-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(5): 2646-2650
doi:10.5923/j.ajmms.20261605.79
Received: Apr. 26, 2026; Accepted: May 19, 2026; Published: May 27, 2026

Improvement of Disability Prevention in Risk Groups of 0-3-Year-Old Children Based on the Regional Model of Early Intervention
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAlimova I. A.
Fergana Medical Institute of Public Health, Fergana, Uzbekistan
Correspondence to: Alimova I. A., Fergana Medical Institute of Public Health, Fergana, Uzbekistan.
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Background. Expanding early detection and early intervention is among the most effective strategies to prevent long-term functional limitations in children aged 0 to 3 years. Objective. To evaluate the effectiveness of implementing a regional model of a comprehensive individualized early intervention and rehabilitation program (CIPR) for young children from at-risk groups. Materials and Methods. We analyzed 523 medical records of children aged 0 to 3 years who were followed in primary health care facilities in Fergana and in the regional perinatal center during 2020 to 2025. In addition, outcome dynamics were assessed in 50 children aged 0 to 3 years who completed a three-month CIPR cycle. The following indicators were considered: coverage of scheduled preventive examinations (at 1, 3, 6, and 12 months), use of standardized developmental assessment scales, changes in functional skills and disability status. Results. Scheduled examinations were completed by 93.5% of children at 1 month and by 79.7% at 12 months. Standardized developmental assessment scales were used in 58.9% of cases. After completion of the program, mean developmental scores increased by 1.7 to 1.9 score units across the main domains. The proportion of children with disability decreased from 24% to 16%, and referrals to the medical rehabilitation center decreased from 40% to 16%. Family satisfaction with the program outcomes was 90%. Conclusion. The regional CIPR model may be regarded as a practice-oriented organizational approach to strengthen outpatient rehabilitation and prevent disability in children aged 0 to 3 years, combining interdisciplinary assessment, caregiver education, and regular follow-up.
Keywords: Early childhood, Disability, Early intervention, Interdisciplinary team, Family-centered care, Rehabilitation, Fergana region
Cite this paper: Alimova I. A., Improvement of Disability Prevention in Risk Groups of 0-3-Year-Old Children Based on the Regional Model of Early Intervention, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2646-2650. doi: 10.5923/j.ajmms.20261605.79.
1. Introduction
- Childhood disability remains a major public health and social issue. UNICEF estimates that about 240 million children aged 0-17 worldwide live with disabilities, which is roughly one in ten children. Children with persistent functional limitations are more likely to experience developmental delay, social exclusion, and barriers in access to health and education services, thereby reinforcing inequality [1].In the Republic of Uzbekistan, official statistics report 941.9 thousand persons with disabilities at the end of 2023, including 161.9 thousand children under 18 [2]. At the same time, the World Bank technical note indicates that 142.3 thousand children under 18 were certified as having disabilities (December 2022), which illustrates differences in definitions, administrative procedures, and reference periods, and supports the need for standardized monitoring [3]. At the regional level, Fergana region maintains a high burden: according to published regional statistical data, 15.5 thousand children with disabilities under 18 were registered in Fergana region at the end of 2024 [4].Contemporary early childhood intervention frameworks emphasize early identification, interdisciplinary assessment, individualized planning, and active caregiver involvement, with support delivered in the child’s natural environments and monitored over time. Due to high neuroplasticity in early childhood, timely developmental surveillance, screening, and intervention before age 3 are considered especially important for children from risk groups [8]. In this context, strengthening outpatient habilitation and structured caregiver education within primary health care is a practical direction for preventing avoidable disability and improving functional outcomes in children aged 0-3 years [5-7].Objective. To assess the effectiveness of implementing a regional comprehensive individualized early intervention and rehabilitation program (CIPR) for children aged 0 to 3 years from risk groups, using retrospective medical record review and pilot implementation data.
