-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(5): 2717-2720
doi:10.5923/j.ajmms.20261605.94
Received: May 8, 2026; Accepted: May 25, 2026; Published: May 28, 2026

Comparative Analysis of the Outcomes of Combined Vagotomy and Simple Suturing in Perforated Duodenal Ulcer
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAbdullaev Khakimjon Makhmudjonovich1, Nuritdinov Orifjon Tolipovich2, Rakhmanov Bakhodirjon Jafaralievich3, Abdullaev Ulugbek Ubaydullaevich4
1Deputy Chief Physician for Surgical Affairs, Namangan Regional Multidisciplinary Medical Center, Namangan, Uzbekistan
2Doctor of Medical Sciences, Head of the 1st Department of Surgery, Clinic of Andijan State Medical Institute, Andijan, Uzbekistan
3Candidate of Medical Sciences, Clinic of Andijan State Medical Institute, Chief Physician, Andijan, Uzbekistan
4Candidate of Medical Sciences, Head of the Department of Clinical Sciences, Faculty of Medicine, Namangan State University, Namangan, Uzbekistan
Correspondence to: Abdullaev Khakimjon Makhmudjonovich, Deputy Chief Physician for Surgical Affairs, Namangan Regional Multidisciplinary Medical Center, Namangan, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The article presents a comparative analysis of the outcomes of combined vagotomy and simple suturing in patients with perforated duodenal ulcer. A total of 143 patients were included in the study, of whom 97 constituted the control group and 46 comprised the main group. In the control group, closure of the perforated ulcer was performed either by laparotomy or laparoscopic approach followed by eradication therapy. In the main group, combined vagotomy (anterior selective proximal vagotomy with posterior truncal vagotomy) together with excision of the perforated ulcer was carried out. During the study, the clinical course, postoperative condition, and risk of recurrence were evaluated. The obtained results demonstrated that combined vagotomy reduced gastric acid-peptic aggression, while excision of the ulcer, considered an antigenic stimulus, contributed to improved clinical outcomes and decreased the risk of recurrence. Combined vagotomy in perforated duodenal ulcer represents a pathogenetically substantiated and effective surgical treatment method.
Keywords: Perforated duodenal ulcer, Combined vagotomy, Simple ulcer suturing, Acid-peptic aggression, Ulcer recurrence
Cite this paper: Abdullaev Khakimjon Makhmudjonovich, Nuritdinov Orifjon Tolipovich, Rakhmanov Bakhodirjon Jafaralievich, Abdullaev Ulugbek Ubaydullaevich, Comparative Analysis of the Outcomes of Combined Vagotomy and Simple Suturing in Perforated Duodenal Ulcer, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2717-2720. doi: 10.5923/j.ajmms.20261605.94.
1. Introduction
- Perforated duodenal ulcer remains one of the most severe emergency conditions in abdominal surgery and is characterized by a high incidence of complications, peritonitis, and disease recurrence. The simple suturing technique, which is widely used in surgical practice, does not completely eliminate the ulcer regarded as an antigenic provoking factor, nor does it adequately address the pathogenetic mechanisms of the disease [12]. In recent years, combined vagotomy has been considered an effective surgical approach aimed at reducing gastric acid secretion and lowering the risk of ulcer recurrence [7].Severe destructive changes associated with perforated duodenal ulcers, including perforation, penetration, hemorrhage, and pancreatic complications, considerably complicate the choice of surgical tactics [11]. In particular, delayed hospitalization has been associated with a significant increase in the risk of peritonitis and postoperative complications [9]. Furthermore, early postoperative infectious complications and functional disorders adversely affect treatment outcomes [10].Although laparoscopic and minimally invasive surgical techniques are increasingly being implemented in modern abdominal surgery, comparative evaluation of the clinical effectiveness of various surgical approaches from the standpoint of evidence-based medicine remains highly relevant [6,13]. Some authors have also proposed conservative treatment strategies; however, the risks of infectious-inflammatory complications and recurrence remain high in cases of perforation [8].In this regard, a comparative analysis of the outcomes of combined vagotomy and simple suturing in perforated duodenal ulcer is of considerable scientific and practical importance, particularly in terms of reducing postoperative complications and preventing disease recurrence.Aim of the Study. To comparatively evaluate the outcomes of combined vagotomy and simple suturing in patients with perforated duodenal ulcer and to determine their effectiveness in reducing postoperative complications and disease recurrence.
2. Materials and Methods
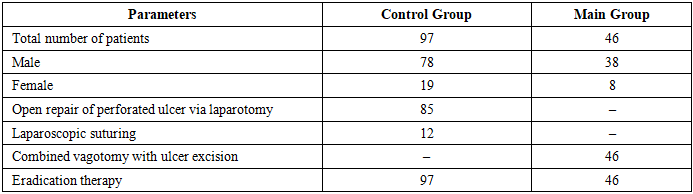
- The study was conducted based on the data of patients treated for perforated duodenal ulcer between 2020 and 2026. A total of 143 patients were analyzed. Of these, 97 patients comprised the control group, while 46 patients constituted the main group (Table 1).
|
|
3. Results
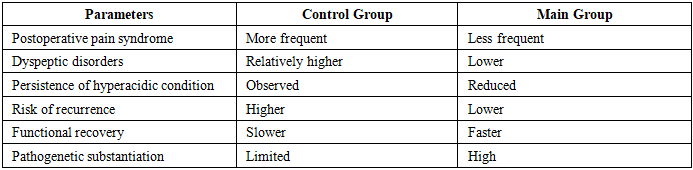
- During the study, the outcomes of surgical treatment in 143 patients with perforated duodenal ulcer were analyzed. In the control group, 97 patients underwent conventional ulcer suturing, whereas 46 patients in the main group underwent combined vagotomy with excision of the perforated ulcer. In the control group, inflammatory signs in the abdominal cavity, prolonged pain syndrome, and dyspeptic disorders were observed more frequently during the early postoperative period. In several patients, recurrent ulcer manifestations were recorded due to the persistence of a hyperacidic condition.In the main group, patients who underwent combined vagotomy demonstrated decreased gastric secretion, more rapid relief of pain syndrome, and earlier postoperative functional recovery. In patients with a vagotonic autonomic background, combined vagotomy proved to be an effective pathogenetically substantiated method.In patients with positive Helicobacter pylori status, combined vagotomy performed together with eradication therapy had a favorable effect on reducing the risk of ulcer recurrence.The average duration of surgery in the control group was 30–40 minutes, whereas in the main group it lasted 40–50 minutes due to the extended operative volume. Nevertheless, despite the relatively longer operative time, the main group demonstrated better clinical outcomes.The obtained results indicate that combined vagotomy with excision of the perforated ulcer is a pathogenetically justified and clinically effective surgical method for the treatment of perforated duodenal ulcer.
4. Discussion
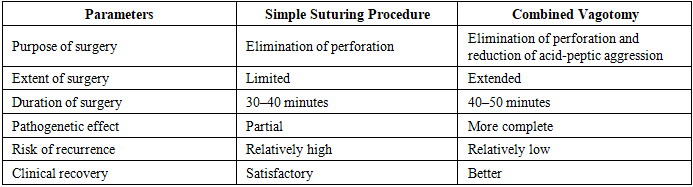
- Appropriate selection of surgical tactics in perforated duodenal ulcer is one of the key determinants of postoperative outcomes. In the present study, treatment outcomes of 143 patients were analyzed. The control group consisted of 97 patients, among whom 85 underwent open repair of perforated duodenal ulcer via laparotomy followed by eradication therapy, while 12 patients underwent laparoscopic closure with eradication therapy. The main group included 46 patients who underwent combined vagotomy together with excision of the perforated duodenal ulcer. Of these, 38 were males and 8 were females. The analysis demonstrated that although the conventional suturing procedure is technically simpler and can be performed within a shorter time, it is primarily aimed at eliminating perforation and does not fully affect the pathogenetic mechanisms of peptic ulcer disease. In particular, persistent hypersecretion of gastric acid, hyperfunction of the vagus nerve, and continued Helicobacter pylori infection increase the risk of recurrent ulcer formation. This issue is especially important in young and working-age patients when evaluating long-term outcomes.Although laparoscopic suturing has the advantage of being minimally invasive, this technique is mainly effective in patients admitted early and presenting with localized peritonitis. In cases of diffuse peritonitis, infiltrative changes, or severe inflammatory alterations around the ulcer, the laparoscopic approach may be technically limited.Combined vagotomy with excision of the perforated ulcer, applied in the main group, represents a pathogenetically substantiated surgical approach. Reduction of gastric secretion through vagotomy decreases acid-peptic aggression and thereby lowers the risk of ulcer recurrence. At the same time, excision of the ulcer area removes inflamed and morphologically altered tissues, creating favorable conditions for improved reparative processes in the postoperative period.The predominance of male patients in the main group confirms that perforated duodenal ulcer occurs more frequently in men. This may be explained by stress-related factors, dietary disturbances, smoking, and increased acid-peptic aggression.The obtained findings demonstrated that combined vagotomy with excision of the perforated ulcer is not only an effective emergency surgical intervention but also a pathogenetically justified procedure aimed at reducing disease recurrence (Table 3).
|
5. Conclusions
- Combined vagotomy with excision of the ulcer in perforated duodenal ulcer is a pathogenetically substantiated surgical approach. This method reduces gastric acid-peptic aggression, improves postoperative clinical outcomes, and decreases the risk of disease recurrence.