Nurboboyev Adkhambek Uygun ugli, Safoyev Baqodir Barnoyevich, Boltayev Timur Shavkatovich
Bukhara State Medical Institute, Bukhara, Uzbekistan
Correspondence to: Nurboboyev Adkhambek Uygun ugli, Bukhara State Medical Institute, Bukhara, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
Infected limb wounds represent not only a medical but also a significant socio-economic problem. Long treatment periods, the need for repeated surgical interventions, prolonged antibacterial therapy, and rehabilitation lead to an increase in healthcare system costs. The aim of this study was to improve the treatment results of patients with purulent surgical diseases of the soft tissues of the upper and lower extremities by applying hyperventilation of wounds with oxygen flow. Research materials and methods. The examination and treatment data of 122 patients with purulent diseases of the limbs were analyzed, of whom 68 patients were included in the I comparison group, who were treated using the traditional treatment method. Group II included 54 patients; during the treatment of this group of patients, in addition to the traditional treatment method, wound hyperventilation with oxygen flow was performed. Results. When using this developed methodology, the indicators of the main criteria for assessing and dynamics of the wound process were: late clearing of infection from the wound (as early as the 2nd day of treatment), the onset of granulation by the 4th day of treatment, and the onset of epithelialization by the 6th day of treatment, indicating the effectiveness of this treatment method. The biochemical indicators of wound exudate normalize by the 5th day of treatment. Wound tissue RO2 indicators on the day of admission in patients of the main group were also below normal. At the same time, the average treatment duration for patients in the comparison group was 6.5±0.5 days. Conclusion. Taking into account the results of the comparative analysis, an optimal method for treating patients with purulent wounds of the soft tissues of the limbs was developed using wound hyperventilation with oxygen flow.
Keywords:
Wound, Purulent diseases of soft tissues, Oxygen hyperventilation, Tissue PO2
Cite this paper: Nurboboyev Adkhambek Uygun ugli, Safoyev Baqodir Barnoyevich, Boltayev Timur Shavkatovich, Efficiency of Using Oxygen Stream Hyperventilation in the Treatment of Patients with Infected Extermity Injuries, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2665-2671. doi: 10.5923/j.ajmms.20261605.84.
1. Introduction
Infected wounds of the limbs represent not only a medical but also a significant socio-economic problem. Long-term treatment, the need for repeated surgical interventions, prolonged antibacterial therapy, and rehabilitation lead to an increase in healthcare system costs. Furthermore, the high risk of developing severe complications, including flegmonas, osteomyelitis, sepsis, and limb amputations, leads to significant mortality and disability among patients of working age [3,6,8].In this regard, one of the promising areas of modern medicine is the development and implementation of methods aimed at increasing tissue oxygenation in the area of the wound defect. In clinical practice, hyperbaric oxygenation has become the most widespread, allowing for a significant increase in oxygen content in blood and tissues [2,5]. However, this method has a number of significant limitations: high equipment costs, the need for specialized pressure chambers, limited availability, as well as the risk of developing side effects associated with the systemic effects of increased oxygen pressure [1].An important advantage of wound hyperventilation with oxygen flow is its relative simplicity, accessibility, and economic efficiency [9]. Unlike hyperbaric oxygenation, this method does not require complex equipment and can be implemented in the conditions of various medical institutions, including general hospitals and outpatient services. This makes it particularly in demand in healthcare systems with limited resources [4,7].Thus, the method of hyperventilation of wounds with oxygen flow meets modern clinical medicine requirements aimed at increasing the efficiency, safety, and accessibility of treating infected limb wounds. Its implementation into clinical practice can contribute to reducing complications, shortening treatment and hospitalization periods, reducing the need for radical surgical interventions, including amputations, and improving functional and cosmetic treatment outcomes.The aim of this study was to improve the treatment results of patients with purulent surgical diseases of the soft tissues of the upper and lower extremities by applying hyperventilation of wounds with oxygen flow.
