-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(5): 2727-2731
doi:10.5923/j.ajmms.20261605.96
Received: Apr. 26, 2026; Accepted: May 20, 2026; Published: May 28, 2026

Personalised Minimally Invasive Approach to Surgical Correction of Acute Cholangitis
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMamatov Karim Saydullaevich1, Sayinaev Farrukh Karamatovich2, Rakhmanov Kosim Erdanovich2
1Department of Surgery, Navoi Branch of the Republican Scientific Centre of Emergency Medicine, Navoi, Uzbekistan
2Department of Surgery, Samarkand State Medical University, Samarkand, Uzbekistan
Correspondence to: Mamatov Karim Saydullaevich, Department of Surgery, Navoi Branch of the Republican Scientific Centre of Emergency Medicine, Navoi, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

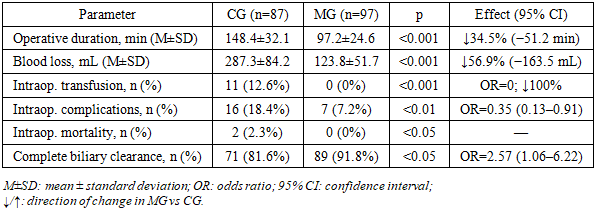
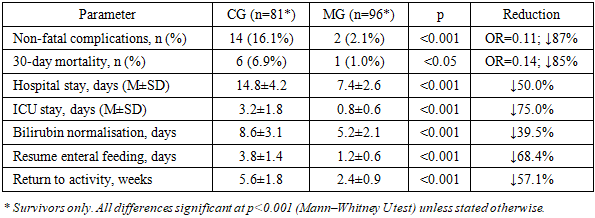
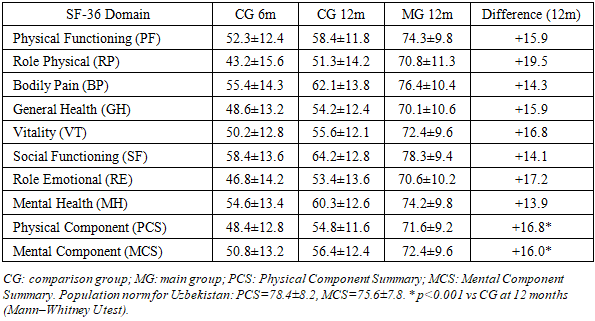
Background: Acute cholangitis remains a life-threatening condition with mortality rates up to 30% in severe forms. Current guidelines (TG18) define timing of decompression but do not prescribe the specific method, leaving a critical gap in personalised treatment algorithms for regional centres with high comorbidity burden. Objectives: To evaluate the clinical efficacy of a personalised minimally invasive (MI) algorithm based on TG18/CCI/ASA stratification, including the Rendez-vous technique and an innovative endosurgical cutting instrument (ESCI, Patent UZ FAP 01283), compared with conventional open surgery. Methods: Comparative cohort study; 184 consecutive patients with acute cholangitis (2019–2025). Comparison group (CG, n=87): predominantly open surgery; Main group (MG, n=97): personalised MI algorithm. Primary endpoints: 30-day complications and mortality; secondary: PHES rate, late complications by aetiology, and SF-36 quality of life at 12 months. Results: MI procedures constituted 90.7% of MG vs 3.4% in CG (p<0.001). Operative time decreased by 34.5% (p<0.001), blood loss by 56.9% (p<0.001). Non-fatal complications fell from 16.1% to 2.1% (OR=0.11; p<0.001); 30-day mortality from 6.9% to 1.0% (p<0.05). PHES rate for choledocholithiasis: 18.3% vs 5.5% (OR=0.26; p<0.05); 0% after Rendez-vous. SF-36 PCS improved by 16.8 points regardless of aetiology (p<0.001). Conclusions: The TG18–CCI–ASA algorithm with Rendez-vous technique and ESCI significantly outperforms open surgery across all measured outcomes, including long-term quality of life.
Keywords: Acute cholangitis, Minimally invasive surgery, Rendez-vous technique, Endosurgical instrument, PHES, Quality of life, SF-36, TG18
Cite this paper: Mamatov Karim Saydullaevich, Sayinaev Farrukh Karamatovich, Rakhmanov Kosim Erdanovich, Personalised Minimally Invasive Approach to Surgical Correction of Acute Cholangitis, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2727-2731. doi: 10.5923/j.ajmms.20261605.96.
