% confidence interval of IR and PI in the early postoperative period
 |
| |
|
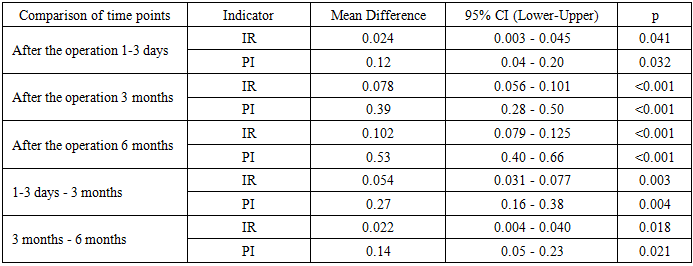
The data in the table show that the postoperative hemodynamic improvement is not only a general trend, but also statistically significant at individual time points. The difference in IR between preoperative and 1-3 days was 0.024, with a p=0.041 result, confirming that the resistance index decreased very early after surgery. This decrease was even more pronounced at 3 months and 6 months, and the p values <0.001 indicate that the changes are highly significant. A significant decrease in IR was also noted in the interval from 1-3 days to 3 months, i.e., the dynamics of recovery was not limited to the first days after surgery, but continued in the following months. A similar picture was observed for PI. The difference between preoperative and 1-3 days was significant with p=0.032, while PI decreased even more significantly at 3 months and 6 months. The fact that the 95% confidence intervals did not cross zero confirms that these differences are stable and reliable. From a clinical point of view, this means that intrarenal resistance and pulsatile oscillations decreased not gradually, but relatively quickly and continuously after surgery. This indicates that a significant improvement in IR and PI indices is observed from 1-3 days after surgery, and by 3 and 6 months these changes become even more pronounced, indicating that hemodynamic recovery has become stable.
4. Discussion
The most common surgical procedure in the neonatal period is endoscopic ureterocele repair. However, some patients may require complete open reconstruction. The choice of surgical intervention depends on the clinical circumstances (eg, dual or single system; presence or absence of ureteral obstruction). The success of endoscopic decompression and the need for reoperation depend on the location of the ureterocele. Endoscopic decompression for intravesical ureterocele is the definitive surgical procedure in approximately 80-90% of cases.Later, the endoscopic incision technique became widespread, and today in most cases this operation is the first stage of surgical treatment. The importance of endoscopic incision is especially great in emergency situations with the development of obstructive pyelonephritis, in young children and with extravesical location of ureterocele. However, 35-73% of patients (according to our data - 62.5%) had indications for repeated operations after endoscopic incision. The main factor determining the need for repeated interventions was the VUR leading to UTI.A meta-analysis by Haddad et al. also showed a decompression rate of almost 90% in endoscopically repaired intravesical ureterocele. The same study described consistent improvement in urethrohydronephrosis in the postoperative period, regardless of the technique used.In patients with urosepsis secondary to obstruction, ureteroceles require immediate decompression, usually through endoscopic incision. Percutaneous drainage is rarely required.Some workers believe that upper urinary tract reconstruction is more effective, which reduces the physical support at the sensory level. However, for specific support, surgical intervention is also needed in the urethrovesical segment.Definitive surgery by heminephricectomy, either open or laparoscopic, is usually performed between six months and one year of age. In patients without renal insufficiency and with a well-functioning upper pole segment of the kidney, radical surgical intervention is ureteroureteroanastomosis (anastomosis of the upper ectopic ureter with the normal lower part of the ureter at the level of the bladder).The data obtained show that good results are achieved with the following approach: Upper pole heminephricectomy was performed in patients without high-pole renal function and without signs of CKD. In patients with CKD and residual ureterocele, ureterocele removal with reimplantation of both ureters and bladder neck reconstruction was performed. The reoperation rate of orthotopic ureterocele due to ineffective endoscopic resection varies from 7 to 23%.The treatment of ureterocele associated with ureteral duplication has undergone significant changes in the last few decades. Given that in most cases the function of the upper segment of the kidney is significantly impaired or absent, the initial treatment consists of removing the ureterocele with simultaneous heminephricectomy and reimplantation of the second ureter - this is called complete reconstruction. Because complete reconstruction in young children is associated with a high risk of complications, an alternative staged approach has been proposed. In the first stage, only the upper half of the kidney was resected, and in the second stage, at an older age, the bladder was operated on. In approximately 50% of patients, a second stage was not necessary, so heminephricectomy became the main treatment option as a first stage or final procedure.