2. Research Materials and Methods
The examination and treatment data of 122 patients with purulent diseases of the extremities were analyzed, of whom 68 patients with purulent diseases of the soft tissues of the upper and lower extremities without diabetes who were treated in the surgery department of the Bukhara Regional Multidisciplinary Medical Center and the Bukhara City Medical Association in 2020-2024 were included in the I comparison group. These patients were treated using a traditional treatment method that included local sanation of wounds with an antiseptic solution of 25% dimexide, necrectomy, water-soluble ointment under an aseptic dressing, general detoxification therapy, and mandatory endovascular diagnostics and treatment.The II - main group of our study included 48 patients with severe forms of purulent diseases of the soft tissues of the upper and lower extremities without diabetes who were undergoing treatment in the department surgery of the Bukhara Regional Multidisciplinary Medical Center and the Bukhara City Medical Association 2025-2026 In the treatment of this group of patients, in addition to the traditional treatment method, wound hyperventilation with oxygen flow was performed (Table 1).Table 1. Distribution of patients by type of treatment (n=122)
 |
| |
|
On the day of admission, all examined patients underwent objective, subjective, general clinical, and instrumental examinations to accurately clarify the diagnosis and assess the patients' somatic condition.Device and methodology for applying wound hyperventilation.To address these tasks, we utilized a device invented in our clinic for hyperoxygenation of wounds with oxygen flows as part of the complex treatment of purulent-necrotic limb wounds.After adhering to the main principles of treating purulent wounds, such as opening the purulent focus, reviewing and sanitizing the purulent cavity with antiseptic solutions, and if necessary, performing necrectomy, as a local treatment for purulent-necrotically affected limbs, the next stage of treatment is transitioned using the proposed device.To assess the oxygen saturation of wound tissues, the partial oxygen pressure (PO2) of wound tissues was determined using a transcutaneous oxygen monitor from the "Radiometer" company (Denmark), consisting of an electrode, a monitor, and a power supply unit. Transcutaneous measurement of PO2 is a direct polarographic measurement using an electrode electrochemical circuit consisting of a modified Clark oxygen electrode, a heating element, and a temperature sensor.The objective assessment of the course of general and local manifestations of the wound process was conducted according to subjective indicators (character of wound discharge, infiltrate absorption, condition of wound edges, characteristics of granulation tissue development and epithelialization) and objective signs (body temperature, general clinical blood analysis, leukocyte index of intoxication, concentration of medium-molecular-weight peptides in blood serum, pH of wound discharge, calculation of PC according to M.F. Mazurik, percentage of reduction in wound surface area, wound healing rate, bacteriological and cytological studies).
3. Results and Their Discussions
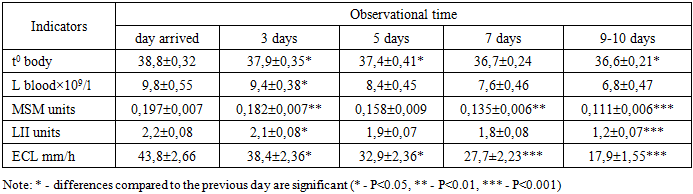