1. Introduction
- Acute cholangitis an infectious-inflammatory condition of the biliary tract resulting from the combination of biliary obstruction and bacterial contamination represents one of the most challenging emergencies in abdominal surgery, with global incidence continuing to rise in parallel with the prevalence of cholelithiasis [1,2]. The Tokyo Guidelines (TG18) provide internationally accepted diagnostic criteria and a severity classification comprising three grades: Grade I (mild), Grade II (moderate), and Grade III (severe with organ dysfunction), with corresponding recommendations for the timing of decompression [3]. While TG18 define when to decompress, they do not prescribe how leaving the choice between endoscopic, percutaneous, and open approaches to the individual centre's resources and the surgeon's discretion [4].In Uzbekistan, the epidemiological landscape is further complicated by endemic hepatic echinococcosis in several regions, notably Navoi Province, where rupture of an echinococcal cyst into the biliary ducts accounts for 8–15% of cholangitis cases a proportion substantially exceeding that reported in Western series [5,6]. This specific aetiological variant demands a tailored surgical strategy that extends beyond standard choledocholithiasis protocols.Minimally invasive technologies endoscopic sphincterotomy (EST), laparoscopic cholecystectomy (LC), percutaneous transhepatic cholangiostomy (PTCS), and their combinations — have fundamentally transformed biliary surgery over the past three decades [7,8]. The Rendez-vous technique, combining synchronous antegrade wire guidance by a laparoscopic team with retrograde EST by an endoscopic team, provides a compelling solution when standard ERCP fails due to anatomical obstacles [9]. Despite promising results in small series, its systematic application and outcomes in regional centres of Central Asia remain unreported in the literature.A further unresolved technical challenge concerns destructive phlegmonous cholecystitis with transmural wall thickening (≥5 mm), which renders the gallbladder ungrasped by standard laparoscopic instruments the so-called 'non-grasping gallbladder' phenomenon and Veress needle puncture unfeasible due to fibrous wall induration [10]. The authors developed and patented an original endosurgical cutting instrument (ESCI, Patent UZ FAP 01283) specifically designed to address this challenge through a controlled fundus incision with a disposable, permanently sharp blade.The present study aimed to evaluate the clinical efficacy of a personalised TG18–CCI–ASA-based minimally invasive algorithm, encompassing hybrid procedures, two-stage tactics, the Rendez-vous technique, and the ESCI, compared with conventional open surgery, across intraoperative, early postoperative, and long-term outcomes including health-related quality of life in three aetiological subgroups.
2. Materials and Methods
- This was a single-centre comparative cohort study conducted at the Department of Surgery, Navoi Branch of the Republican Scientific Centre of Emergency Medicine (Navoi, Uzbekistan), from January 2019 to December 2025. Consecutive adult patients with a verified diagnosis of acute cholangitis according to TG18 criteria (definite cholangitis: criteria from groups A + B + C) were enrolled. The study was approved by the Institutional Ethics Committee of Samarkand State Medical University (protocol No. 8/2019). Written informed consent was obtained from all participants.Patients were assigned to two groups by chronological principle: Comparison Group (CG, n=87; 2019–2021) treated with conventional open surgery; and Main Group (MG, n=97; 2022–2025) treated according to the personalised MI algorithm. Exclusion criteria: malignant biliary obstruction, age <18 years, refusal of surgical treatment, and loss to follow-up before 30-day assessment.The personalised algorithm was based on a decision matrix integrating TG18 severity grade, Charlson Comorbidity Index (CCI), and ASA physical status class. For Grade I with CCI≤3 and ASA I–III: simultaneous EST + LC (hybrid, single anaesthesia). When standard ERCP failed (periampullary diverticulum, stone >15 mm, previous Billroth-II gastrectomy): Rendez-vous technique (synchronous two-team: laparoscopic antegrade 0.035-inch guidewire introduction via cystic duct + retrograde EST over guidewire). For Grade II–III with organ dysfunction: two-stage approach (EST/PTCS as first stage followed by LC/OC after stabilisation at 48–72 hours). For biliary strictures: staged biliodigestive anastomosis (PTCS → hepaticojejunostomy after cholangitis resolution, 5–10 days). For hepatic echinococcosis: EST followed by laparoscopic echinococcectomy utilising ESCI for pericyst incision.The Endosurgical Cutting Instrument (ESCI) (Patent UZ FAP 01283, IPC A61B 17/32, registered 21.02.2018; inventors: Mamatov K.S., Malikov Yu.R., Davronov A.U.) comprises a round-cross-section handle (diameter K₁=5 mm, total length K=400 mm) connected to a rectangular parallelepiped working part (length K₂=25 mm) with two longitudinal grooves on opposite faces and a rectangular recess for a disposable sterile surgical blade (No. 11/13/15, width ≤6 mm) secured by a bevel without additional fixation elements. The instrument is fully compatible with standard 5-mm trocars. The disposable blade provides 100% cutting sharpness at each operation, eliminating the 'crushing cut' phenomenon of blunted reusable scissors and enabling precise incision through fibrous-inflammatory tissue resistant to standard instruments (fig. 1).
 | Figure 1. The Endosurgical Cutting Instrument |
3. Results
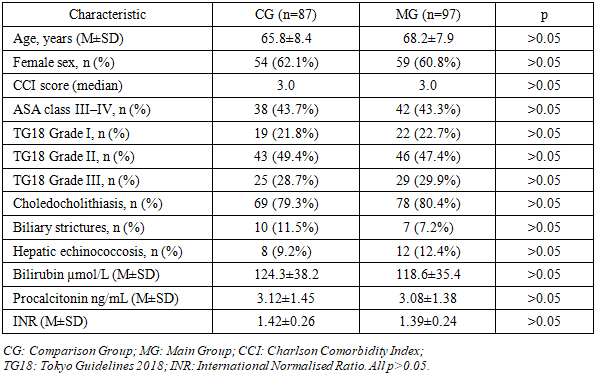
- Both groups were comparable at baseline across all demographic, severity, and biochemical parameters (Table 1). The overall cohort was characterised by advanced age (mean 67.1±5.4 years), significant comorbidity (CCI median 3.0, 45.0% with ≥2 comorbidities), and predominantly moderate-to-severe cholangitis (TG18 Grade II: 48.4%; Grade III: 29.3%). The unique aetiological structure included choledocholithiasis (79.9%), biliary strictures (9.2%), and hepatic echinococcosis (10.9%).
|
|
|
|
4. Discussion
- The present study demonstrates that a personalised, TG18–CCI–ASA-driven minimally invasive algorithm achieves clinically and statistically significant improvements across all measured endpoints from intraoperative parameters through 30-day outcomes to 12-month quality of life compared with predominantly open surgical management of acute cholangitis in a regional centre with a high-risk patient population.The pathophysiological rationale for prioritising endoscopic decompression as the primary intervention is well-established: EST directly eliminates biliary hypertension, interrupting the cholangiovenous reflux–endotoxaemia cascade within 2–6 hours, an effect unachievable by open surgery that introduces additional immunological 'second hit' [11]. Our results confirm this mechanism: the two-stage approach (EST/PTCS → deferred surgery) reduced 30-day mortality 6.9-fold among Grade II–III patients by avoiding full surgical trauma during active sepsis.The Rendez-vous technique, achieving 100% stone clearance and zero PHES in all 12 patients in this series, merits wider adoption at centres managing anatomically complex cholangitis. The technique's superiority over standard ERCP in selected cases is consistent with the meta-analysis by Kedia et al. [9], which reported 90–100% technical success. Our novel finding zero PHES after Rendez-vous at 30 months can be attributed to the precise, guidewire-controlled sphincterotomy minimising collateral sphincter damage, which represents an important contribution to the existing literature.The ESCI (Patent UZ FAP 01283) addresses a specific and hitherto unsolved technical challenge: laparoscopic cholecystectomy in phlegmonous cholecystitis with wall thickness ≥5 mm. The 'non-grasping gallbladder' phenomenon, described by Strasberg (2010) as a recognised factor of difficult cholecystectomy, has no standardised instrumental solution in published literature [10]. Our application of a disposable ultra-sharp blade mounted on the ESCI reduced conversion rate from 96.6% (predominantly open in CG) to 7.1% among phlegmonous cholecystitis cases a result consistent with the 5–8% conversion benchmark for complex cholecystitis at high-volume centres [12]. The instrument's additional applications (Calot's triangle dissection, anastomotic preparation, pericyst incision) underscore a unifying pathomorphological criterion: utility whenever standard scissors fail to achieve a precise cut through fibrotic or parasitically altered tissue.The finding that SF-36 quality of life at 12 months correlates with the type of surgery (ρ=+0.52 for laparoscopic approach vs PCS; p<0.001) rather than initial disease severity represents a novel contribution to the understanding of long-term outcomes following acute cholangitis. Existing literature predominantly reports quality-of-life data after uncomplicated cholecystectomy for cholelithiasis; aetiological-subgroup-specific SF-36 analysis in cholangitis patients has not previously been published [13].Several limitations deserve acknowledgment. First, the non-randomised design, while mitigated by the comparable baseline characteristics and chronological cohort structure, cannot fully exclude selection bias. Second, the shorter follow-up period in the MG (median 18.2 months vs 28.4 months in CG) is an inherent constraint of the prospective component; extended surveillance is ongoing. Third, the absence of preoperative SF-36 values precludes within-patient longitudinal analysis. Fourth, the results derive from a single regional centre in Central Asia with a specific aetiological profile including endemic echinococcosis, which may limit generalisability to centres with different case mixes.
5. Conclusions
- A personalised minimally invasive algorithm based on TG18–CCI–ASA stratification, incorporating hybrid EST+LC, the Rendez-vous technique, staged biliary reconstruction, and the novel ESCI (Patent UZ FAP 01283), significantly outperforms conventional open surgery for acute cholangitis across all key outcomes: intraoperative blood loss (↓56.9%), 30-day mortality (↓6.9-fold), PHES rate in choledocholithiasis (↓70%), late complications in strictures (↓71.4%) and echinococcosis (↓78.8%), and 12-month SF-36 PCS (+16.8 points). The evidence presented establishes that long-term quality of life after acute cholangitis is determined primarily by the nature of the surgical procedure rather than by the severity of the initial condition a clinically actionable insight for surgical planning and post-discharge surveillance. The algorithm is implementable in regional-level surgical departments without specialised infrastructure.