-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(5): 2712-2716
doi:10.5923/j.ajmms.20261605.93
Received: Apr. 29, 2026; Accepted: May 26, 2026; Published: May 28, 2026

Analysis of the Causes of Unsatisfactory Outcomes of Conventional Treatment Strategies for Gastroduodenal Bleeding in Patients with Severe Comorbid Pathology
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKaraboev Bekzodbek Bakhodirovich1, Khakimov Dilshodbek Mamadaliyevich2
1Associate Professor of the Department of General Surgery, Endosurgery, Pediatric Surgery, Anesthesiology and Resuscitation, and Pediatric Anesthesiology and Resuscitation, Faculty of Advanced Training and Retraining of Physicians, Andijan State Medical Institute, Andijan, Uzbekistan
2Doctor of Medical Sciences, Professor, Director of the Andijan Branch of the Republican Scientific Center for Emergency Medical Care, Andijan, Uzbekistan
Correspondence to: Karaboev Bekzodbek Bakhodirovich, Associate Professor of the Department of General Surgery, Endosurgery, Pediatric Surgery, Anesthesiology and Resuscitation, and Pediatric Anesthesiology and Resuscitation, Faculty of Advanced Training and Retraining of Physicians, Andijan State Medical Institute, Andijan, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

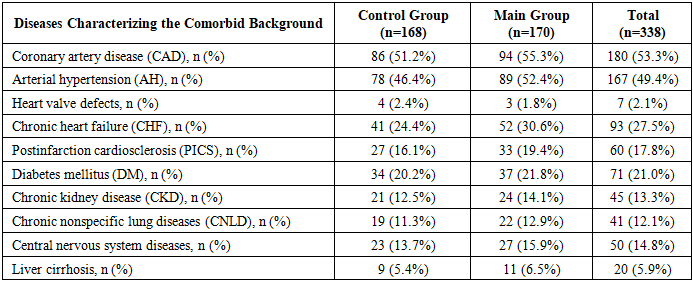
Non-variceal gastroduodenal bleeding (GDB) remains one of the most urgent challenges in emergency surgery due to the persistently high rates of recurrent hemorrhage and mortality, particularly among elderly patients. Conventional treatment approaches often fail to account for the systemic pathogenetic effects of concomitant diseases, resulting in hemostatic instability and unsatisfactory treatment outcomes. A retrospective and prospective analysis of treatment outcomes was conducted in 338 patients with ulcerative and erosive gastroduodenal bleeding. The primary focus of the study was the control group (n=168, 2017–2021), in which conventional diagnostic and therapeutic strategies were applied. Comorbid status was assessed using the Charlson Comorbidity Index. The study included a comprehensive evaluation of clinical, laboratory (including markers of endothelial dysfunction), and endoscopic parameters (Forrest classification). The examined cohort was predominantly represented by elderly patients (45.0%), with a mean age of 63.4±11.4 years. A high level of polymorbidity was identified, averaging 2.17 concomitant diseases per patient, with coronary artery disease (53.3%) and arterial hypertension (49.4%) being the most prevalent conditions. The mean Charlson Comorbidity Index score was 4.8±1.8 points, while 54.4% of patients demonstrated a pronounced or severe comorbid background (≥5 points). Analysis of outcomes in the control group revealed a correlation between the severity of concomitant pathology and the frequency of recurrent hemorrhage, associated with profound endothelial disturbances and morphological characteristics of the lesions (57.1% combined lesions). The conventional management strategy for patients with gastroduodenal bleeding, limited to local hemostatic measures without consideration of systemic endothelial dysfunction and the severity of comorbid conditions, does not provide reliable prevention of recurrent bleeding. A transition toward risk-oriented predictive models integrating vascular endothelial status indicators and individualized comorbidity profiles is required.
Keywords: Gastroduodenal bleeding, Comorbidity, Conventional treatment strategy, Recurrent bleeding, Mortality, Charlson Comorbidity Index, Endothelial dysfunction
Cite this paper: Karaboev Bekzodbek Bakhodirovich, Khakimov Dilshodbek Mamadaliyevich, Analysis of the Causes of Unsatisfactory Outcomes of Conventional Treatment Strategies for Gastroduodenal Bleeding in Patients with Severe Comorbid Pathology, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2712-2716. doi: 10.5923/j.ajmms.20261605.93.