Group I included 68 patients with purulent diseases of the soft tissues of the upper and lower extremities. Of these, 37 (54.4%) patients had purulent wounds of the upper limbs, and 31 (45.6%) patients had purulent wounds of the lower limbs. Of the 68 examined patients in this group, 40 (58.8%) were admitted to the clinic with various purulent soft tissue diseases, and 28 (41.2%) patients were admitted with extensive purulent wounds of various etiologies that had already been admitted from other medical hospitals or outpatient clinics in the first phase of the wound process.All 40 patients admitted with various purulent diseases of the soft tissues of the limbs underwent an opening of the purulent focus and sanation of the wound process on the day of admission. Subsequent treatment tactics were identical to those for patients with incoming purulent wounds, which included daily treatment of the wound with antiseptics and application of Levomekol ointment and 25% dimexide solution under an aseptic dressing.It should be noted that the subsequent treatment tactics for patients with both postoperative purulent wounds and purulent soft tissue diseases were identical.Analysis of the body intoxication indicators in patients with purulent soft tissue diseases in comparison group I revealed the following changes (Table 2). As seen from the table, on the first day of treatment, the body temperature of patients averaged 38.8 ± 0.320°C. The leukocyte content in the blood was 9.8 ± 0.55 × 109/L. The volume of average molecules averaged 0.197 0.007 units. Similarly, an increase in LII and ESR was noted.Table 2. Dynamics of intoxication indicators in patients with purulent soft tissue diseases I - comparison group (n=68)
 |
| |
|
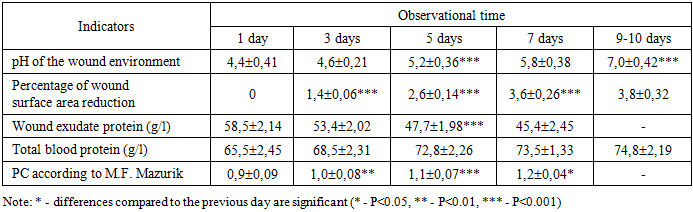
By the seventh day of treatment, although these figures had a downward trend, they remained above the norm.Upon further treatment and observation, by the tenth day, all analyzed intoxication indicators, except for blood ESR, were within the normal range.The next criteria for assessing the dynamics of the wound process in patients were the pH of the wound environment, the percentage of reduction in the wound surface area, and PC indicators according to M.F. Mazurik (Table 3). In the analyzed group of patients, on the first day of inpatient treatment, the initial pH level of the wound environment was significantly lower (acidosis) and averaged 4.4±0.41. Wound exudate protein averaged 58.5±2.14 g/l. At the same time, PC averaged 0.9±0.09 units.Table 3. Dynamics of biochemical indicators and wound healing rate in patients of comparison group I (n=68)
 |
| |
|
By the seventh day, the wound area was 1.2±0.04, and the wound area significantly decreased by 3.6±0.26% per day. The pH of the wound medium averaged 5.8±0.38. Only by the tenth day of treatment did the pH of the wound medium become neutral. The reduction in wound surface area per day was 3.8±0.32%. The secretion of exudate from the wound has ceased, which, in our opinion, is due to the transition of the wound process from phase 1 to phase 2.To assess the oxygen saturation of wound tissues, the partial oxygen pressure (PO2) of the wound tissues was determined. Its methodology is described in detail in Chapter II of the dissertation.The indicators provided in Table 4 indicate that if the RO2 of wound tissues on the day of admission was 18.8 and 0.4 mm Hg, it increased to 20.8 and 0.2 mm Hg on the 3rd day, which is 2.0 mm Hg higher than on the day of admission. By the fifth day of traditional treatment, oxygen tension in the wound tissues increased to 24.6 ± 0.2 mm Hg, and by the seventh day, these figures reached 26.4 ± 0.6 mm Hg. With further treatment, by the 10th day, the RO2 of the tissue wound was still below normal levels and amounted to 28.8 ± 0.3 mm Hg.Table 4. Dynamics of RO2 indicators in wound tissues in patients compared to the control group Group I (n=68)
 |
| |
|
An important characteristic criterion for assessing the wound process was the identification of microbial contamination, the species composition of the microflora, and the timing of wound cleansing. The species composition of the microflora identified from the exudate of infected wounds of patients with purulent diseases of the soft tissues of the limbs, patients of the I comparison group, is presented in Figure 1.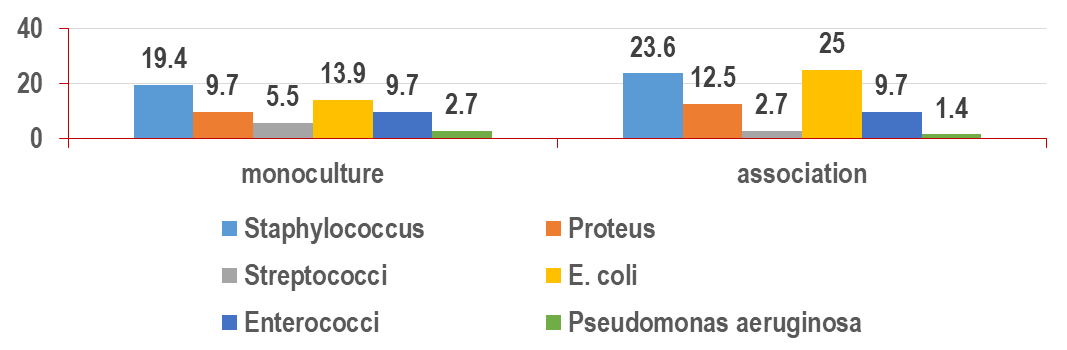 | Figure 1. Species composition of microflora and their sown exudate infected wounds of patients with purulent diseases of the soft limb tissues of comparison group I (n=68) |
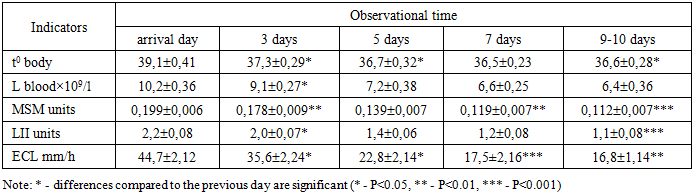
In the majority of cases, pathogenic staphylococcus was sown in 27 patients, of whom 12 (17.6%) were monoculture and 15 (22.1%) were association. In 26 observations, intestinal bacillus was sown, which was present in 9 (13.2%) cases as a monoculture and in 17 (25.0%) as a microbial association. The next most frequently identified species was proteus (15 observations), which was sown in 6 (8.8%) cases as a monoculture and in 9 (13.2%) as part of microbial associations. This was followed by enterococci—13 observations—sown in 6 (8.8%) cases as monocultures and in 7 (10.3%) as part of microbial associations. Streptococci found in 6 observations were 3 (4.4%) in the form of monocultures and associations, respectively. Bluefish rods were sown in 2 (2.9%) patients as a monoculture and in 1 (1.5%) as part of microbial associations.Dynamic monitoring of the level of microbial contamination of purulent wounds in patients of this subgroup revealed the following: at the time of admission, microbial contamination averaged 108 mt/g, and on the following day after surgical treatment of the wound with a ointment bandage, its values were 105 mt/g. By the 4th day of complex treatment, the degree of microbial contamination in these patients was below the critical level and amounted to 102 mt/g of tissue.In the analyzed group of patients, wound cleansing from infection occurred on average by 4.3±0.6 days. By the third day, the infiltrates had dissolved.On the fifth day, the cytological picture was predominantly inflammatory and inflammatory-regenerative in nature, and only by the seventh day was the predominantly regenerative type of cytograms recorded.Indicators of the main assessment criteria and the dynamics of the wound process—the late clearing of infection from the wound (only by the 4th day of treatment), the onset of granulation by the 6th–7th day of treatment, and the onset of epithelialization by the 8th–9th day of treatment—leave much to be desired. The biochemical indicators of the wound exudate normalize only by the 10th day of treatment. The average treatment duration for patients in the comparison group was 10.5±0.3 days. All of this necessitated the development of additional measures aimed at improving treatment methods for purulent soft tissue diseases.Group II included 54 patients with purulent diseases of the soft tissues of the upper and lower extremities. Of these, 29 (53.7%) patients had purulent wounds of the upper limbs, and 25 (46.3%) patients had purulent wounds of the lower limbs. Of the 54 examined patients in this group, 32 (59.2%) were admitted to the clinic with various purulent soft tissue diseases, 22 (40.82%) patients were admitted with previously existing extensive purulent wounds of various etiologies, who were admitted from other medical hospitals or outpatient clinics in the first phase of the wound process.All 32 patients admitted with various purulent diseases of the soft tissues of the limbs on the day of admission underwent an incision of the purulent focus and sanation of the wound process. Further treatment tactics were identical to those for patients with incoming purulent wounds, which included daily treatment of the wound with antiseptics and application of Levomekol ointment and 25% dimexide solution under an aseptic dressing, as in the control group, and unlike this group of patients, hyperventilation with oxygen flows was additionally performed according to our developed regimen for 4 hours 2 times a day. The hyperventilation session was conducted before the transition of the first phase of the wound process to the second phase. The criteria for assessing the transition of the wound process from the first phase to the second were the vascular cleansing of the wound from necrotic tissues and purulent secretions, the appearance of granulation tissue, bacteriological examination results, as well as cytological examination, which we performed in 31.5% of patients.Analysis of the body intoxication indicators in patients with purulent soft tissue diseases in comparison group II revealed the following changes (Table 5. As seen from the table, the body temperature of patients on the first day of treatment averaged 39.1 ± 0.410°C. The leukocyte content in the blood was 10.2 ± 0.36 × 109/L. The volume of average molecules averaged 0.199 0.006 units. Similarly, an increase in LII and ESR was noted.Table 5. Dynamics of intoxication indicators in patients with purulent soft tissue diseases of Group II (n=54)
 |
| |
|
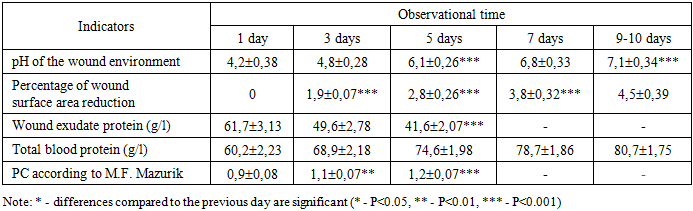
By the fifth day of treatment, patients in the main group with purulent soft tissue diseases had a tendency toward normalization. At the same time, for all indicators of body intoxication: body t0, L, MSM, LII, and blood ESR, a further decrease was noted, i.e., a trend toward normalization was noted – 36.7 0.32, 8.4 0.45×109; 0.158 0.009; 1.9 0.07; 32.9 and 2.36, respectively. Upon further treatment and observation, by the seventh day, all analyzed intoxication indicators were within the normal range.The next criteria for assessing the dynamics of the wound process in patients were the pH of the wound environment, the percentage of reduction in the wound surface area, and PC parameters according to M.F. Mazurik (Table 6). In the analyzed group of patients, on the first day of inpatient treatment, the initial pH level of the wound environment was significantly lower (acidosis) and averaged 4.2±0.38. Wound exudate protein averaged 61.7±3.13 g/l. At the same time, PC averaged 0.9±0.08 units.Table 6. Dynamics of biochemical indicators and wound healing rate in Group II patients (n=54)
 |
| |
|
By the seventh day, the wound area was 1.4±0.06, and the wound area significantly decreased by 3.8±0.32% per day. The pH of the wound medium averaged 6.8±0.38. The secretion of exudate from the wound has ceased, which, in our opinion, is due to the transition of the wound process from phase 1 to phase 2. By the seventh day of treatment, the pH of the wound environment became neutral. The reduction in wound surface area by the 10th day was 4.5±0.39%.To assess the oxygen saturation of wound tissues, the partial oxygen pressure (PO2) of the wound tissues was determined.The indicators presented in Table 7 indicate that if the RO2 of wound tissues on the day of admission was 18.2 mm Hg, it increased to 26.9 mm Hg on the 3rd day, which is 8.7 mm Hg higher than on the day of admission. By the fifth day of treatment using hyperventilation with oxygen flows, the oxygen tension in the wound tissues increased to 32.7 and 0.5 mm Hg, reaching normal values; by the seventh day, these figures reached 34.5 and 0.7 mm Hg. Upon further treatment, by the 10th day, the tissue wound RO2 indicators were 38.6 and 0.4 mm Hg.Table 7. Dynamics of RO2 indicators in wound tissues in patients with primary Group II (n=54)
 |
| |
|
An important characteristic criterion for assessing the wound process was the identification of microbial contamination levels, the species composition of the microflora, and the timing of wound cleansing. The species composition of the microflora identified from the exudate of infected wounds in patients with purulent diseases of the soft tissues of the limbs, Group II patients, is presented in Figure 2.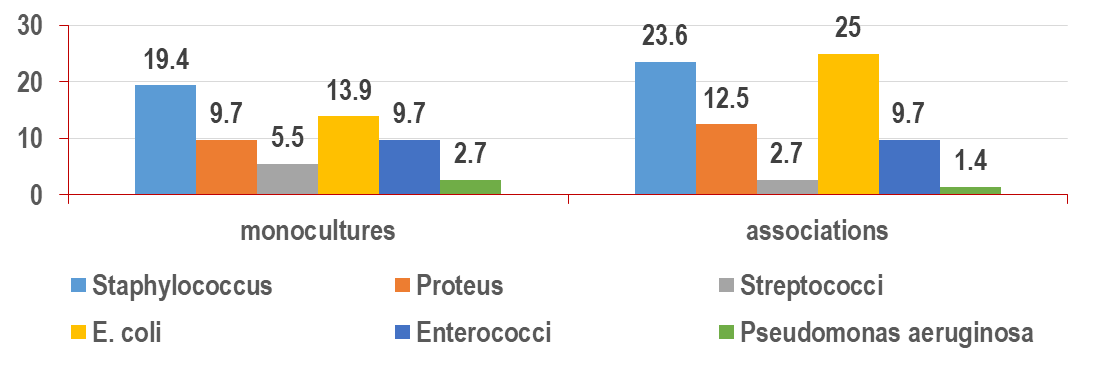 | Figure 2. Species composition of microflora and their sown exudate infected wounds of patients with purulent diseases of the soft limb tissues of group II (n=54) |
In most cases, pathogenic staphylococcus was isolated in 22 patients, of whom 9 (16.6%) were monoculture and 13 (24.1%) were association. In 21 observations, intestinal bacilli were sown, which were present in 7 (12.9%) cases as monocultures and in 14 (25.9%) as microbial associations. The next most frequently detected species was proteus 12 observations sown in 5 (9.2%) cases as a monoculture and in 7 (12.9%) as part of microbial associations. This was followed by enterococci 11 observations sown in 4 (7.4%) cases as monocultures and in 7 (12.9%) as part of microbial associations. Streptococci found in 4 observations were 2 (3.7%) in the form of monocultures and associations, respectively. The bluish-purple bacillus was isolated in 2 (3.7%) patients as a monoculture and in 1 (1.8%) as a microbial association. Dynamic monitoring of the level of microbial contamination of purulent wounds in patients of this subgroup revealed the following: at the time of admission, microbial contamination averaged 108 mt/g, and on the following day after surgical treatment of the wound with a ointment bandage, its values were 105 mt/g. By the 2nd day of complex treatment, the degree of microbial contamination in these patients was below the critical level and amounted to 102 mt/g of tissue.In the analyzed group of patients, the cleansing of wounds from infection occurred on average by 2.2±0.3 days. By the second day, the infiltrates had dissolved.The onset of granulation is noted on average on the fourth day. These data are confirmed by cytological studies. Thus, on the second day, a large number of destructive and degeneratively altered leukocytes, predominantly with incomplete and distorted types of phagocytosis, were detected in cytological preparations.On the third day, the cytological picture was mostly inflammatory and inflammatory-regenerative in nature, and only by the sixth day was the predominantly regenerative type of cytograms recorded.The conducted study of patients in the main group with purulent-necrotic diseases of the soft tissues of the limbs using wound hyperventilation with oxygen flow revealed the following features of the wound process: the use of local treatment for purulent wound hyperventilation with oxygen flow for 4 hours 2 times a day with subsequent application of levomekol ointment under an aseptic dressing leads to complete cleansing of the wound and normalization of clinical and laboratory indicators of intoxication. At the same time, to assess the course of the wound process, both body intoxication indicators (L, MSM, LII, ESR) and biochemical indicators of wound exudate (pH, wound exudate protein, PC according to Mazurik) are of important diagnostic and prognostic importance.Indicators of the main criteria for evaluating the wound process and its dynamics include the late clearing of infection from the wound (as early as the 2nd day of treatment), the onset of granulation by the 4th day of treatment, and the onset of epithelialization by the 6th day of treatment, indicating the effectiveness of this treatment method. The biochemical indicators of wound exudate normalize by the 5th day of treatment. The average treatment duration for patients in the comparison group was 6.5±0.5 days.Thus, the use of wound hyperventilation with oxygen flows in the complex treatment of purulent wounds of the limbs is the most effective method, which reduces wound cleansing time by 2.5±0.5 days and hospital stay by 4.0±0.2 days, which improves the results of medical care for patients with purulent diseases of the soft tissues of the limbs. All of this contributes to the economic efficiency of this developed methodology and allows for the recommendation of this treatment method for wide application in medical practice.
4. Conclusions
1. When treating patients with purulent diseases of the soft tissues of the limbs using the traditional method using a 25% dimexide solution with a levomekol ointment under a gauze bandage, it is noted that the wound clears of infection later (only by the 4th day of treatment), granulation begins to appear by the 6-7th day of treatment, and epithelialization begins to appear by the 8th-9th day of treatment. The biochemical indicators of wound exudate normalize only by the 10th day of treatment. Wound tissue RO2 indicators on the day of admission were below normal, ranging from 18.8 to 0.4 mm Hg; against the background of traditional treatment, all these indicators normalized at a slow pace only on the 9th–10th day of treatment. At the same time, the average duration of treatment for patients is 10.5±0.3 days, which requires the development of additional measures aimed at improving treatment methods.2. When applying the developed methodology of hyperventilation of wounds with oxygen flows as part of the complex treatment of patients with purulent diseases of the soft tissues of the limbs, the main criteria for assessing and dynamics of the wound process were the late clearing of the wound from infection (as early as the 2nd day of treatment), the onset of granulation by the 4th day of treatment, and the onset of epithelialization by the 6th day of treatment, indicating the effectiveness of this treatment method. The biochemical indicators of wound exudate normalize by the 5th day of treatment. Wound tissue RO2 indicators on the day of admission in patients of the main group were also below normal, ranging from 18.2 to 0.5 mm Hg against the background of comprehensive treatment using local hyperventilation of the wound with oxygen flows according to the methodology we developed, all these indicators normalize rapidly by the 5-6th day of treatment. At the same time, the average treatment duration for patients in the comparison group was 6.5±0.5 days.3. The use of hyperventilation of wounds with oxygen flows in the complex treatment of patients with purulent diseases of the soft tissues of the limbs reduces the period of wound cleansing from infection to 2.0±0.3 days of treatment, infiltrate dissolution to 1.5±0.5 days, granulation to 2.5±0.4 days, and epithelialization to 2.0±0.5 days. The normalization time for wound tissue RO2 indicators is 3-4 days earlier than with the traditional treatment method. All of this contributes to reducing the duration of inpatient treatment by 3-4 days.4. The use of hyperventilation of wounds with oxygen flows in the complex treatment of patients with purulent diseases of the soft tissues of the limbs according to the developed methodology using a wound hyperventilation device is a highly therapeutic and cost-effective treatment method that can be recommended for wide application in clinical practice.
References
| [1] | Alekseeva N.T. Morphological assessment of regenerate in the healing of purulent skin wounds under the influence of various regional impact methods // Journal of Anatomy and Histopatology. – 2014. – Vol. 3. – No. 2. |
| [2] | Bejalo V. A., Sysolyatina E. V. New Opportunities for Combating Bioplates in Healing Chronic Wounds // Infectious Diseases: News. Opinions. Learning. – 2025. – Vol. 14. - No. 1 (50). – P. 80-89. |
| [3] | Vladimirova O. V. et al. Opportunities for monitoring and stimulating long-term unhealing wounds using a comprehensive approach // Medical Bulletin of the North Caucasus. – 2025. – Vol. 20. – No. 4. – P. 326-330. |
| [4] | Grigoryan A. Yu. et al. Application of factor analysis in evaluating wound treatment effectiveness // Siberian Scientific Medical Journal. – 2025. – Vol. 45. – No. 5. – P. 188-198. |
| [5] | Yegorov V. S. et al. Morphological assessment of the effectiveness of treating infected wounds with high-intensity pulsed broadband radiation // Biomedical Photonics. - 2024. – Vol. 13. – No. 3. – P. 31-41. |
| [6] | Chudnykh S. M. et al. Results of the planimetric study of experimentally modeled infected wounds under the influence of high-intensity pulsed broadband radiation // Biomedical Photonics. – 2025. – Vol. 14. - No. 1. – P. 29-35. |
| [7] | Chen P, Zou Y, Liu Y, Han W, Zhang M, Wu Y, Yin R. Low-level photodynamic therapy in chronic wounds. Photodiagnosis Photodyn Ther. 2024 Apr; 46: 104085. |
| [8] | Everts P, Onishi K, Jayaram P, Lana JF, Mautner K. Platelet-Rich Plasma: New Performance Understandings and Therapeutic Considerations in 2020. Int J Mol Sci. 2020 Oct 21; 21(20): 7794. |
| [9] | He L, Feng Q, Yu C, Wu A, Li Y, Wang X. Three-in-One Multifunctional Metal-Organic Gel-Encapsulated Microneedles for Programmed Treatment of Infected Wounds. Adv Healthc Mater. 2026 Apr; 15(15): e04748. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML