Ilkhamdjan A. Karimdzhanov1, Lola K. Rakhmanova2, Umida N. Karimova3, Shakhodat D. Matkarimova4
1MD, DSc, PhD, Professor, Head of the Department of Children’s Diseases in Family Medicine, Tashkent State Medical University, Tashkent, Uzbekistan
2MD, DSc, PhD, Professor, Department of Children’s Diseases in Family Medicine, Tashkent State Medical University, Tashkent, Uzbekistan
3MD, PhD, Professor, Department of Children’s Diseases in Family Medicine, Tashkent State Medical University, Tashkent, Uzbekistan
4Assistant, Department of Pediatrics and Higher Nursing, Urgench State Medical Institute, Urgench, Uzbekistan
Correspondence to: Ilkhamdjan A. Karimdzhanov, MD, DSc, PhD, Professor, Head of the Department of Children’s Diseases in Family Medicine, Tashkent State Medical University, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
Background. In children, nephrotic syndrome associated with acute glomerulonephritis may be accompanied by immune dysregulation, complement activation and recurrent complications, particularly under adverse environmental conditions. This study aimed to assess the effectiveness of immunocorrection in the early prevention of complications of nephrotic syndrome in children living in the Aral Sea region. Materials and Methods. Sixty children aged 3–14 years with acute glomerulonephritis and nephrotic syndrome were examined. Group I included 30 patients living in Tashkent, and group II included 30 patients living in the Aral Sea region. The control group consisted of 30 practically healthy age-matched children. Serum interleukin-2 (IL-2), interleukin-4 (IL-4), and complement components C3 and C4 were assessed. In group II, azoximer bromide (Polyoxidonium) was added to complex therapy at a dose of 0.15 mg/kg/day parenterally for 5–10 days. Results. Children from the Aral Sea region had a more severe clinical profile, with higher rates of edema, ascites, hepatomegaly, pallor, fatigue, appetite loss and concomitant conditions. IL-2 and IL-4 levels were increased in both patient groups compared with controls and were highest in group II. Complement components C3 and C4 were significantly reduced, with the most pronounced hypocomplementemia in group II. After immunocorrection, follow-up assessment after 3–6 months showed a significant decrease in IL-2 and IL-4 and an increase in C3 and C4 compared with children receiving conventional therapy. Relapse of acute glomerulonephritis with nephrotic syndrome occurred in 3 of 30 children (10.0%) during 6 months of follow-up. Conclusions. In children living in the Aral Sea region, acute glomerulonephritis with nephrotic syndrome is characterized by frequent relapses, hyperproduction of IL-2 and IL-4, and hypocomplementemia involving C3 and C4. The inclusion of azoximer bromide in complex therapy may improve immunological parameters and support the prevention of secondary immunodeficiency-related complications.
Keywords:
Immunocorrection, Nephrotic syndrome, Acute glomerulonephritis, Complement, Cytokines, Aral Sea region
Cite this paper: Ilkhamdjan A. Karimdzhanov, Lola K. Rakhmanova, Umida N. Karimova, Shakhodat D. Matkarimova, Immunocorrection in Children with Nephrotic Syndrome in the Aral Sea Region, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2680-2684. doi: 10.5923/j.ajmms.20261605.86.
