-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(5): 2706-2711
doi:10.5923/j.ajmms.20261605.92
Received: Apr. 23, 2026; Accepted: May 23, 2026; Published: May 28, 2026

A Composite Biomarker Risk Stratification Model for Cardiorenal Syndrome Associated with Chronic Heart Failure
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLGadayev A. G.1, Turakulov R. I.1, Boboyev A. T.2, Khalilova F. A.3
1Tashkent Medical University, Tashkent, Uzbekistan
2Republican Specialized Scientific-Practical Medical Center of Hematology, Tashkent, Uzbekistan
3Bukhara State Medical Institute, Bukhara, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

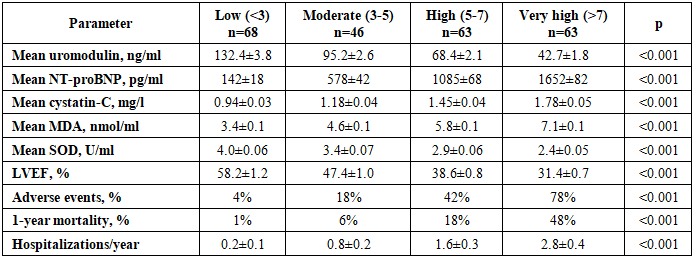
The article presents the development and validation of a composite biomarker risk stratification model for cardiorenal syndrome (CRS) associated with chronic heart failure (CHF). The study included 240 participants: Group 1 patients with CRS (n=100), Group 2 patients with CHF without CRS (n=100), Group 3 control (n=40). Five biomarkers (uromodulin, NT-proBNP, cystatin-C, MDA, SOD) were combined into a composite risk score (0-10 points). ROC analysis demonstrated that the individual biomarker AUCs ranged from 0.82 (SOD) to 0.91 (uromodulin), while the composite score achieved AUC=0.96 with 95% sensitivity and 91% specificity. Patients were stratified into four risk categories: low (<3), moderate (3-5), high (5-7), very high (>7). Adverse cardiac event rates increased from 4% in low-risk to 78% in very-high-risk category (p<0.001). The composite score >5 had OR=28.3 (95% CI 9.2-86.8) for CRS development. The proposed model demonstrates significantly higher prognostic accuracy than individual markers and is recommended for clinical implementation. The article presents 4 figures and 2 tables.
Keywords: Cardiorenal syndrome, Composite biomarker score, Risk stratification, ROC analysis, Prognostic model, Uromodulin, NT-proBNP, Cystatin-C, Multivariable analysis, Clinical decision support
Cite this paper: Gadayev A. G., Turakulov R. I., Boboyev A. T., Khalilova F. A., A Composite Biomarker Risk Stratification Model for Cardiorenal Syndrome Associated with Chronic Heart Failure, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2706-2711. doi: 10.5923/j.ajmms.20261605.92.
1. Introduction
- Cardiorenal syndrome (CRS) represents a complex pathophysiological entity characterized by bidirectional dysfunction between the heart and kidneys, where acute or chronic dysfunction of one organ leads to dysfunction of the other [1]. Patients with chronic heart failure (CHF) develop renal dysfunction in 30-50% of cases, which significantly worsens overall mortality and increases the risk of adverse cardiovascular events [2,3].Early identification and risk stratification of patients with CRS remains a major clinical challenge. Traditional approaches relying on individual biomarkers (creatinine, urea, BNP) have limited sensitivity and specificity, often detecting damage only after significant pathological changes have occurred [4]. The complexity of CRS pathogenesis, involving multiple interacting mechanisms neurohumoral activation, oxidative stress, tubulointerstitial damage, glomerular dysfunction, and microvascular impairment necessitates a multidimensional approach to risk assessment [5].Recent advances in molecular medicine have introduced novel biomarkers reflecting different aspects of CRS pathogenesis. Uromodulin (Tamm-Horsfall protein), synthesized in the thick ascending limb of Henle's loop and distal tubules, reflects tubular function and tubulointerstitial integrity [6,7]. NT-proBNP serves as a sensitive marker of cardiac hemodynamic burden and neurohumoral activation [8]. Cystatin-C provides accurate assessment of glomerular filtration, particularly in early stages of kidney dysfunction [9]. Malondialdehyde (MDA) reflects lipid peroxidation as a marker of oxidative stress, while superoxide dismutase (SOD) represents the antioxidant defense system [10].However, no single biomarker can comprehensively capture the multifaceted pathophysiology of CRS. The concept of composite biomarker scoring combining multiple biomarkers reflecting different pathogenetic pathways has emerged as a promising approach for improved risk stratification [11]. Such composite models have demonstrated superior diagnostic and prognostic performance compared to individual biomarkers in various cardiovascular conditions [12].Despite the theoretical advantages of composite scoring, no validated model specifically tailored for CRS in CHF patients exists in current clinical practice. The development of such a model could significantly improve early identification of high-risk patients, enable personalized therapeutic approaches, and potentially reduce mortality through timely intervention.The aim of this study was to develop and validate a composite biomarker risk stratification model for CRS associated with CHF, integrating uromodulin, NT-proBNP, cystatin-C, MDA, and SOD into a unified prognostic scoring system, and to assess its discriminatory performance compared to individual biomarkers.
