-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(5): 2651-2654
doi:10.5923/j.ajmms.20261605.80
Received: Apr. 12, 2026; Accepted: May 10, 2026; Published: May 27, 2026

Dermoscopic-Histopathological Correlation Across Disease Stages of Cutaneous Lichen Sclerosus: A Single-Center Observational Study
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLOmasharifa Binti Jamal Po1, Sidikov Akmal Abdikakharovich2
1Candidate of Medical Sciences, Associate Professor, Department of Obstetrics and Gynecology of Postgraduate Education, Kursk State Medical University, Kursk, Russia
2Doctor of Medical Sciences, Professor, Rector of the Fergana Medical Institute of Public Health, Fergana, Uzbekistan
Correspondence to: Omasharifa Binti Jamal Po, Candidate of Medical Sciences, Associate Professor, Department of Obstetrics and Gynecology of Postgraduate Education, Kursk State Medical University, Kursk, Russia.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Purpose: To identify stage-specific dermoscopic patterns of cutaneous lichen sclerosus (LS) and correlate them with histopathological changes. Methods: The manuscript is based on a dissertation study of 60 patients with LS (30 women and 30 men) examined clinically, dermoscopically and histologically. Representative lesions were additionally analyzed according to inflammatory, inflammatory-sclerotic, sclerosis, and scleroatrophic patterns. Results: Active lesions were characterized by erythematous foci, red focused vessels, linear irregular vessels and dotted vessels, together with bright white or yellow-white areas. In the inflammatory-sclerotic pattern, erythematous foci were present in 92%, red focused vessels in 80%, dotted vessels in 56%, and linear irregular vessels in 36% of representative lesions, while bright white/yellow-white areas and yellow-white keratotic follicular plugs were each found in 100%. More advanced lesions showed increasing dominance of crystalline structures, white structureless zones, keratotic plugs, and reduced vascular density. Histologically, the progressive stage corresponded to vacuolar interface dermatitis with a dense lichenoid infiltrate, whereas the chronic stage showed dense fibrosis of the papillary dermis and sclerosis with a lower inflammatory burden. Conclusion: Dermoscopy reflects stage-dependent structural changes in LS and can guide non-invasive staging, biopsy targeting and differential diagnosis.
Keywords: Lichen sclerosus, Dermoscopy, Histopathology, Stage-specific changes, Differential diagnosis, Morphea
Cite this paper: Omasharifa Binti Jamal Po, Sidikov Akmal Abdikakharovich, Dermoscopic-Histopathological Correlation Across Disease Stages of Cutaneous Lichen Sclerosus: A Single-Center Observational Study, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2651-2654. doi: 10.5923/j.ajmms.20261605.80.
1. Introduction
- Lichen sclerosus (LS) is a chronic inflammatory and fibroatrophic dermatosis that predominantly affects the anogenital region, although extragenital lesions may also occur [1-4]. Despite the availability of clinical diagnostic criteria, early lesions may mimic vitiligo, leukoplakia, lichen planus, chronic eczema or morphea, which delays diagnosis and postpones treatment [1,4,5]. Dermoscopy is increasingly used as a bedside method for recognizing LS, identifying activity-related vascular clues and selecting the most informative site for biopsy [5-8].The dissertation on which this manuscript is based addressed a clinically important gap: the relationship between dermoscopic changes and the underlying histopathological stage of the disease. The main practical question is whether dermoscopy can separate active inflammatory lesions from fibrosing and scleroatrophic lesions and therefore improve both diagnosis and stage-oriented management. The objective of the present article was to analyze the dermoscopic-histopathological correlation in cutaneous LS and to summarize the stage-specific patterns observed in the cohort.
2. Materials and Methods
- The study included 60 patients with lichen sclerosus, comprising 30 women with vulvar lesions and 30 men with penile lesions. All patients underwent clinical examination, dermoscopic assessment, and histopathological evaluation of biopsy specimens. Immunohistochemical findings were not the primary focus of the present study and are discussed only insofar as they support the interpretation of disease stage.Dermoscopy was performed using a Heine dermatoscope. The examination protocol included assessment of inflammatory vascular structures, bright white and yellow-white areas, crystalline structures, follicular keratotic plugs, pigmented structures, erosions, and hemorrhagic spots. In addition to the analysis of the entire cohort, representative lesions were classified into inflammatory, inflammatory-sclerotic, sclerotic, and scleroatrophic patterns. Histopathological evaluation was performed according to Ackerman’s inflammatory pattern framework, with particular emphasis on vacuolar and lichenoid interface dermatitis, as well as superficial fibrosing dermatitis. The present article reports the validated descriptive and comparative findings.
