-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(5): 2698-2702
doi:10.5923/j.ajmms.20261605.90
Received: Apr. 27, 2026; Accepted: May 19, 2026; Published: May 27, 2026

Age-Dependent Renal Pathomorphological Alterations in Patients with Cerebrovascular Diseases
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAbdullayev Nodirbek Uroyimjonovich1, Narbayev Zafar Kamilovich2
1Lecturer, Impuls Medical Institute, Namangan, Uzbekistan
2Candidate of Medical Sciences, Department of Otolaryngology, Andijan State Medical Institute, Andijan, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This study explores age-associated pathomorphological changes in renal tissue in patients who died from cerebrovascular diseases (CVD). The analysis was based on autopsy materials from 81 cases collected between 2022 and 2024, with diagnoses confirmed through clinical and morphological data. Histological examination using hematoxylin–eosin staining, along with immunohistochemical and morphometric methods, was performed to assess structural alterations in kidney tissue. The results demonstrated that renal changes, including arteriolosclerosis, glomerulosclerosis, interstitial fibrosis, and tubular atrophy, were observed across all cases. No significant sex-related differences were identified, indicating that these alterations occur independently of gender. However, a strong association was found between the severity of renal damage and increasing age, with the highest prevalence observed in patients aged 53–85 years. Additionally, comorbid conditions such as arterial hypertension, type 2 diabetes mellitus, and atherosclerosis played a crucial role in exacerbating renal pathology. These findings highlight the importance of age and systemic vascular disorders in the development of renal complications in CVD and emphasize the need for early detection and integrated clinical management.
Keywords: Cerebrovascular diseases, Kidney pathology, Age-related changes, Glomerulosclerosis, Hypertension, Diabetes mellitus, Morphometry
Cite this paper: Abdullayev Nodirbek Uroyimjonovich, Narbayev Zafar Kamilovich, Age-Dependent Renal Pathomorphological Alterations in Patients with Cerebrovascular Diseases, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2698-2702. doi: 10.5923/j.ajmms.20261605.90.
Article Outline
1. Introduction
- Cerebrovascular diseases (CVD), including ischemic and hemorrhagic stroke, remain among the leading causes of mortality and long-term disability worldwide [2]. Beyond their primary impact on the central nervous system, these disorders are increasingly recognized as manifestations of systemic vascular pathology. In this context, multiple organs particularly the kidneys are affected due to shared microvascular and hemodynamic mechanisms. The kidney, characterized by a dense microvascular network and high metabolic demand, is especially susceptible to ischemic and hypoxic injury under conditions of impaired cerebral and systemic circulation [5].The concept of the brain–kidney axis has gained attention in recent years, emphasizing the bidirectional relationship between cerebrovascular and renal dysfunction. Acute cerebrovascular events can lead to systemic hemodynamic instability, endothelial dysfunction, and inflammatory responses, all of which may contribute to acute or chronic kidney injury. Conversely, pre-existing renal impairment is known to increase the risk of cerebrovascular complications, creating a vicious cycle of progressive organ damage.Age is a critical factor influencing both cerebrovascular and renal pathology. Structural and functional changes in the aging kidney include nephron loss, glomerulosclerosis, vascular wall thickening, and interstitial fibrosis. These alterations reduce the adaptive capacity of renal tissue to withstand ischemic stress. At the same time, age-related vascular changes such as arterial stiffness, endothelial dysfunction, and reduced autoregulatory capacity further exacerbate both cerebral and renal injury. As a result, older individuals are at significantly higher risk of developing combined cerebrovascular and renal pathology.In addition to aging, several comorbid conditions play a central role in the development and progression of renal damage in patients with CVD. Arterial hypertension contributes to arteriolar hyalinosis and nephrosclerosis, while diabetes mellitus induces glomerular basement membrane thickening and mesangial expansion. Atherosclerosis leads to narrowing of renal arteries and chronic ischemia, further aggravating tissue damage. These conditions often coexist, amplifying their deleterious effects on both the brain and kidneys.Despite growing recognition of the interconnection between cerebrovascular and renal diseases, the pathomorphological features of renal involvement in CVD, particularly in relation to age, remain insufficiently characterized. Most existing studies focus on clinical or functional parameters, whereas detailed histological and morphometric analyses are relatively limited.Therefore, the present study aims to investigate the morphofunctional and morphometric changes in renal tissue in patients with cerebrovascular diseases and to determine their age-related characteristics. By integrating histological, immunohistochemical, and morphometric approaches, this research seeks to provide a more comprehensive understanding of renal pathology in CVD and its dependence on age and associated risk factors.