2. Materials and Methods
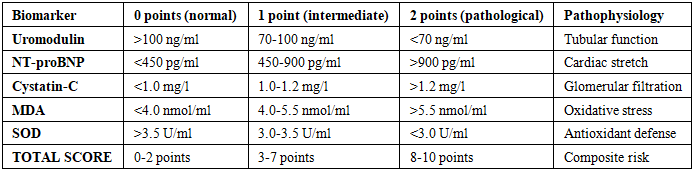
- Study design and population. A prospective, controlled, comparative cohort study was conducted between 2022-2025 at the clinical bases of Abu Ali Ibn Sino Bukhara State Medical Institute. The study enrolled 240 participants distributed into three groups: Group 1 (main) patients with CRS developed against the background of CHF (n=100, mean age 62.4±1.2 years, males 42.0%, females 58.0%); Group 2 (comparison) patients with CHF without renal dysfunction (n=100, mean age 61.1±0.9 years); Group 3 (control) healthy volunteers (n=40, mean age 44.2±1.1 years).Inclusion criteria: confirmed CHF based on coronary heart disease and/or hypertension, with corresponding renal dysfunction (eGFR <60 ml/min/1.73 m² for Group 1). Exclusion criteria: acute myocardial infarction, unstable angina, severe arrhythmias, advanced chronic kidney disease (stage V), autoimmune diseases, oncological conditions.Biomarker assessment. Uromodulin and cystatin-C were measured in serum by enzyme-linked immunosorbent assay (ELISA) using Snibe Maglumi 800 (China) instrument. NT-proBNP was determined by immunochemiluminescent assay. MDA was measured by thiobarbituric acid reaction at 532 nm wavelength. SOD activity was assessed using the standard spectrophotometric method based on inhibition of superoxide radical reaction. Serum creatinine was measured by the kinetic Jaffe method.Cardiac and renal imaging. Echocardiography was performed using PHILIPS Affiniti 70 (USA) device to evaluate left ventricular ejection fraction (LVEF), end-systolic diameter (ESD), end-diastolic diameter (EDD), and E/A ratio. Renal artery Doppler ultrasonography assessed peak systolic velocity (Vps), end-diastolic velocity (Ved), resistive index (RI), and pulsatility index (PI). UMOD gene rs4293393 A/G polymorphism was determined by PCR-RFLP method.Composite risk score development. Five biomarkers were selected for inclusion based on their pathophysiological relevance and individual diagnostic performance. Each biomarker was scored 0-2 points based on tertile distribution: 0 points (normal), 1 point (intermediate), 2 points (pathological). The total composite score ranged from 0 to 10 points. Cut-off values: uromodulin >100/70-100/<70 ng/ml; NT-proBNP <450/450-900/>900 pg/ml; cystatin-C <1.0/1.0-1.2/>1.2 mg/l; MDA <4.0/4.0-5.5/>5.5 nmol/ml; SOD >3.5/3.0-3.5/<3.0 U/ml.Statistical analysis. SPSS 25.0 (IBM, USA) and Python 3.10 with scikit-learn 1.4 were used. The discriminatory performance was evaluated using ROC analysis with Area Under Curve (AUC), sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV). Multivariable logistic regression was performed with calculation of odds ratios (OR) and 95% confidence intervals (CI). Risk categories were established based on score distribution: low risk (<3), moderate (3-5), high (5-7), very high (>7). Statistical significance was set at p<0.05.
3. Results and Discussion
- 1. Diagnostic performance of individual biomarkers and composite scoreThe discriminatory performance of individual biomarkers and the composite score for CRS diagnosis was assessed using ROC analysis (Figure 1).