2. Materials and Methods
- Study design and setting. The study combined (1) a retrospective review of outpatient and perinatal center records and (2) a pilot before-after assessment of a three-month CIPR cycle in children aged 0-3 years in Fergana, Uzbekistan (2020-2025).Participants and data sources. The study was conducted within a dissertation project in preventive medicine. A retrospective review was performed of 523 medical records of children aged 0 to 3 years who were followed in outpatient primary care clinics in Fergana and at the Fergana Regional Perinatal Center during 2020 to 2025. The retrospective cohort included (1) children aged 0 to 3 years with an established disability status and (2) children with high perinatal and/or neurological risk without formal disability status. The following indicators were assessed: coverage of scheduled preventive examinations at 1, 3, 6, and 12 months, timeliness of referrals to specialist care, and the use of standardized developmental assessment tools as part of developmental surveillance and screening.To evaluate the regional CIPR model, a pilot group of 50 children aged 0 to 3 years with different types of developmental disorders was enrolled in a three-month early intervention cycle. Outcomes were evaluated across major functional domains (speech and language, gross motor, fine motor, cognitive, and socio-emotional development) based on standardized scales and interdisciplinary team observations, consistent with contemporary early childhood intervention frameworks emphasizing individualized planning and family-centered support. Additional endpoints included changes in disability status following re-evaluation by the medical-psychological-pedagogical commission and the frequency of referrals to the medical rehabilitation center (MRC).Intervention: regional CIPR model (organizational pathway). In this article, the “regional model of early intervention” is understood as a standardized outpatient care pathway for children aged 0-3 years from at-risk groups, implemented in primary health care in Fergana in coordination with the regional perinatal center and linked to referral mechanisms (medical rehabilitation center and disability status re-evaluation). Thus, CIPR is not a statistical model; it is a structured service package delivered as a time-limited cycle with documented baseline assessment, individualized planning, caregiver training, and follow-up monitoring.The pathway includes sequential components: (1) early identification and triage during scheduled preventive examinations and/or postnatal follow-up; (2) standardized developmental screening and interdisciplinary assessment; (3) an individualized plan with measurable domain targets and a structured home program; (4) outpatient habilitation/rehabilitation support combined with structured caregiver education; (5) scheduled follow-up with repeat developmental assessment and documentation of domain scores; (6) escalation criteria and referral decisions, including referral to MRC or disability status re-evaluation when indicated.In the pilot part of this study, the CIPR package was implemented as a three-month cycle with baseline and endline assessments using standardized developmental scales and interdisciplinary team observations across the main functional domains.Outcomes. Primary outcomes included coverage of scheduled preventive examinations (1, 3, 6, and 12 months), use of standardized developmental assessment tools in routine visits, and changes in functional domain scores during the pilot program. Secondary outcomes included change in disability status after re-evaluation and changes in referral frequency to the medical rehabilitation center (MRC).