2. Materials and Methods
2.1. Study Design and Sample
- This study was designed as a retrospective descriptive morphological investigation based on autopsy materials. The research was carried out at the Republican Pathological Anatomy Center using specimens collected between 2022 and 2024. A total of 81 autopsy cases were included in the analysis.Inclusion criteria comprised cases with a confirmed diagnosis of cerebrovascular disease (CVD), established through clinical records and postmortem morphological findings, including ischemic infarction, hemorrhagic stroke, cerebral edema, and brainstem injury. Only cases with adequately preserved renal tissue suitable for histological and immunohistochemical examination were selected.Exclusion criteria included cases with severe postmortem autolysis, incomplete clinical data, or pre-existing advanced renal diseases unrelated to vascular pathology that could confound the interpretation of results. All procedures were conducted in accordance with ethical standards for the use of autopsy materials in biomedical research.
2.2. Data Collection
- Clinical and laboratory data were obtained retrospectively from medical records and autopsy protocols. The collected information included patient demographics, primary diagnosis, comorbid conditions, and duration of hospitalization prior to death.For analytical purposes, cases were stratified into the following categories:Sex: male and femaleDuration of hospitalization: categorized into four groups (0–1 day, 2–3 days, 4–7 days, and 8–15 days)
|
2.3. Histological and Immunohistochemical Analysis
- Renal tissue samples were collected during autopsy and fixed in 10% neutral buffered formalin, followed by routine processing, paraffin embedding, and sectioning at 3–5 μm thickness.Histological ExaminationSections were stained with hematoxylin and eosin (H&E) to assess general histoarchitecture and identify key pathological features, including:Glomerular changes (e.g., sclerosis, collapse)Vascular alterations (arteriolosclerosis, hyalinosis)Tubular damage (atrophy, degeneration)Interstitial changes (fibrosis, inflammatory infiltration)Immunohistochemical (IHC) AnalysisImmunohistochemical staining was performed to evaluate cellular activity and extracellular matrix remodeling. Specific markers (e.g., α-SMA for myofibroblast activation and fibrosis, TGF-β1 for fibrogenic signaling) were used to identify:Fibrotic processesVascular remodelingCellular proliferation and injuryVisualization was achieved using standard chromogenic detection methods, and stained sections were analyzed under light microscopy.Histomorphometric AnalysisQuantitative assessment of renal structures was conducted using histomorphometric techniques. The relative proportions of key renal components—glomeruli, tubules, interstitium, and blood vessels—were measured using image analysis software. This allowed objective evaluation of structural alterations and comparison across age groups.
2.4. Statistical Analysis
- Data were processed using descriptive statistical methods. Absolute numbers and percentages were calculated for categorical variables, including sex distribution, age groups, and hospitalization duration.Comparative analysis between groups was performed using frequency distribution tables to identify patterns and trends. The results were presented in the form of tables and diagrams to facilitate interpretation. Although inferential statistical tests were not the primary focus of this study, observed differences were interpreted in the context of clinical and morphological relevance.These morphological features collectively indicate chronic ischemic nephropathy and are consistent with long-standing vascular insufficiency. The severity of these changes generally increased with age and was more pronounced in patients with multiple comorbidities.In addition, immunohistochemical analysis supported the presence of fibrogenic activity and vascular remodeling, further confirming the progressive nature of renal damage in CVD.
3. Results
3.1. Sex Distribution
- Among the 81 analyzed cases, 41 patients (50.6%) were male and 40 patients (49.4%) were female, indicating an almost equal distribution between sexes. The minimal difference (1 case) suggests that sex does not play a determining role in the development of renal pathomorphological changes in patients with cerebrovascular diseases (CVD).From a clinical–morphological perspective, this finding implies that the mechanisms underlying renal damage in CVD are likely related to systemic vascular and metabolic factors rather than sex-specific biological differences. Therefore, in the context of this study, sex can be considered a neutral variable, although it may still interact with other factors such as age, hormonal status, and comorbidities in more complex analyses.