1. Introduction
- The problem of providing effective medical care to patients with acute gastroduodenal bleeding (GDB) of ulcerative and erosive etiology has, at the present stage of abdominal surgery development, acquired the character of an interdisciplinary challenge [1,2]. Despite the widespread implementation of modern endoscopic technologies and highly effective antisecretory agents, the rate of unfavorable treatment outcomes remains consistently high, largely due to the qualitative transformation of the hospitalized patient population [3].The contemporary clinical profile of patients with GDB is characterized by a pronounced shift toward older age groups. According to the obtained data, elderly (60–74 years) and senile (≥75 years) patients collectively account for 60.0% of the total cohort, while the mean age reaches 63.4±11.4 years [4]. In this category of patients, hemorrhagic syndrome develops not as an isolated lesion of the gastrointestinal tract, but rather as a critical condition occurring against the background of pronounced polymorbidity [5]. The average number of concomitant diseases is 2.17 per patient, creating prerequisites for mutual aggravation of pathological processes.Conventional treatment strategies for GDB, primarily focused on local hemostasis and correction of volemic disturbances, are often ineffective precisely in comorbid patients [6]. The principal reason for the failure of traditional approaches is the neglect of systemic pathogenetic mechanisms determining hemostatic stability. In particular, the presence of coronary artery disease (53.3%), arterial hypertension (49.4%), and diabetes mellitus (21.0%) forms a pathological basis in the form of chronic endothelial dysfunction (ED) [7]. A severe comorbid background (Charlson Comorbidity Index ≥7 points in 16.8% of patients) is associated with an imbalance between vasoconstrictive factors (endothelin-1) and vasodilatory factors (nitric oxide), thereby preventing stable thrombus formation and slowing mucosal repair processes [8].One of the central unresolved issues in modern surgery remains the absence of a comprehensive predictive algorithm capable of identifying, at the stage of primary diagnosis, a high-risk group for recurrent bleeding among patients with concomitant pathology. Standard assessment according to the Forrest classification (Ia–III) provides only a static morphological characterization of the bleeding source at the time of examination [9]. However, in comorbid patients, ulcerative defects are frequently deep, involving destruction of major intramural vessels (ulcers penetrating into the muscular layer), which creates conditions for massive vascular erosion in 44.7% of cases. The situation is further complicated by the high prevalence of diffuse lesions: in 57.1% of patients, the pathological process involves two or more anatomical regions, making definitive hemostasis difficult to achieve using conventional methods.Thus, the conventional treatment strategy that has been employed in clinical practice for decades is approaching the limits of its effectiveness. Unsatisfactory outcomes (recurrent hemorrhage and in-hospital mortality) observed in the control group of patients (2017–2021) directly indicate the necessity for an in-depth investigation of the relationship between systemic manifestations of endothelial dysfunction and the local viability of the gastroduodenal mucosa. Without consideration of these factors, prediction of the clinical course of gastroduodenal bleeding remains subjective, while therapeutic interventions remain insufficiently personalized [10].The aim of the present study was to conduct a detailed investigation of the causes of unfavorable outcomes associated with conventional treatment strategies for gastroduodenal bleeding in patients with pronounced comorbid backgrounds, based on a retrospective assessment of clinical and endoscopic characteristics and an analysis of the role of systemic and local factors of endothelial dysfunction in the development of recurrent hemorrhage.
2. Materials and Methods
- The methodology of the present study was developed in accordance with the academic standards of evidence-based medicine for an in-depth analysis of the causes of unfavorable outcomes in the treatment of gastroduodenal bleeding (GDB). The study population consisted of 338 patients with ulcerative and erosive non-variceal gastroduodenal bleeding who underwent treatment at the Andijan Branch of the Republican Scientific Center for Emergency Medical Care between 2017 and 2026.The study included two principal stages. The first stage comprised a retrospective analysis of treatment outcomes in the control group (n=168, 2017–2021), in which conventional diagnostic and therapeutic strategies were applied. The primary objective of this stage was to identify the structure of unfavorable outcomes, including the incidence of recurrent hemorrhage and the causes of in-hospital mortality in comorbid patients.The second stage (prospective, 2022–2026) included the evaluation of 170 patients in the main group, in whom a newly developed risk-oriented management system was implemented. To obtain reference laboratory and endothelial parameters, a reference group (n=20) consisting of apparently healthy individuals was formed.Inclusion and Exclusion Criteria. To ensure a high degree of sample representativeness and scientific validity, strict selection criteria were established.Inclusion criteria:1. Patients aged 18 years and older. 2. Endoscopically verified source of gastroduodenal bleeding (ulcerative defects or erosive lesions of the gastric and duodenal mucosa). 3. Presence of confirmed comorbid pathology documented and assessed using the Charlson Comorbidity Index. 4. Availability of written informed consent from the patient or their relatives. Exclusion criteria:Variceal gastroduodenal bleeding associated with portal hypertension, oncological lesions of the gastrointestinal tract, traumatic injuries of the upper gastrointestinal tract, absence of comorbid pathology, and pregnancy.Characteristics of Patients in the Control Group (“Conventional Strategy”). The control group (n=168) served as the basis for analyzing the causes of unfavorable disease progression under standard treatment approaches. Males predominated in this group, accounting for 61.9% (n=104), with a male-to-female ratio of 1.63:1. The age profile of the group was characterized by the predominance of middle-aged patients (45–59 years) — 44.0%, and elderly patients (60–74 years) — 40.5%. The mean age of patients in the group was 61.7±10.6 years.Assessment of Comorbid Status. Comorbidity was defined as the presence of one or more chronic diseases capable of critically affecting hemostatic stability and the risk of recurrent bleeding. Quantitative and qualitative assessment was performed using the Charlson Comorbidity Index. In the control group, the structure of concomitant pathology was as follows (Table 1).
|
3. Results
- Clinical and Statistical Analysis of the Structure of Unfavorable Outcomes. During the retrospective analysis of treatment outcomes in the control group (n=168, 2017–2021), which received therapy according to conventional protocols, key factors determining the development of unfavorable outcomes were identified. The principal criterion of clinical destabilization was recurrent gastroduodenal bleeding (GDB), the incidence and complication profile of which were subjected to detailed analysis.It was established that the morphological characteristics of hemorrhagic sources in the studied patients were highly complex. Ulcerative lesions penetrating through the submucosal layer into the muscular layer of the organ were identified in 44.7% (n=151) of patients. Such depth of tissue destruction resulted in damage to major intramural vessels, manifesting as active spurting hemorrhage (Forrest Ia) in 3.3% of cases. Overall, signs of active bleeding (Forrest Ia and Ib) at the time of primary esophagogastroduodenofibroscopy (EGDFS) were documented in 24.0% (n=81) of patients.Particular significance in the structure of unfavorable outcomes was attributed to the extent of lesions. Combined forms of gastroduodenal involvement affecting two or more anatomical regions simultaneously were diagnosed in 57.1% (n=193) of observations. The diffuse nature of mucosal involvement (combined lesions of the antrum, gastric body, and duodenum) represented a statistically significant predictor of failure of single-session endoscopic hemostasis.Correlation Between Comorbid Background and the Risk of Hemorrhagic Complications. The analysis demonstrated a direct relationship between the severity of somatic status and the risk of recurrent hemorrhage. The mean integrated comorbidity score (Charlson Comorbidity Index) was 4.8±1.8 points. Distribution of patients according to comorbidity severity demonstrated the following results (Table 2).
|

4. Discussion
- Critical analysis of the obtained data suggests that the conventional management strategy for patients with ulcerative and erosive gastroduodenal bleeding demonstrates clear limitations in effectiveness when applied to comorbid patient populations. Unfavorable treatment outcomes observed in the control group (2017–2021) were determined by a combination of pathogenetic and tactical factors.First, the conventional model relies predominantly on the visual endoscopic characterization of the bleeding source according to the Forrest classification. However, in comorbid patients, the endoscopic picture is often misleading: hemostasis that appears stabilized at the time of examination (Forrest IIc–III, observed in 40.2% of patients) does not guarantee the absence of recurrence under conditions of pronounced endothelial dysfunction. The traditional approach failed to account for the imbalance between vasoconstrictive factors (endothelin-1) and vasodilatory factors (NOx), which impairs adequate vascular wall repair.Second, the diffuse nature of the lesions represents a major tactical challenge. The identification of combined lesion patterns in 57.1% of patients indicates that local hemostatic procedures (adrenaline injection, coagulation, or clipping of a single lesion) leave other compromised mucosal regions unprotected. In ulcers penetrating into the muscular layer (44.7% of cases), conventional injection hemostasis provides only temporary vascular compression without eliminating the underlying cause of vascular erosion under conditions of systemic ischemia and metabolic disturbances such as diabetes mellitus and chronic kidney disease.Third, the severity of surgical trauma associated with emergency operations performed at the stage of recurrent hemorrhage in patients with a mean Charlson Comorbidity Index of 4.6–5.1 points inevitably results in decompensation of concomitant diseases. The traditional strategy, based on reactive surgical intervention only after recurrence has already occurred, is frequently fatal for elderly patients (45.0% of the cohort) with coronary artery disease, postinfarction cardiosclerosis, and chronic heart failure.Therefore, the ineffectiveness of the conventional approach lies in its predominantly “local” orientation, whereas gastroduodenal bleeding in a comorbid patient represents a systemic pathological process. The development of an artificial intelligence–based predictive model incorporating assessment of endothelial status represents a pathogenetically justified step toward reducing the incidence of recurrent hemorrhage.
5. Conclusions
- 1. Conventional diagnostic and therapeutic strategies for gastroduodenal bleeding in comorbid patients are associated with a high probability of unfavorable outcomes due to the neglect of systemic risk factors, including endothelial dysfunction and severe polymorbidity (Charlson Comorbidity Index ≥5 points in 54.4% of patients). 2. The high prevalence of combined gastroduodenal lesions (57.1%) and the predominance of deep ulcerative defects (44.7%) penetrating into the muscular layer render local endoscopic hemostatic techniques insufficiently reliable without comprehensive systemic pathogenetic support. 3. Assessment of endothelin-1, nitric oxide metabolites, VEGF, and von Willebrand factor levels in peripheral blood and gastric lavage fluid is essential for objective prediction of recurrent hemorrhage in patients with cardiovascular and metabolic disorders. 4. Reduction in the incidence of recurrent bleeding and in-hospital mortality in this patient population is achievable only through the implementation of risk-oriented algorithms incorporating early endovascular interventions and automated artificial intelligence–based prognostic risk assessment.