3. Results
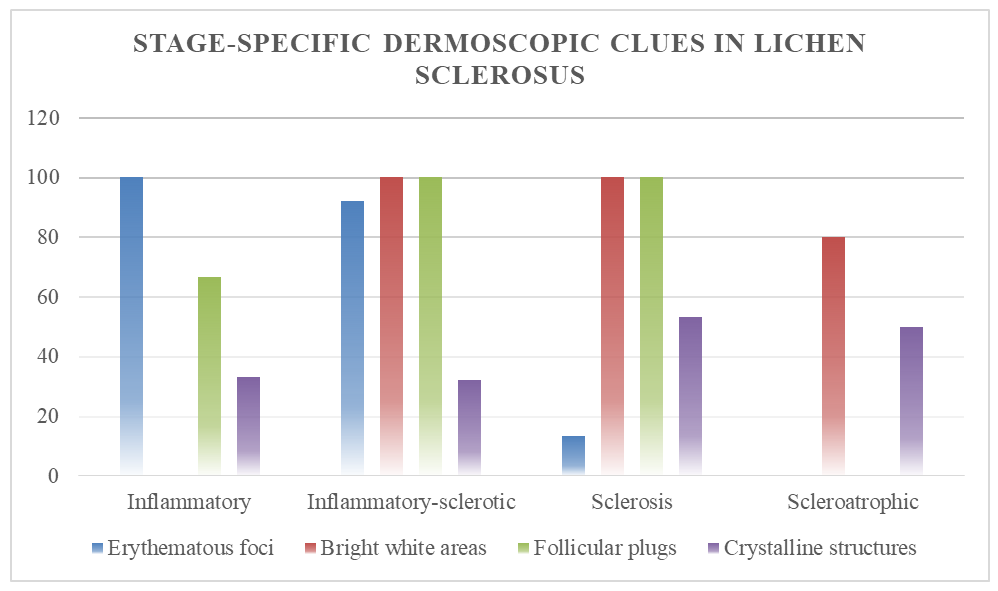
- A stable dermoscopic background across disease stages consisted of bright white or yellow-white structureless areas corresponding to sclerosis and hyalinization. However, the vascular component and ancillary structures changed substantially according to lesion activity. In inflammatory lesions, erythematous foci were present in all representative lesions, whereas red focused vessels, branching linear vessels, linear irregular vessels and crystalline structures were each found in one third. Yellow-white keratotic follicular plugs and hemorrhagic spots were documented in two thirds of these early active lesions.The inflammatory-sclerotic pattern showed the most pronounced vascular activation. Erythematous foci were seen in 23/25 representative lesions (92%), red focused vessels in 20/25 (80%), dotted vessels in 14/25 (56%), and linear irregular vessels in 9/25 (36%). Bright white/yellow-white areas and yellow-white keratotic follicular plugs were both detected in 25/25 lesions (100%). Crystalline structures were present in 8/25 (32%), while limited erosions and rainbow effect were observed in 2/25 lesions (8%) each. This constellation indicates ongoing inflammatory activity superimposed on early sclerosis.
 | Figure 1. Stage-specific dermatoscopic signs of scleroatrophic lichen |
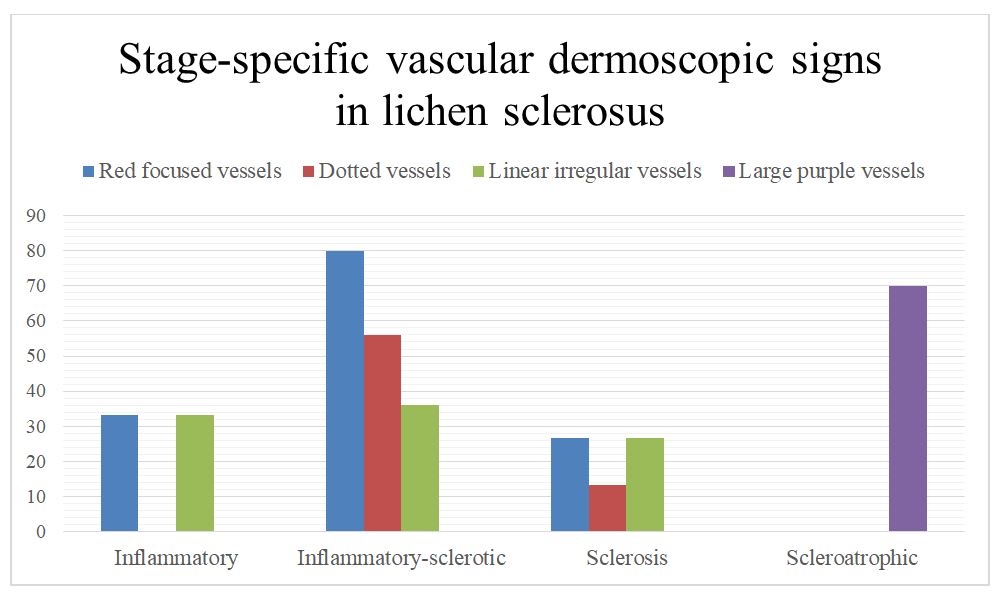 | Figure 2. Vascular dermatoscopic features of lichen sclerosus et atrophicus depending on the stage of the disease |
4. Discussion
- The present findings are consistent with published work showing that white structureless areas, follicular plugging and activity-related vascular structures are core dermoscopic clues of LS [5-8]. The distinctive value of dermoscopy in LS lies not only in diagnosis but also in biologic staging. The prominent vascular component in active lesions probably reflects endothelial activation and microvascular remodeling, whereas the later reduction of inflammatory vessels with persistence of white and crystalline clues reflects collagen remodeling and sclerosis [1,2,6,9].A clinically relevant implication is biopsy targeting. Early erythematous or vascular lesions can be histologically subtle, while advanced sclerotic plaques may mainly show fibrosis. Dermoscopy helps select lesions with both active and diagnostic morphology and therefore improves clinicopathological concordance. It also helps identify lesions that warrant closer surveillance because new erosions, ulceration, bleeding and proliferating atypical vessels may indicate an unfavorable course or malignant progression [8-10].The main strength of this study is the direct integration of bedside dermoscopy with validated histopathology in a sex-balanced cohort. The main limitation is that the work was performed in a single center and the stage-specific dermoscopic analysis was based on representative lesions rather than a prospective longitudinal imaging protocol. Even so, the observed stage gradient is internally coherent and clinically applicable.
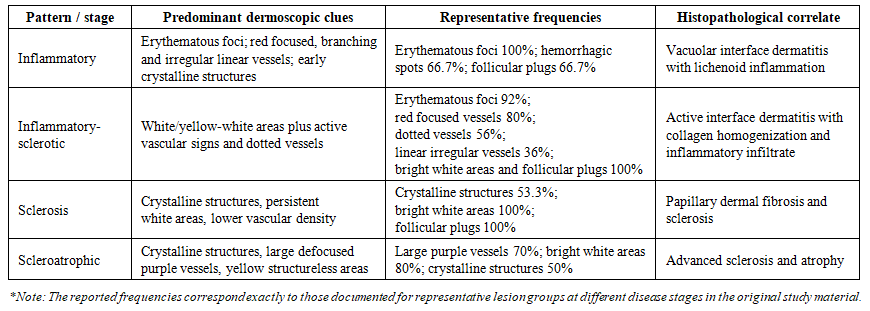 | Table 1. Stage-oriented dermoscopic and histopathological correlates in lichen sclerosus |
5. Conclusions
- Dermoscopy in LS is not merely an adjunctive imaging technique. It reflects stage-specific biological changes, improves non-invasive recognition of disease activity, supports differential diagnosis with morphea and other white dermatoses, and assists in rational biopsy selection. Active LS is characterized by erythematous foci and polymorphous vessels on a white background, whereas chronic lesions show dominant white/yellow-white areas, crystalline structures and follicular plugs that correspond to fibrosis and sclerosis.