5. Conclusions
The possibility of immediate echosonography for early diagnosis of congenital anomalies of the renal urinary tract in children allows to determine the anatomical structure of the urinary system, assess the degree of obstruction and correctly determine the surgical plan. Also, this method is considered preferable to other methods due to its minimal invasiveness, minimal trauma, low rate of possible postoperative complications, and rapid recovery in patients. Opening of intravesical ureterocele through endoscopic transurethral lambdoid incision allows to reduce the degree of obstruction to 100%, to restore urodynamics and hemodynamics, and to create an antireflux mechanism in the mouth of the urethra.
References
| [1] | V. I. Dubrov, A. V. Strotsky, and A. O. Shkutov, “Effectiveness of endoscopic treatment of ureterocele in duplicated ureter in children,” Russian Journal of Pediatric Surgery, Anesthesiology and Intensive Care, no. 1, 2020. |
| [2] | I. M. Kagansov, D. N. Shchedrov, V. V. Sizonov, V. I. Dubrov, S. G. Bondarenko, G. I. Kuzovleva, A. V. Pirogov, V. G. Svarich, V. M. Orlov, and O. V. Staroverov, “Ureteral stump syndrome after ureteroureterostomy, heminephrectomy and nephrectomy in children,” Vestnik Urologii, no. 4, 2020. |
| [3] | I. M. Kagantsov, V. V. Sizonov, V. I. Dubrov, S. G. Bondarenko, N. R. Akramov, O. S. Shmyrov, G. I. Kuzovleva, R. V. Surov, and A. A. Logval, “First experience of ureteroureterostomy (ureteropyeloanastomosis) in duplex kidney in children,” Vestnik Urologii, no. 4, 2017. |
| [4] | “A step-by-step guide to double-puncture technique for endoscopic management of ureterocele,” vol. 21, 2024. |
| [5] | Z. Alyusuf et al., “Intravesical urachal cyst masquerading as a bladder malignancy: A case report,” Journal of Medical Case Reports, vol. 17, no. 1, p. 364, 2023. |
| [6] | K. Aikins, K. Taghavi, M. Grinlinton, P. Reed, N. Price, and V. Upadhyay, “Cystoscopic transurethral incision in simplex and duplex ureteroceles: Is it the definitive procedure?” Journal of Pediatric Urology, vol. 15, no. 5, pp. 560.e1–560.e6, Oct. 2019. |
| [7] | S. Bayram et al., “Evaluation of management of ureteroceles in our clinic: 8 years of experience,” Cirugía y Cirujanos, vol. 93, no. 1, pp. 1–5, 2025. |
| [8] | C. E. Barnewolt et al., “Contrast-enhanced voiding urosonography. Part 2: Urethral imaging,” Pediatric Radiology, vol. 51, no. 12, pp. 2368–2386, Nov. 2021. |
| [9] | E. C. Benya et al., “Assessment of distal ureteral and ureterovesical junction visualization on contrast-enhanced voiding urosonography,” Pediatric Radiology, vol. 51, no. 8, pp. 1406–1411, 2021. |
| [10] | Z. Bian et al., “Curative effect of laparoscopic ureteral end-to-side anastomosis at the pelvic level for a duplex kidney in children,” Frontiers in Pediatrics, vol. 13, p. 1509039, 2025. |
| [11] | L. A. M. Brinkman et al., “Pop-off mechanisms in fetal megacystis: Extravasation, umbilical cord cyst, ureterocele and megaureter,” Ultrasound in Obstetrics & Gynecology, vol. 65, no. 4, pp. 487–494, 2025. |
| [12] | G. Contini et al., “Voiding cystourethrography in patients undergoing endoscopic decompression of duplex system ureteroceles: To do or not to do?” Pediatric Surgery International, vol. 40, no. 1, p. 103, 2024. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML