-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(5): 2721-2726
doi:10.5923/j.ajmms.20261605.95
Received: May 10, 2026; Accepted: May 27, 2026; Published: May 28, 2026

Integrated Risk Stratification Score for Individualized Surgical Decision-Making in Benign Thyroid Nodular Disease
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLSalimov Eshdolvat Eshmakhmatovich, Rakhmanov Kosim Erdanovich, Sayinaev Farrukh Karamatovich
Department of Surgery, Samarkand State Medical University, Samarkand, Uzbekistan
Correspondence to: Salimov Eshdolvat Eshmakhmatovich, Department of Surgery, Samarkand State Medical University, Samarkand, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

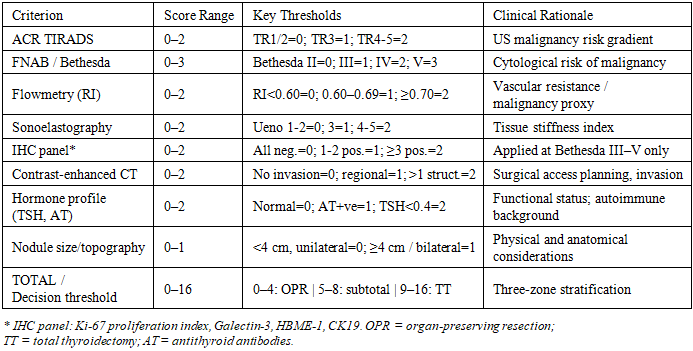
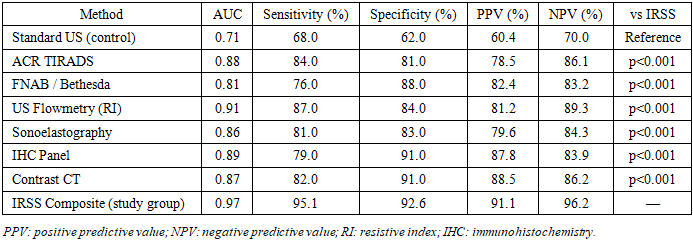
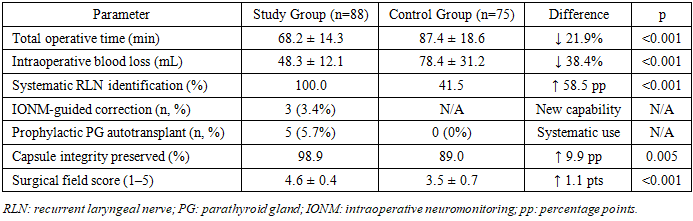
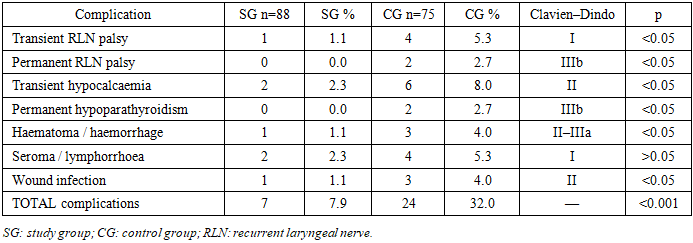
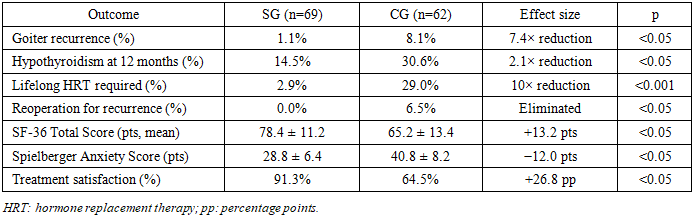
Background: The optimal extent of surgery for benign thyroid nodular disease (BTND) remains contentious. Current guidelines lack a standardised quantitative algorithm integrating multiple pre-operative diagnostic criteria into a reproducible clinical decision tool. Objective: To develop and validate a multi-parameter integrated risk stratification scoring system (IRSS) for individualised surgical volume selection in BTND, and to evaluate the clinical impact of an associated intraoperative innovation bundle. Methods: A prospective comparative study including 163 patients with BTND who underwent thyroid surgery at the Kashkadarya Branch of the Republican Specialized Endocrinological Scientific-Practical Medical Centre (2019–2025). Patients were allocated to a study group (SG, n=88) managed by the IRSS protocol, and a control group (CG, n=75) receiving standard care. The IRSS combines eight criteria: ACR TIRADS category, Bethesda cytology, US flowmetry resistive index (RI), sonoelastography Ueno grade, immunohistochemistry (Ki-67, Galectin-3, HBME-1, CK19), contrast-enhanced CT, thyroid hormone profile, and nodule morphometry (maximum score 16, three risk zones). The SG additionally received a five-technology intraoperative bundle: continuous intraoperative neuromonitoring (IONM) of the recurrent laryngeal nerve (RLN), parathyroid gland flowmetry, Harmonic Focus ultrasonic dissector, and two original instruments (modified retractor; thyroid lobe fixator). Primary outcomes: overall early complication rate, goiter recurrence, and post-operative hypothyroidism. Secondary outcomes: operative parameters and quality of life (SF-36; Spielberger anxiety scale). Results: The IRSS achieved AUC=0.97 (sensitivity 95.1%; specificity 92.6%), compared with AUC=0.71 for standard ultrasound (p<0.001). Organ-preserving surgery was performed in 55.7% of SG vs 33.3% of CG (p<0.05). Overall early complication rate: 7.9% (SG) vs 32.0% (CG) (p<0.001). No permanent RLN palsy or permanent hypoparathyroidism occurred in SG. At median 28.4-month follow-up: goiter recurrence 1.1% vs 8.1% (p<0.05); lifelong hormone replacement 2.9% vs 29.0% (p<0.001); reoperation 0% vs 6.5% (p<0.05). SF-36 total score: 78.4 vs 65.2 (p<0.05). Conclusions: The IRSS provides a reproducible, institution-independent framework for surgical decision-making in BTND that simultaneously reduces complications, recurrence, and iatrogenic hypothyroidism while improving patient-reported outcomes. Wide implementation is recommended.
Keywords: Thyroid nodular disease, Risk stratification, Thyroidectomy, TIRADS, Bethesda system, Intraoperative neuromonitoring, Quality of life, Organ-preserving surgery, Immunohistochemistry, Resistive index
Cite this paper: Salimov Eshdolvat Eshmakhmatovich, Rakhmanov Kosim Erdanovich, Sayinaev Farrukh Karamatovich, Integrated Risk Stratification Score for Individualized Surgical Decision-Making in Benign Thyroid Nodular Disease, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2721-2726. doi: 10.5923/j.ajmms.20261605.95.
1. Introduction
- Thyroid nodular disease represents one of the most prevalent endocrine conditions worldwide, detectable by high-resolution ultrasonography in up to 67% of the adult population in iodine-deficient regions [1]. According to the World Health Organization, more than 200 million individuals globally suffer from some form of thyroid pathology, with the highest burden concentrated in Central and South Asian countries, where alimentary iodine deficiency remains an endemic challenge [2]. The Kashkadarya region of Uzbekistan, where the present study was conducted, is characterised by moderate iodine deficiency, translating into a consistently high demand for specialised thyroid surgical care at the regional endocrine surgery centre.Despite advances in thyroid imaging, cytopathology, and molecular diagnostics, the choice of surgical extent for benign thyroid nodular disease (BTND) remains one of the most debated topics in endocrine surgery. The fundamental clinical dilemma is well-established: total thyroidectomy (TT) virtually eliminates the risk of recurrence but commits every patient to life-long levothyroxine replacement therapy and carries the highest procedural risk for recurrent laryngeal nerve (RLN) palsy and hypoparathyroidism; conversely, organ-preserving resections (OPR) preserve thyroid function in a substantial proportion of patients but are associated with a 10-year goiter recurrence rate of 22–32% when the extent of resection is not guided by objective criteria [3,4].Current international guidelines from the American Thyroid Association (ATA, 2015), European Thyroid Association (ETA, 2023), and AACE/AME/ETA Joint Consensus (2020) provide qualitative frameworks for surgical decision-making but do not offer a formalised, quantitatively validated scoring instrument that integrates the full range of available pre-operative diagnostic data into a reproducible clinical decision tool [5–7]. This gap results in significant inter-surgeon and inter-institutional variability, with rates of total thyroidectomy for BTND ranging from 28% to 67% across published series a discrepancy that cannot be fully accounted for by differences in patient case-mix alone [8].Recent advances in thyroid functional imaging particularly colour Doppler flowmetry with resistive index (RI) quantification and strain/shear-wave sonoelastography provide objective surrogates for tissue vascularity and stiffness that correlate with functional reserve and malignant potential [9,10]. Intraoperative technologies, including continuous IONM of the RLN and fluorescence-guided parathyroid identification with indocyanine green or flowmetry, have demonstrated significant reductions in the rates of permanent nerve palsy and hypoparathyroidism in high-volume centres [11,12]. However, the integration of these diagnostic and intraoperative innovations into a unified, clinically actionable management pathway has not been systematically evaluated to date.The present study addresses this gap through the development, clinical validation, and prospective evaluation of an Integrated Risk Stratification Score (IRSS) combining eight pre-operative diagnostic criteria in a formal quantitative decision framework for BTND, complemented by a five-technology intraoperative innovation bundle. The primary hypothesis was that structured multi-parameter stratification combined with systematic intraoperative protective measures would simultaneously reduce early complications, long-term recurrence, and the burden of iatrogenic hypothyroidism while improving patient-reported quality of life.
2. Materials and Methods
- This was a retrospective-prospective, controlled comparative study conducted at the Kashkadarya Branch of the Republican Specialized Endocrinological Scientific-Practical Medical Centre (Karshi, Uzbekistan) from January 2019 to December 2025. The study was approved by the Institutional Review Board of Samarkand State Medical University (Protocol No. 14/2019) and conducted in accordance with the Declaration of Helsinki. All patients provided written informed consent.Inclusion criteria: (1) confirmed BTND (benign nodular goiter, follicular adenoma, or diffuse-nodular goiter on pre-operative assessment); (2) age ≥18 years; (3) scheduled for primary elective thyroid surgery; (4) absence of confirmed thyroid malignancy on pre-operative evaluation. Exclusion criteria: prior thyroid surgery, pregnancy, systemic malignancy, and inability to provide informed consent. A total of 163 eligible patients were enrolled: 88 in the study group (SG) managed according to the IRSS protocol (prospective arm, 2021–2025) and 75 in the control group (CG) receiving standard care (retrospective arm, 2019–2021). Both cohorts were balanced for age (46.9±1.9 vs 47.2±2.3 years; p=0.91), sex (females: 85.2% vs 84.0%; p=0.84), and principal diagnosis distribution (p>0.05 for all categories).
|
3. Results
- The IRSS composite achieved an AUC of 0.97 (95% CI: 0.94–0.99), sensitivity 95.1%, specificity 92.6%, positive predictive value 91.1%, and negative predictive value 96.2% significantly superior to standard ultrasound alone (AUC=0.71; p<0.001) and to each individual component (Table 2). Cytological concordance between pre-operative FNAB and final histopathology was 88.6% in SG vs 74.7% in CG (p<0.05), attributable to immunohistochemical adjudication of Bethesda III–IV categories, which enabled avoidance of total thyroidectomy in 55.6% of such patients with a normal IHC profile. The IRSS RI threshold (≥0.70) distinguished benign from potentially malignant nodules with a specificity of 84.0% (mean RI: 0.53±0.06 vs 0.74±0.08; p<0.001).
|
|
|
|
4. Discussion
- The central finding of this study is that an eight-criterion integrated scoring system achieves exceptional diagnostic accuracy (AUC=0.97) for guiding surgical volume selection in BTND a performance level that substantially surpasses any single diagnostic modality evaluated in the present cohort and compares favourably with the most comprehensive multi-modal algorithms reported in the recent literature [13,14]. The performance gap over standard ultrasound alone (ΔAUC=0.26; p<0.001) is of direct clinical significance: it translates into a measurable shift from predominantly radical to predominantly organ-preserving surgery, with a concomitant 10-fold reduction in lifelong hormone dependence and a 7.4-fold reduction in recurrence without any increase in complication risk.The role of pre-operative immunohistochemical adjudication warrants specific attention. In the present cohort, IHC reclassification of cytologically indeterminate nodules (Bethesda III–IV) enabled avoidance of total thyroidectomy in 55.6% of such patients, consistent with recently reported rates for Afirma Genomic Sequencing Classifier and ThyroSeq v3 molecular testing [15,16]. Critically, however, the IHC panel used here (Ki-67, Galectin-3, HBME-1, CK19) is widely available in standard pathology laboratories across Central Asia, making this approach practically deployable without access to high-cost next-generation sequencing platforms currently unavailable in the region.The integration of US flowmetry RI as a quantitative marker of nodule vascularity is another distinctive feature of the IRSS. An RI threshold of ≥0.70 demonstrated AUC=0.91 superior to conventional colour Doppler vascularity type grading and provided an objective, operator-independent correlate of malignant microangioarchitecture, consistent with the mechanistic data from earlier studies [17,18]. This finding supports formalisation of flowmetry RI as a mandatory component of pre-operative thyroid assessment in institutions evaluating surgical candidates.The intraoperative innovation bundle produced equally compelling results. The near-complete elimination of permanent RLN palsy (0% vs 2.7%) and permanent hypoparathyroidism (0% vs 2.7%) in SG is attributable to the combination of systematic anatomical identification and real-time monitoring: IONM enabled early detection of traction-induced amplitude loss in 3 cases, permitting immediate corrective manoeuvre and full signal recovery an outcome category not achievable with visual identification alone [19]. These findings are consistent with the meta-analytic evidence of Barczynski et al. (2020), reporting a 2–3-fold reduction in permanent palsy with systematic vs selective IONM implementation, and extend that literature to a regional surgical centre context [20]. The substantial reduction in operative time (21.9%) attributable to the modified retractor and lobe fixator reflects the direct ergonomic benefit of purpose-designed instrumentation an area underrepresented in the published thyroid surgery literature.The magnitude of improvement in patient-reported quality of life is noteworthy. The between-group difference in SF-36 total score (+13.2 points) exceeds the published minimal clinically important difference (MCID) for SF-36 of 5–10 points [21], indicating that the benefit is not merely statistically significant but experientially meaningful for patients. The normalisation of Spielberger anxiety scores to normative range in SG (28.8 vs clinical threshold of 30) vs persistent elevation in CG (40.8) underlines the psychological burden of unresolved symptoms, recurrence anxiety, and hormone dependence that accompanies inadequately individualised surgical care.Several limitations of the present study must be acknowledged. First, the retrospective-prospective design, though analytically controlled, precludes strict randomisation; residual confounding cannot be entirely excluded, though baseline group comparability was confirmed on all measured parameters. Second, follow-up was incomplete in 19.6% of patients, though loss-to-follow-up rates were comparable between groups. Third, the generalisability of the IHC-based adjudication to settings without established thyroid cytopathology laboratories may be limited. Fourth, the novel instrumentation (retractor and lobe fixator) requires prospective evaluation in a multi-centre setting to confirm the observed benefits.
5. Conclusions
- The Integrated Risk Stratification Score provides a reproducible, institution-independent, eight-criterion quantitative framework for individualised surgical decision-making in benign thyroid nodular disease. Its systematic application, complemented by a structured intraoperative innovation bundle, simultaneously reduces overall complications by 4-fold, eliminates permanent RLN palsy and permanent hypoparathyroidism, reduces goiter recurrence 7.4-fold, decreases lifelong hormone dependence 10-fold, and generates a clinically meaningful improvement in all patient-reported quality-of-life metrics. The IRSS represents a practical, cost-accessible tool for standardising thyroid surgical care across endocrine surgery units of varying resource levels. Multicentre prospective validation is warranted and is planned as the next phase of this research programme.