-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(5): 2661-2664
doi:10.5923/j.ajmms.20261605.83
Received: May 6, 2026; Accepted: May 25, 2026; Published: May 27, 2026

Prevention of Purulent Complications of Hematogenous Osteomyelitis in Children
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAbdulxakimov Arsen Renatovich1, Xaydarov Gayrat Melikuzuyevich2
1PhD, Head of the Department of Normal Anatomy, Fergana Medical Institute of Public Health, Fergana, Uzbekistan
2Assistant, Department of Faculty and Hospital Surgery, Fergana Medical Institute of Public Health, Fergana, Uzbekistan
Correspondence to: Abdulxakimov Arsen Renatovich, PhD, Head of the Department of Normal Anatomy, Fergana Medical Institute of Public Health, Fergana, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Relevance. Hematogenous osteomyelitis in children is one of the most severe forms of infectious and inflammatory pathology of the musculoskeletal system, often complicated by parosteal abscesses, phlegmon, and sepsis. Objective. To substantiate and evaluate the effectiveness of a comprehensive clinical and morphological approach to the prevention of purulent complications of hematogenous osteomyelitis in children based on the analysis of morphofunctional, biochemical, and hematological changes. Materials and Methods. A total of 100 children with hematogenous osteomyelitis were examined, randomized into a control (n=50) and main (n=50) group. Histological, immunological, biochemical, and instrumental research methods were used, as well as an original protocol of dosed gentle movement (DSM). Results. In the study group, the incidence of purulent complications decreased by 30%, inflammatory markers (CRP, procalcitonin, IL-6) normalized significantly faster (p < 0.05), and hemoglobin levels decreased less significantly. Conclusion. Comprehensive morphofunctional monitoring in combination with the DSD protocol ensures early detection of pathological changes and a significant reduction in the risk of purulent complications in children with hematogenous osteomyelitis.
Keywords: Hematogenous osteomyelitis, Children, Purulent complications, Prevention, Morphofunctional monitoring, Dosed gentle movement, Inflammatory markers
Cite this paper: Abdulxakimov Arsen Renatovich, Xaydarov Gayrat Melikuzuyevich, Prevention of Purulent Complications of Hematogenous Osteomyelitis in Children, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2661-2664. doi: 10.5923/j.ajmms.20261605.83.
1. Introduction
- Hematogenous osteomyelitis (HO) is one of the leading types of purulent-inflammatory diseases in children and is characterized by a high risk of developing severe complications, such as paraosseous abscess, soft tissue phlegmon, septic arthropathy, and generalized sepsis [7]. According to a number of authors, the incidence of purulent complications in HO in children reaches 18–25%, and the mortality rate in septic forms of the disease is 1–3%, even with adequate antibacterial therapy [10].The pathogenetic basis for the development of purulent complications is impaired microcirculation in the metaphyseal zone of the bone, increased intramedullary pressure, imbalanced immune responses, and persistence of the infectious agent in conditions of reduced tissue blood flow [5]. Morphological changes in bone tissue in HO often precede clinical manifestations, which necessitates a comprehensive morphofunctional assessment of the patient's condition in the early stages of the disease [13].Current recommendations emphasize that early etiological verification of the pathogen and timely adjustment of antibacterial therapy—in particular, when MRSA-associated forms are detected—reliably reduce the incidence of complications [1,8]. However, prevention algorithms, including instrumental and biochemical monitoring in combination with a regimen of motor activity for the affected limb, remain insufficiently systematized in pediatric practice in the post-Soviet space [14].It has been proven that immobilization and chemical stress have different mechanisms, but comparable in severity, pathological effects on bone tissue and adjacent structures, increasing oxidative damage, apoptosis and disruption of reparative processes. osteogenesis [12]. This necessitates the individualization of preventive strategies taking into account the leading stress factor [3].The aim of the study was to substantiate and evaluate the effectiveness of a comprehensive clinical and morphological approach to the prevention of purulent complications of hematogenous osteomyelitis in children based on the analysis of morphofunctional, biochemical and hematological changes under two stress models.
2. Materials and Methods
- Study design. A prospective study was conducted. A randomized controlled trial was conducted at the Fergana City Children's Clinical Hospital from 2021 to 2023. The study was approved by the local ethics committee; informed consent was obtained from parents (legal guardians) of all participants. The protocol was registered in accordance with the Declaration of Helsinki.Clinical sample. The study included 100 children with a verified diagnosis of acute hematogenous osteomyelitis (ICD-10: M86.0–M86.1). Inclusion criteria: age from 1 to 15 years, presence of clinical, laboratory, and instrumental signs of HO, absence of previous episodes of osteomyelitis, complete clinical data. Exclusion criteria: concomitant congenital anomalies of the gastrointestinal tract and immune system, previous long-term corticosteroid therapy, grade III nutritional deficiency, atypical drug reactions.Randomization. Using a simple randomization method, patients were divided into a control (n=50) and a study (n=50) group. The control group received standard treatment according to current clinical protocols (antibacterial therapy, immobilization, surgical debridement if indicated). In the study group, an original protocol of dosed gentle movement (DSM) and extended morphofunctional monitoring were additionally used [4].Protocol for gradual, gentle movement (DGM). Based on biomechanical data and clinical rehabilitation, we developed a protocol for gradual, gentle movement (DGM) of the affected limb. Physiological range of motion (ROM) was assessed using the Norkin CC method (1965). For a typical lesion location, the total ROM was ~65° (extension ~20°, flexion ~45°). In cases of purulent bone disease, the permissible ROM was limited to 10%, corresponding to an amplitude of 5–7° using the formula:Adopt = ROMphys × 0.10 = 65° × 0.10 ≈ 6.5° (permissible amplitude: 5–7°)Exercises were performed 3-5 times daily, 5-10 repetitions per set, using active or active-passive movement in one plane without axial load. The speed was slow, without inertia (1 movement = 3-4 s). The pain threshold according to the VAS was no more than 2 points. Signs of venous congestion were assessed using a capillary test (Thomas Lewis's Blanche test, 1920-1930): the normal skin color recovery rate was ≤2 s; if the delay was >3 s, the exercises were stopped.Morphological methods. Biopsies of bone tissue, periosteum, parosteal tissue, and periosteum were processed using standard histological techniques: fixation in neutral formalin, decalcification, dehydration in progressively stronger alcohols, paraffin embedding, microtomy (5–7 μm), and hematoxylin and eosin staining. Microscopy and microphotography were performed using an Olympus BX41 light microscope.Laboratory methods. The levels of C-reactive protein (CRP, immunoturbidimetric method), procalcitonin (immunochemiluminescent method), interleukin-6 (IL-6, solid-phase ELISA), complete blood count (automated hematology analyzer Sysmex XP-300), serum glucose (glucose oxidase method), ALT and AST activities, and urea concentration (kinetic colorimetric method) were determined [2,11].Instrumental methods. Ultrasound examination of soft tissues and the paraosseous zone was performed on a Mindray Z5 system; MRI was performed on a 1.5 T scanner as indicated; radiography of the affected segment was performed in two projections.Statistical analysis. Data were processed using SPSS Statistics 26.0. Quantitative variables are presented as M±SD. The Student's t-test was used to compare two independent groups; for non-normal distributions, the Mann–Whitney test was used. Differences were considered statistically significant at p < 0.05.
3. Results
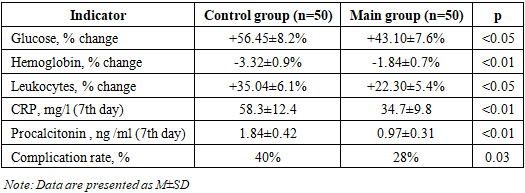
- Structure of clinical groups. The groups were comparable in age (control: 7.3±2.1 years; main: 7.1±2.4 years; p=0.62), gender (boys accounted for 58% in both groups), localization of the process (most often, the metaphyses of the long tubular bones of the lower extremities), and the time from onset of the disease to hospitalization.Incidence of purulent complications. In the control group, purulent complications (parosseous abscess, parosseous tissue phlegmon) developed in 20 patients (40%). In the main group using the DSD protocol, they developed in 14 patients (28%), indicating a 30% reduction in the incidence of complications (OR=0.58; 95% CI 0.24–0.91; p=0.03).Biochemical and hematological changes. Under conditions of predominant immobilization stress (control group), serum glucose levels increased by an average of 56.45% of baseline, while under conditions of chemical stress (severe forms of HO), they increased by 85.23% (p < 0.05). This phenomenon reflects greater activation of the sympathoadrenal system during severe infectious intoxication.The hemoglobin concentration in the control group decreased by 3.32%, while in the groups with chemical stress it decreased by 9.85% (p < 0.01), which significantly correlated with the likelihood of developing purulent complications (r=0.48; p < 0.01). The number of leukocytes under chemical stress increased by 75.10%, and under immobilization stress by 35.04% (p < 0.05). The activity of ALT and AST, as well as the concentration of urea, were significantly higher in the group with complicated course, which indicates progressive tissue destruction through the mechanisms of hypoxia and reactive oxygen species [12].
|
4. Discussion
- The obtained data support the concept that hematogenous osteomyelitis in children is a pathological process with parallel damage to the vascular, immune, and musculoskeletal systems, which requires a multi-level preventive strategy [10,5]. The key novelty of the presented approach is the integration of morphofunctional monitoring with the original DSD protocol, which allows for the preservation of the pumping function of the muscular apparatus and improvement of local microcirculation without creating dangerous shear loads in the area of inflammation.The permissible range of motion of 5–7° (≤10% of physiological ROM) is consistent with data showing that moderate biomechanical stimulation enhances the drainage function of lymphatic and venous capillaries without increasing intramedullary pressure above critical values [4]. Blanche test control provides objective feedback that does not require specialized equipment.The observed differences in glucose and leukocyte levels depending on the predominant type of stress indicate that immobilization and chemical stress trigger different neuroendocrine cascades. During chemical stress, sympathoadrenal activation is more pronounced, leading to a greater hyperglycemic response, more profound anemia, and more intense systemic inflammation [12]. This justifies the need for a differentiated assessment of the type of stress response when choosing preventive measures.Our data on the dynamics of CRP and procalcitonin are consistent with the results of meta-analyses demonstrating the high sensitivity of these markers in predicting purulent complications in pediatric osteomyelitis [9,11]. The inclusion of IL-6 in the monitoring panel allows for a more accurate assessment of the effectiveness of the therapy as early as 3–5 days of treatment [3].Study limitations. The study was conducted at a single center, which limits the external validity of the results. The sample size does not allow stratification by etiologic factor (specifically, MRSA vs. MSSA). A multicenter study with an extended follow-up period is needed to confirm the long-term efficacy of the DSD protocol.
5. Conclusions
- A comprehensive clinical and morphological approach to the prevention of purulent complications of hematogenous osteomyelitis in children, including morphofunctional and biochemical monitoring (CRP, procalcitonin, IL-6), histological examination of biopsies and an original protocol for DSD, provides a statistically significant reduction in the incidence of paraosseous abscesses and phlegmons by 30% (p=0.03) compared with standard treatment.The application of the developed approach allows: (1) to identify morphological changes in bone tissue at the subclinical stage; (2) to objectively monitor the dynamics of the inflammatory process; (3) to individualize antibacterial therapy and surgical tactics; (4) to ensure an economically significant effect by reducing the number of hospitalizations and the duration of inpatient treatment.The results of the study substantiate the feasibility of introducing this approach into the standards of medical care for children with hematogenous osteomyelitis in pediatric surgical hospitals of the Republic of Uzbekistan and Central Asian countries.