1. Introduction
In recent decades, a steady increase has been observed in the incidence of glomerulopathies in children with nephrotic syndrome (NS) [1–3]. At the same time, early prevention, pathogenetic approaches and adequate treatment of urinary system disorders caused by autoimmune processes remain insufficiently developed in the pediatric population. As a result, chronicity and mortality associated with these diseases remain high.Chronic renal failure as a cause of disability in children is registered in 5 per 100,000 children, whereas the risk of developing end-stage chronic renal failure by the age of 20 years may reach 68.0% [4,5]. The formation and progression of chronic kidney diseases in children are often characterized by latent impairment of individual renal functions, with subsequent involvement of the tubules and interstitium [6–12]. This tendency requires increased attention to nephrotic syndrome in children with diseases influenced by environmental factors, including those living in the Aral Sea region. These problems are related to global challenges of modern medicine, including secondary immunodeficiency, allergic diseases and metabolic disorders. The ecological crisis zone of the Aral Sea directly includes Turkmenistan, Kazakhstan and Uzbekistan and indirectly affects Tajikistan and Kyrgyzstan [13,14]. Environmental problems in the Aral Sea region have a particularly negative impact on population health, especially on mothers and children [15–17].The above considerations indicate that studying the clinical and immunological features of nephrotic syndrome in children living in the Aral Sea region, as well as improving immunocorrection approaches, remain urgent tasks of modern pediatrics and pediatric nephrology.The aim of the study was to substantiate the effectiveness of immunocorrection in the early prevention of complications of nephrotic syndrome in children living in the Aral Sea region.
2. Materials and Methods
The study included 60 children aged 3–14 years with acute glomerulonephritis (AGN) and nephrotic syndrome. The patients were divided into two groups: group I included 30 patients with AGN and NS living in Tashkent, and group II included 30 patients with AGN and NS living in the Aral Sea region. The control group consisted of 30 practically healthy age-matched children.The clinical diagnosis was established on the basis of medical history, clinical examination, laboratory tests and functional diagnostic methods. The serum levels of interleukin-2 (IL-2) and interleukin-4 (IL-4) [18], as well as complement components C3 and C4 [19], were assessed in all patients.For the purpose of immunocorrection, azoximer bromide (Polyoxidonium; NPO PETROVAX PHARM, state registration No. B-250-95 No. 33801) was included in the complex therapy of patients in group II. The drug was administered parenterally at a dose of 0.15 mg/kg body weight per day for 5–10 days. No complications were observed after administration. Treatment effectiveness was evaluated using clinical and immunological parameters.Venous blood collected in the morning after overnight fasting served as the study material. Quantitative data were processed using methods of variation statistics with assessment of the significance of numerical differences using Student's t-test.
3. Results and Discussion
Based on the results of the studies, it was revealed that of the observed patients, 35.0% were girls and 65.0% were boys. When assessing the clinical manifestations of NS in the examined children (groups I and II), a tendency was found to a statistically significantly higher frequency of the following symptoms in group II compared to group I: oliguria (91.0%-100.0%), edema (45.8%-85.6%), hematuria (88.8%-65.2%), arterial hypertension (79.8%-71.2%), azotemia (53.8%-64.2%), pale skin (65.8%-81.2%), fatigue (55.3%-79.1%), decreased appetite (78.1%-84.0%), positive percussion symptom (65.0%-71.5%), ascites (35.1%-58.4%), hepatomegaly (31.8%-58.0%), respectively (p<0.001-0.01).The underlying disease was statistically significantly associated with several concomitant conditions (p < 0.01). The most frequent comorbidities were anemia (87.0% in group I and 100.0% in group II), chronic tonsillitis (77.0% - 86.0%), thyroid dysfunction (24.9% - 45.0%), recurrent bronchitis (9.6% - 14.0%), adenoids (4.6% - 18.1%), and polyvalent allergy (15.9% - 35.4%), respectively (Fig. 1). 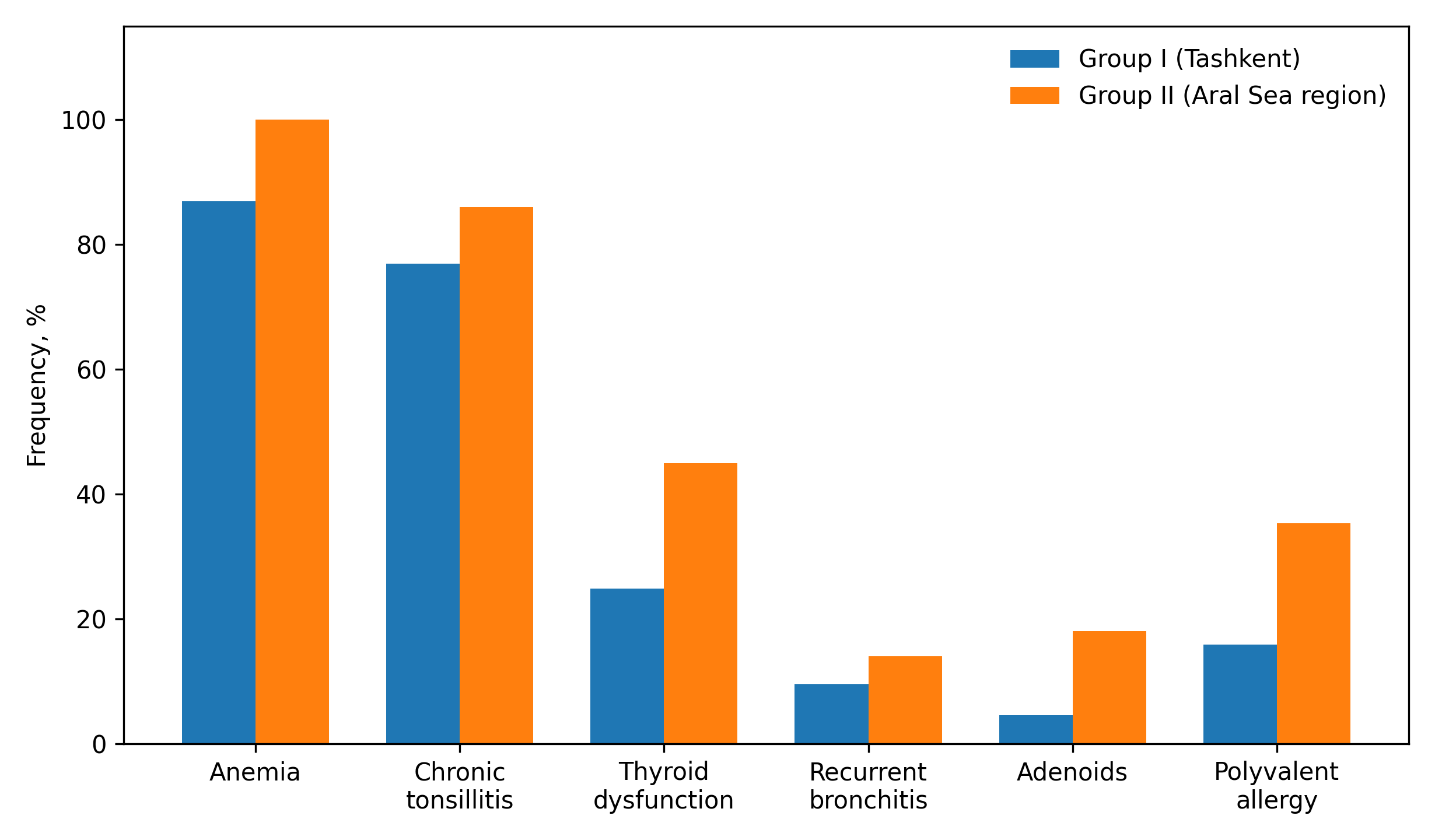 | Figure 1. Concomitant conditions in the examined children. Group I: children with AGN and NS living in Tashkent; group II: children with AGN and NS living in the Aral Sea region |
Assessment of individual renal function parameters revealed a decrease in daily diuresis and relative urine density (p < 0.001), as well as an increase in daily erythrocyturia and leukocyturia (p < 0.001–0.01). A statistically significant increase was also observed in daily proteinuria and in serum urea and creatinine concentrations (p < 0.001–0.01). Intergroup comparison showed that impairment of renal functional activity was more pronounced in group II than in group I. Cytokine status also differed between the groups (Fig. 2). IL-2 production was significantly increased in both patient groups compared with the control group (p < 0.001). In group II, IL-2 levels were significantly higher than in group I (p < 0.001). IL-4 production was also significantly higher in all patient groups than in the control group (p < 0.001). In children from group II, IL-4 levels were significantly higher than in group I (p < 0.001–0.01).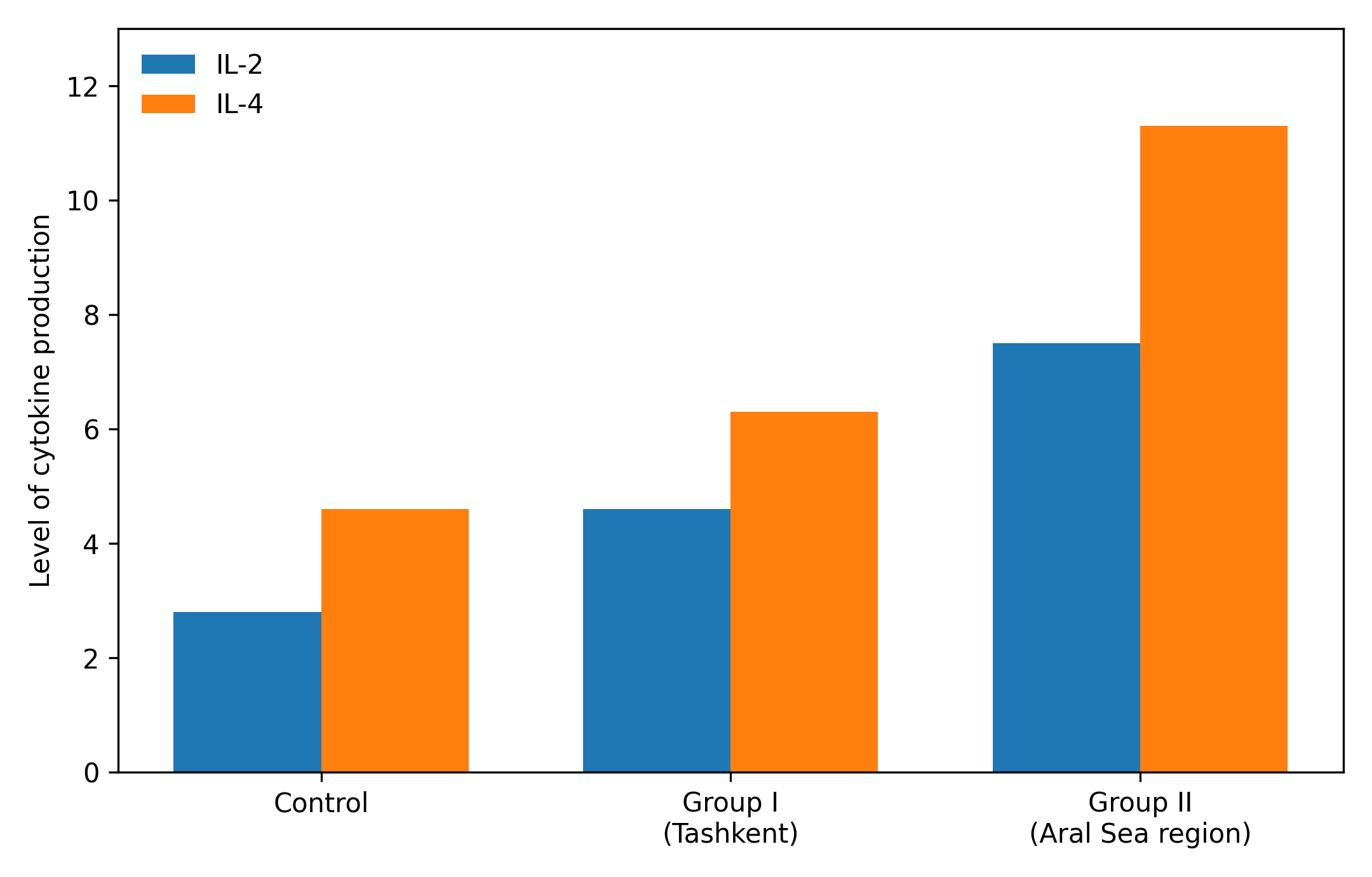 | Figure 2. IL-2 and IL-4 production levels in the examined children |
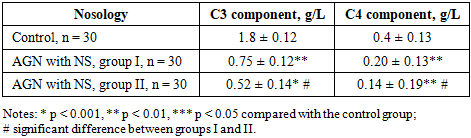
Complement components C3 and C4 were assessed in the examined children (Table 1).Table 1. Levels of C3 and C4 complement components in the examined children, M ± m
 |
| |
|
Comparative evaluation of immunological parameters showed a significant decrease in C3 and C4 levels compared with the control group (p < 0.001–0.01). The decrease was more pronounced in group II; C3 and C4 levels were approximately 1.5-fold lower than in group I (p < 0.001–0.01).Before discharge, patients in group II received Polyoxidonium as part of complex therapy, whereas group I received conventional therapy. After immunocorrection, dynamic assessment after 3–6 months showed improvement in immunological parameters in patients treated with Polyoxidonium, manifested by a significant decrease in IL-2 and IL-4 (p < 0.001) and an increase in C3 and C4 complement components (p < 0.001–0.01) compared with children who received conventional therapy.During 6 months of follow-up, exacerbation of AGN with NS was observed in 3 of 30 patients (10.0%). A decrease in the frequency of intercurrent diseases, including tonsillitis, acute respiratory viral infections, bronchitis and allergy, was also noted. These conditions are clinically important because they may contribute to exacerbation of AGN with NS. Normalization of peripheral blood and urine parameters was observed, including hemoglobin level, leukocyte count, erythrocyte sedimentation rate, proteinuria, erythrocyturia, leukocyturia and daily diuresis, together with prolongation of the clinical remission period.The findings indicate that children with AGN and NS living in the Aral Sea region had a more pronounced clinical and immunological burden than children living in Tashkent. The higher frequency of edema, ascites, hepatomegaly, pallor, fatigue, reduced appetite and concomitant disorders suggests a more complicated disease course in group II.The observed increase in IL-2 and IL-4 supports the role of cytokine imbalance in the pathogenesis of nephrotic syndrome in children. IL-2 stimulates the synthesis of several cytokines, including IL-4. Important properties of IL-2 include protection of activated T cells from apoptosis and participation in the regulation of immunological tolerance. Through autocrine effects on Th1 cells and paracrine effects on the Th2-cell subpopulation, IL-2 influences the Th1/Th2 balance, stimulates the cytotoxic activity of CD8 lymphocytes and contributes to the formation of T-cell populations [20].Based on the obtained results, the cytokine imbalance between Th1 and Th2 responses may determine the direction of immune response impairment. Dysregulated production of pro- and anti-inflammatory cytokines may have pathogenetic