3.2. Hospitalization Duration
- Analysis of hospitalization duration revealed that the majority of patients experienced short hospital stays, with 53.1% of cases occurring within the first 3 days of admission. The largest subgroup consisted of patients hospitalized for 2–3 days (29.6%), followed by those hospitalized for 0–1 day (23.5%), 4–7 days (25.9%), and 8–15 days (21.0%).These findings suggest that many patients were admitted in a severe or critical condition, leading to rapid clinical deterioration and early mortality. The high proportion of deaths within the first 72 hours reflects the acute and aggressive course of cerebrovascular events, often complicated by systemic dysfunction, including renal impairment.Patients who survived longer (4–15 days) may have initially responded to treatment but subsequently developed secondary complications, such as multi-organ failure, acute kidney injury, or thromboembolic events. Overall, the data emphasize the importance of early diagnosis, timely hospitalization, and intensive care management in improving patient outcomes.
3.3. Age Distribution
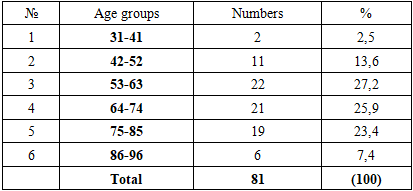
- The age distribution demonstrated a clear predominance of cases among middle-aged and elderly individuals. The highest frequencies were observed in the following groups:53–63 years: 27.2% (22 cases)64–74 years: 25.9% (21 cases)75–85 years: 23.4% (19 cases)Combined, these age groups accounted for 76.5% of all cases, indicating that renal pathomorphological changes associated with CVD are most prevalent in individuals aged 53–85 years.In contrast, younger age groups (31–52 years) represented a relatively small proportion (16.1%), suggesting that severe combined cerebrovascular and renal pathology is less common in early adulthood. However, when present, such cases may indicate underlying severe systemic or genetic predispositions.The lower frequency observed in the oldest group (86–96 years, 7.4%) may reflect selection bias, survival characteristics, or underdiagnosis of renal pathology in very elderly individuals.Overall, the results highlight the strong association between aging and the progression of both cerebrovascular and renal pathology, likely due to cumulative vascular damage, reduced regenerative capacity, and increased prevalence of comorbid conditions.
3.4. Morphological Findings
- ConditionsHistological and morphometric examination of renal tissue revealed several consistent structural alterations indicative of chronic and progressive injury. The most frequently observed changes included:Arteriolosclerosis: Thickening and hyalinization of small arterial walls, leading to luminal narrowing and reduced perfusionGlomerulosclerosis: Partial or global sclerosis of glomeruli, reflecting chronic ischemic and metabolic injuryInterstitial fibrosis: Expansion of fibrous connective tissue within the interstitium, associated with chronic inflammation and hypoxiaTubular atrophy: Degeneration and shrinkage of renal tubules, often accompanied by loss of epithelial cellsThese morphological features collectively indicate chronic ischemic nephropathy and are consistent with long-standing vascular insufficiency. The severity of these changes generally increased with age and was more pronounced in patients with multiple comorbidities.In addition, immunohistochemical analysis supported the presence of fibrogenic activity and vascular remodeling, further confirming the progressive nature of renal damage in CVD.