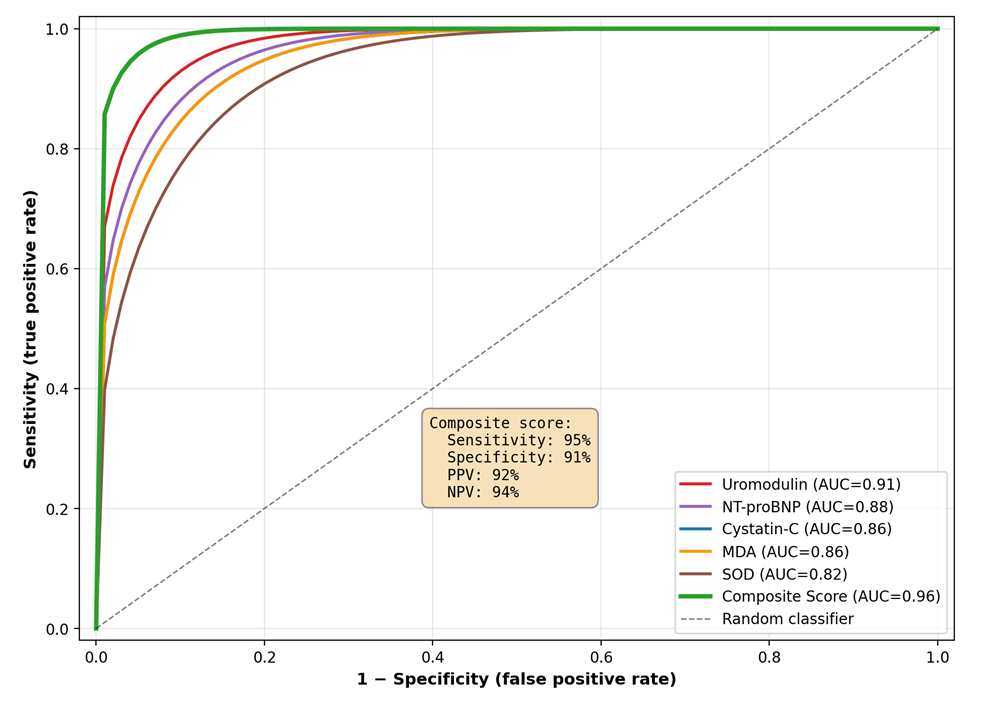 | Figure 1. ROC analysis of individual biomarkers and the composite score for cardiorenal syndrome diagnosis. AUC values for individual biomarkers ranged from 0.82 (SOD) to 0.91 (uromodulin), while the composite score achieved AUC=0.96 |
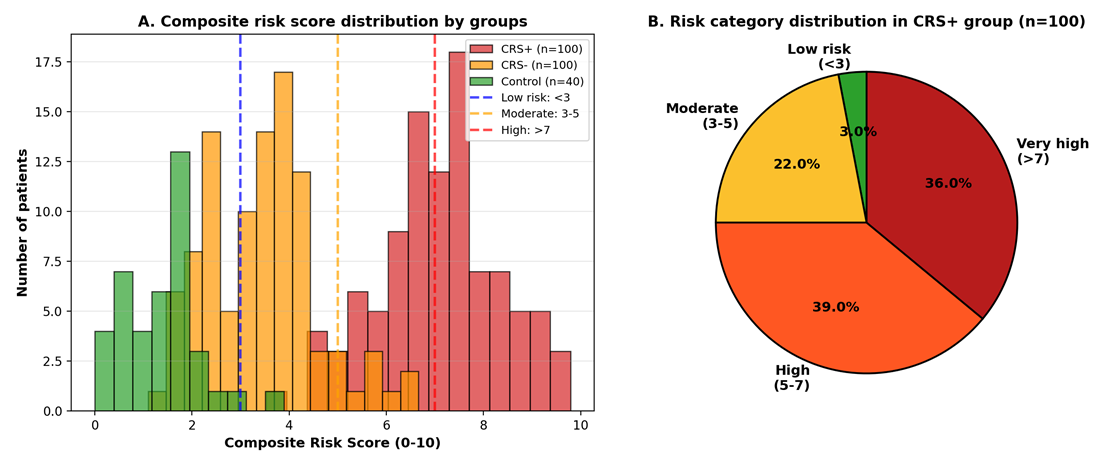 | Figure 2. Composite biomarker risk score: A — distribution of risk scores across study groups; B — risk category distribution in CRS+ group (n=100). Cut-off values: low risk (<3), moderate (3-5), high (5-7), very high (>7) |
|
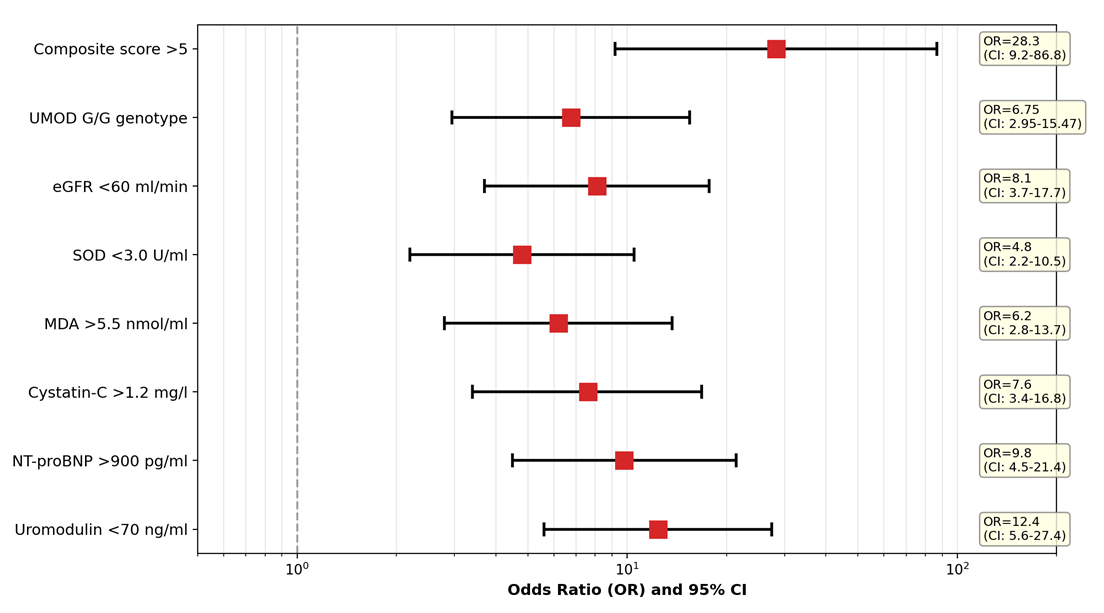 | Figure 3. Forest plot of odds ratios for individual biomarker abnormalities and the composite score >5 for cardiorenal syndrome diagnosis (univariate logistic regression analysis) |
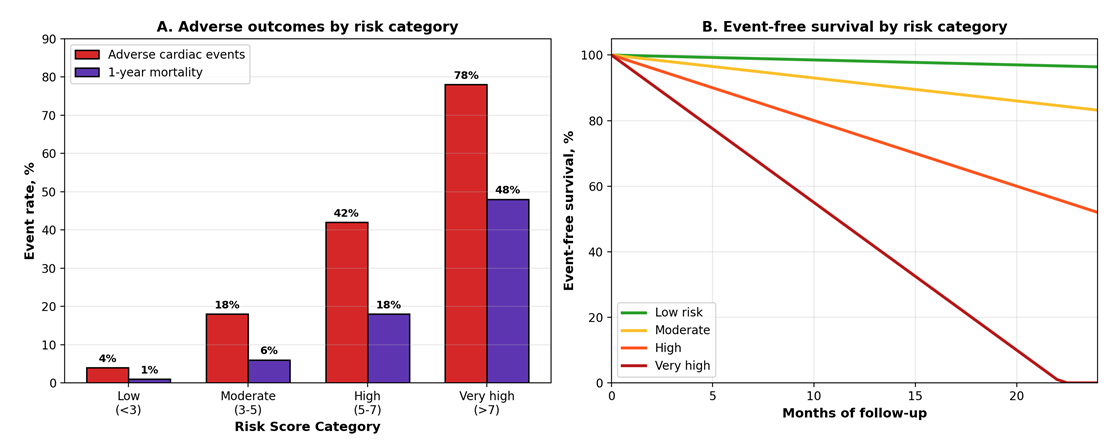 | Figure 4. Clinical outcomes stratified by composite biomarker risk score: A — adverse cardiac event rates and 1-year mortality across risk categories; B — event-free survival curves over 24 months follow-up |
|
4. Conclusions
- 1. The composite biomarker risk score combining uromodulin, NT-proBNP, cystatin-C, MDA, and SOD demonstrates significantly superior diagnostic performance (AUC=0.96, sensitivity 95%, specificity 91%) compared to individual biomarkers (AUC range 0.82-0.91) for cardiorenal syndrome.2. The four-tier risk stratification model (low <3, moderate 3-5, high 5-7, very high >7) effectively differentiates patient prognosis: 75% of CRS+ patients fall into high or very-high risk categories, while virtually 0% of controls do, validating the discriminatory power of the model.3. Composite score >5 demonstrates substantial association with CRS risk (OR=28.3; 95% CI 9.2-86.8; p<0.001), significantly outperforming individual biomarker abnormalities (OR range 4.8-12.4). This reflects the synergistic effect of multiple pathophysiological pathway abnormalities.4. Clinical outcomes show a clear graded relationship with risk categories: adverse cardiac event rates progressively increase from 4% (low risk) to 78% (very high risk), and 1-year mortality from 1% to 48% (p<0.001 for trend), confirming strong prognostic utility.5. The composite score integrates five complementary aspects of CRS pathogenesis — tubular function, neurohumoral activation, glomerular filtration, oxidative stress, and antioxidant defense — providing a comprehensive assessment that captures the multifactorial nature of cardiorenal interaction.6. The proposed model uses only routine laboratory tests, employs simple 0-10 point scoring, and provides robust risk stratification, making it suitable for clinical implementation. Multi-center external validation studies are warranted before widespread clinical adoption.