significance in uncontrolled inflammation and autoimmune pathology. IL-2 and IL-4 favor the formation of Th2 cells that produce IL-4, which may promote immediate-type hypersensitivity involving IgE [21].The complement system also appears to be involved in the immunopathogenesis of AGN with NS. C3 is a key component of defense against infection and participates in both the classical pathway, which is activated by IgG and IgM, and the alternative pathway, which may be activated by toxins, endotoxins and IgA. Activation of C3 contributes to histamine release from mast cells and platelets, leukocyte chemotaxis, antibody-antigen interactions, phagocytosis, increased vascular permeability and smooth muscle contraction.C4 participates mainly in the classical pathway of complement activation. It supports phagocytosis, increases vascular wall permeability and participates in viral neutralization. Complement activation is finely regulated in the body; when this regulation is disturbed, glomerular lesions may be characterized by dense intramembranous deposits, which are diagnosed by electron microscopy [22,23].The present results suggest that dysregulation of the alternative complement pathway plays an important role in both C3 glomerulopathy and immune complex-mediated glomerular diseases. Therefore, in children with AGN and NS, membranoproliferative glomerulonephritis may develop within the spectrum of C3 glomerulopathy, together with reduced serum C3 and C4 levels.Thus, the results of the conducted immunological studies confirm that the body's immune system is closely linked to the function of IL-2, IL-4 and C3, C4 components of complement, which play an important role in the mechanism of immune defense, manifested in the form of antigen-structural homeostasis, carrying out specific processes of immunological reactivity.The improvement observed after immunocorrection may be associated with the immunotropic effects of azoximer bromide. Polyoxidonium is described as a high-molecular-weight physiologically active compound with pronounced immunotropic activity. It interacts with the surface membranes of neutrophils, monocytes and lymphocytes. By its mechanism of action, Polyoxidonium is considered an immunomodulator with a complex and multifaceted influence on the immune system. It may restore impaired immune functions without affecting normal immune responses and acts primarily on innate immune cells, including neutrophils, monocytes/macrophages and natural killer cells [24]. The study has several limitations. The sample size was relatively small, the treatment comparison was not randomized, and follow-up lasted 6 months. Therefore, the findings should be interpreted as preliminary and require confirmation in larger controlled studies with longer follow-up and standardized assessment of renal outcomes.