3. Results
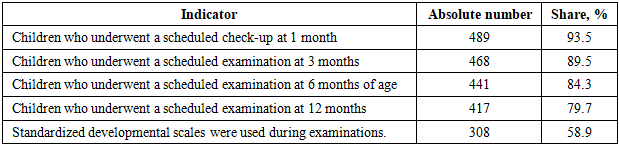
- Review of medical records demonstrated a progressive decline in coverage of scheduled preventive examinations as children aged: from 93.5% at 1 month to 79.7% at 12 months (Table 1). Standardized developmental assessment tools were used in 58.9% of preventive visits, which reduces the sensitivity of early detection and limits timely referral planning and early habilitation pathways, as recommended by contemporary developmental surveillance and screening frameworks.
|
|
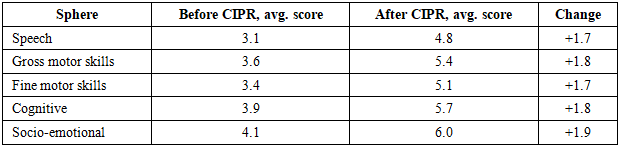
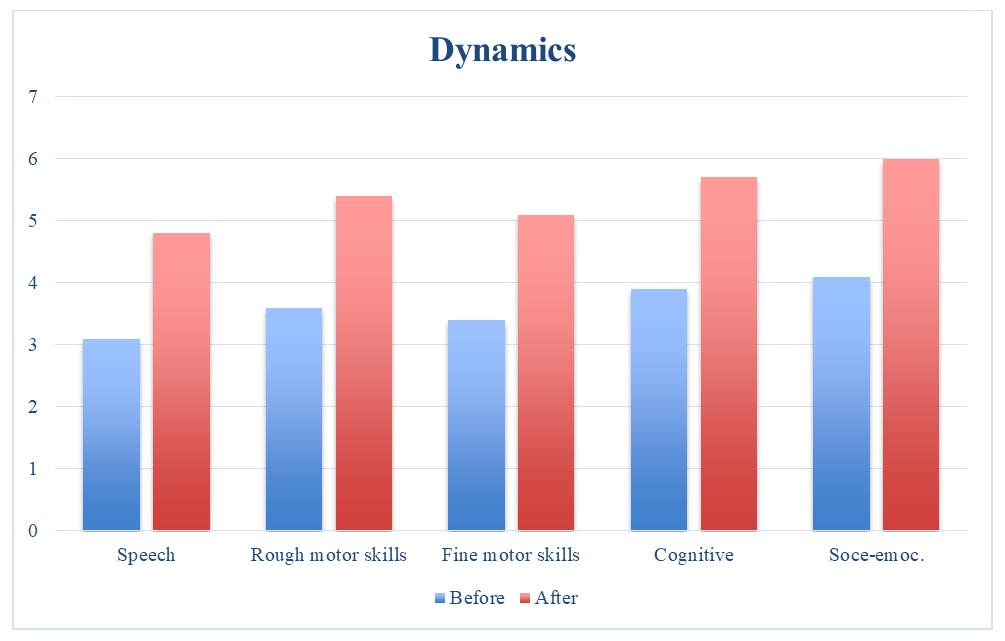 | Figure 1. Dynamics of average developmental indicators before and after CIPR (n=50) |
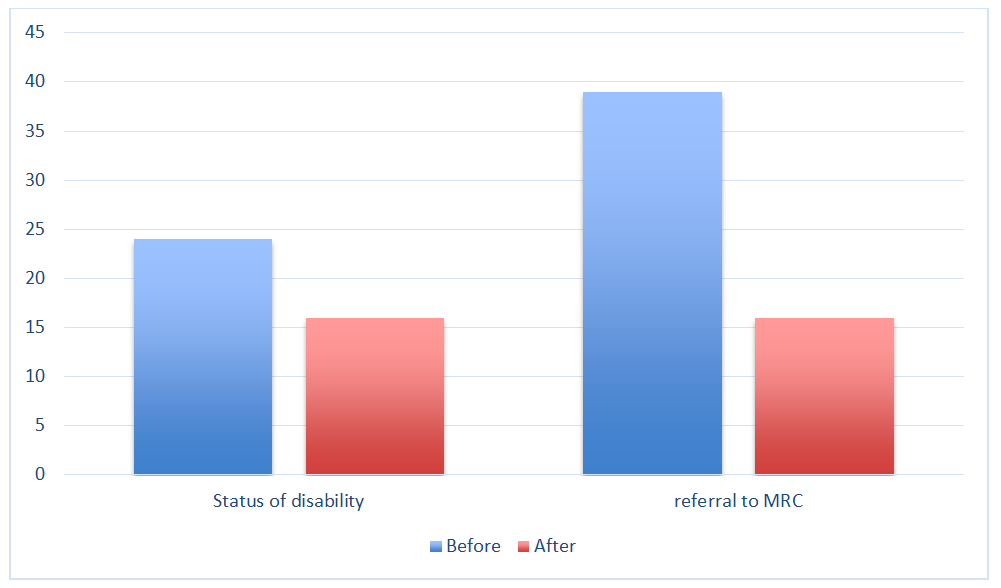 | Figure 2. Change in disability status and referrals to MRC before and after CIPR |
4. Discussion
- The findings indicate that, despite relatively high coverage of scheduled preventive examinations in early infancy, the use of standardized developmental assessment tools remains insufficient (58.9%). This gap can reduce the sensitivity of developmental surveillance and delay timely referral to early intervention services, which is inconsistent with international clinical approaches that emphasize routine surveillance supplemented by standardized screening when concerns are present.The regional CIPR model is designed to shorten the interval between identification of developmental concerns and initiation of structured support by combining interdisciplinary assessment, caregiver training, and follow-up monitoring. This design corresponds to widely used early childhood development frameworks that describe primary health care as a platform for early identification, coordinated support, and continuity of care in the first years of life.A more than two-fold reduction in referrals to the medical rehabilitation center (MRC) (from 40% to 16%) suggests a redistribution of care toward outpatient management. From a health system perspective, such a shift is aligned with the goal of rational allocation of rehabilitation resources provided that outpatient services are standardized, adequately staffed, and monitored for outcomes.At the same time, interpretation of the observed change in disability status (24% to 16%) should be cautious. In this study, the indicator reflects functional dynamics and repeated comprehensive assessment rather than a purely administrative correction. Given the pilot before-after design and the three-month observation period, alternative explanations (measurement variability, selection effects, short-term fluctuations) cannot be fully excluded.For further implementation, it is advisable to (a) formalize inclusion criteria for CIPR, (b) unify the assessment toolkit and scoring rules, and (c) strengthen intersector coordination across health care, education, and social protection. Multisector models are explicitly emphasized in contemporary early childhood development guidance as a condition for sustainable outcomes.
5. Conclusions
- The regional CIPR model demonstrated practical applicability for strengthening outpatient care and supporting disability prevention for children aged 0 to 3 years from risk groups. In the pilot group, the following changes were observed: an improvement in functional indicators by 1.7 to 1.9 score units, a reduction in the proportion of children with disability status from 24% to 16%, a decrease in referrals to the MRC from 40% to 16%, and high caregiver-reported satisfaction (90% fully satisfied). The model may be recommended for scaling, provided that unified assessment protocols, specialist training, and a result monitoring system are in place.