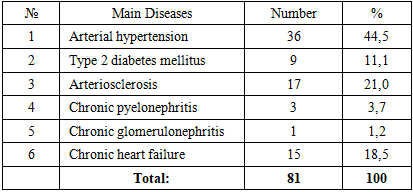
3.5. Associated Comorbidities
|
4. Discussion
- The present study provides further evidence that renal pathomorphological alterations in patients with cerebrovascular diseases (CVD) are primarily driven by age-related and systemic vascular factors, rather than sex-specific differences. The nearly equal distribution between male and female cases supports previous epidemiological findings indicating that sex does not significantly influence the structural renal response to cerebrovascular pathology[1]. Instead, the development of renal lesions appears to depend more on the cumulative burden of vascular risk factors and aging processes.A key finding of this study is the predominance of cases within the 53–85-year age range, which reflects the progressive nature of both cerebrovascular and renal diseases. Aging is associated with structural and functional changes in the vascular system, including arterial stiffness, endothelial dysfunction, and impaired autoregulation, all of which contribute to reduced organ perfusion. In the kidneys, these changes manifest as nephron loss, glomerulosclerosis, and interstitial fibrosis, ultimately leading to decreased functional reserve [4]. The observed age-related increase in renal damage highlights the importance of considering aging as a central determinant in the pathogenesis of combined brain–kidney pathology.The relatively short duration of hospitalization observed in a large proportion of cases suggests that many patients were admitted in advanced or critical condition, often with rapidly progressing disease. This finding may reflect delayed recognition of symptoms, inadequate early intervention, or limited access to timely medical care. The high early mortality rate underscores the aggressive course of cerebrovascular events when accompanied by systemic complications, including renal dysfunction. It also emphasizes the need for improved early detection, rapid diagnostic protocols, and intensive management strategies in acute care settings.Morphologically, the predominant findings—arteriolosclerosis, glomerulosclerosis, interstitial fibrosis, and tubular atrophy—are characteristic of chronic ischemic and hypertensive renal injury. These features are consistent with previously described patterns in hypertensive nephropathy and diabetic kidney disease[3]. The presence of these changes in patients with CVD supports the concept that renal damage in this context is not an isolated phenomenon but rather part of a systemic microvascular disease process. Chronic hypoperfusion, oxidative stress, and inflammatory signaling likely play key roles in mediating these structural alterations.Comorbid conditions such as arterial hypertension, type 2 diabetes mellitus, and atherosclerosis were highly prevalent among the studied cases and appear to be central contributors to both cerebrovascular and renal pathology. These diseases share common pathogenic mechanisms, including endothelial injury, vascular remodeling, and impaired autoregulation of blood flow. As a result, they create a shared pathophysiological pathway linking the brain and kidneys, often described as the “vascular continuum.” The coexistence of these conditions accelerates the progression of organ damage and worsens clinical outcomes.Overall, the findings of this study support the concept of a multifactorial and systemic origin of renal pathology in CVD. Age-related vascular changes, combined with chronic comorbidities, lead to progressive renal impairment that parallels cerebrovascular damage. This underscores the importance of a holistic, interdisciplinary approach in both research and clinical management, focusing on the early identification and control of vascular risk factors.
5. Conclusions
- The results of this study demonstrate that renal pathomorphological changes in cerebrovascular diseases are a significant component of systemic vascular pathology and are influenced by multiple interrelated factors.First, these changes occur independently of sex, indicating that gender does not play a major role in determining the structural response of renal tissue in the context of CVD.Second, a strong association was identified between renal pathology and age, with the highest prevalence observed in individuals aged 53–85 years. This finding highlights the critical role of aging in promoting vascular and renal degeneration, as well as reducing the adaptive capacity of organs to ischemic stress.Third, the development and progression of renal alterations are closely linked to comorbid conditions, particularly arterial hypertension, diabetes mellitus, and atherosclerosis. These diseases contribute to vascular damage, chronic ischemia, and fibrotic remodeling of renal tissue, thereby exacerbating pathological changes.Taken together, the observed morphological features—such as glomerulosclerosis, interstitial fibrosis, and tubular atrophy—reflect underlying systemic vascular injury and chronic hypoxic processes affecting the kidneys.From a clinical perspective, these findings emphasize the need for:Early screening and monitoring of renal function in patients at risk of cerebrovascular diseasesComprehensive management of vascular risk factors, including blood pressure control, glycemic regulation, and lipid managementPreventive strategies targeting middle-aged and elderly populations, aimed at reducing the incidence and severity of both cerebrovascular and renal complicationsIn conclusion, the study highlights the importance of recognizing renal involvement as an integral component of cerebrovascular disease and supports the implementation of integrated, multidisciplinary approaches to improve patient outcomes and reduce mortality.