4. Conclusions
1. In children living in the Aral Sea region, acute glomerulonephritis with nephrotic syndrome is characterized by frequent relapses and a more pronounced immunodeficiency state, manifested by hyperproduction of IL-2 and IL-4 and hypocomplementemia involving C3 and C4 complement components.2. The high therapeutic effectiveness observed during treatment with Polyoxidonium and the absence of treatment-related complications allow it to be considered for use as part of complex therapy and prevention of secondary immunodeficiency in children with acute glomerulonephritis and nephrotic syndrome living in the Aral Sea region.
References
| [1] | Rakhmanova LK, Karimova UN, Sadikova NB. Assessment of the combination of quantitative and qualitative signs in nephrotic syndrome in children with atopic dermatitis. Medical Science of Uzbekistan. 2025; (2): 80-82. |
| [2] | World Health Organization, United Nations Children’s Fund, International Council for the Control of Iodine Deficiency Disorders. Assessment of iodine deficiency disorders and monitoring their elimination. 3rd ed. Geneva: WHO; 2007. |
| [3] | Karimdzhanov IA, Rakhmanova LK, Karimova UN, Yaxyayeva KZ, Akhmedova NA, Rakhmanov AA. Immunopathological prediction of complications of nephropathy in children due to allergy. Child’s Health. 2025; 20(5): 34-37. |
| [4] | Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2024 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int. 2024; 105(4S): S117-S314. |
| [5] | Rodriguez-Iturbe B, Haas M. Post-streptococcal glomerulonephritis. In: Ferretti JJ, Stevens DL, Fischetti VA, editors. Streptococcus pyogenes: Basic biology to clinical manifestations. Oklahoma City (OK): University of Oklahoma Health Sciences Center; 2016. |
| [6] | Kari JA, Bamagai A, Jalalah SM. Severe acute post-streptococcal glomerulonephritis in an infant. Saudi J Kidney Dis Transpl. 2013; 24(3): 546-548. doi: 10.4103/1319-2442.111061. |
| [7] | Bakr A, Mahmoud LA, Al-Chenawi F, et al. HLA-DRB1* alleles in Egyptian children with post-streptococcal acute glomerulonephritis. Pediatr Nephrol. 2007; 22(3): 376-379. doi: 10.1007/s00467-006-0324-y. |
| [8] | Raxmanova LK, Karimova UN, Israilova NA, Yax’yaeva KZ. Peculiarities of immunity in nephrotic syndrome in children with COVID-19 against the atopic background. Turkish Journal of Physiotherapy and Rehabilitation. 2021; 32(2): 4391-4394. |
| [9] | Sharmin M, Chowdhury AM, Ali MA, et al. Clinical profile and immediate outcome of children admitted with acute glomerulonephritis in Pediatrics Department of a tertiary level hospital. Mymensingh Med J. 2020; 29(1): 5-15. |
| [10] | Skrzypczyk P, Ofiara A, Zacharzewska A, et al. Acute post-streptococcal glomerulonephritis — immune-mediated acute kidney injury: case report and literature review. Cent Eur J Immunol. 2021; 46(4): 516-523. doi: 10.5114/ceji.2021.112244. |
| [11] | Hunt EAK, Somers MJG. Infection-related glomerulonephritis. Pediatr Clin North Am. 2019; 66(1): 59-72. doi: 10.1016/j.pcl.2018.08.005. |
| [12] | Syridou G, Drikos I, Vintila A, et al. Influenza A H1N1-associated acute glomerulonephritis in an adolescent. IDCases. 2019; 19: e00659. doi: 10.1016/j.idcr.2019.e00659. |
| [13] | Ziyadullaev NS, Aimbetov NK, Trostyansky DV. The tragedy and salvation of the Aral Sea: the task of world and regional powers. Economy of Central Asia. 2025; 9(3): 217-240. doi: 10.18334/asia.9.3.123706. |
| [14] | Mirziyoyev ShM. The President of Uzbekistan addressed the 78th session of the UN General Assembly. President.uz. Available from: https: //president.uz. |
| [15] | Kosbergenova GK. Physical development characteristics of children living in the Aral Sea region with chronic respiratory diseases. Theory and Practice of Modern Science. 2020; 11(65): 254-256. |
| [16] | Zonn IS, Glyants MKh. Aral Encyclopedia. Moscow: International Relations; 2008. 250 p. |
| [17] | Fayzullaeva KA. Problems of the ecological crisis of the Aral Sea and its impact on public health. Agricultural Sciences and Agro-Industrial Complex at the Turn of the Century. 2013; (1): 1-5. |
| [18] | Aripova TU, Umarova AA, Petrova TA. Normative indicators of the main parameters of the immune system in children according to age: methodological recommendations. Tashkent; 2004. |
| [19] | Zhiznevskaya II, Khmelevskaya IG. Prognostic criteria for chronicity of glomerulopathies in childhood. Fundamental Research. 2012; 2(7): 319-323. |
| [20] | Rakhmanov AM, Rakhmanova LK, Matkarimov ShD. Modern features of the pathogenesis, epidemiology and clinical course of acute glomerulonephritis in children. International Journal of Scientific Pediatrics. 2026; 5(2): 1255-1264. doi: 10.56121/2181-2926-2026-5-2-1255-1264. |
| [21] | Liu Q, Ding JL. The molecular mechanisms of TLR-signaling cooperation in cytokine regulation. Immunol Cell Biol. 2016; 94(6): 538-542. |
| [22] | Kambham N. Postinfectious glomerulonephritis. Adv Anat Pathol. 2012; 19(5): 338-347. |
| [23] | Serdobintsev KV. The complement system: pathology, diagnostics, treatment. Allergology and Immunology in Pediatrics. 2016; (3): 33-40. |
| [24] | Mukhomedzyanova LV, Andrianova IV, Vakhrushev SG. Dynamics of functional indices of the palatine tonsils in patients with chronic tonsillitis during conservative treatment. Russian Otolaryngology. 2004; (4): 135-138. |
| [25] | Karimdjanov I. A., Rаkhmаnоvа L. K., Matkаrimоvа Sh. D. Modern Aspects of the Course of Acute Glomerulonephritis in Children. American Journal of Medicine and Medical Sciences 2026, 16(3): 998-1007. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML