-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(5): 2637-2641
doi:10.5923/j.ajmms.20261605.77
Received: Apr. 23, 2026; Accepted: May 19, 2026; Published: May 27, 2026

Integrated Pathomorphological, Hematological and Immunohistochemical Assessment of Placental Circulatory Disorders in Pregnancy
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLErgasheva Dilyorakhon Islomjon kizi1, Shakirov Sardor Abdusaminovich2, Shokirova Sadokat Mukhammatsoliyevna3
1PhD., Associate Professor, Department of Pathological Physiology and Pathological Anatomy, Fergana Medical Institute of Public Health, Fergana, Uzbekistan
2Professor, Department of Obstetrics and Gynecology, Andijan State Medical Institute, Andijan, Uzbekistan
3DSc., Department of Obstetrics and Gynecology, Andijan State Medical Institute, Andijan, Uzbekistan
Correspondence to: Shakirov Sardor Abdusaminovich, Professor, Department of Obstetrics and Gynecology, Andijan State Medical Institute, Andijan, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Placental circulatory disorders are associated with impaired uteroplacental and fetoplacental exchange and contribute to adverse perinatal outcomes. This study assessed structural, hematological and immunohistochemical changes in placental tissue at 11, 23 and 30 weeks of gestation. Histological, morphometric, hematological and immunohistochemical methods were used to evaluate villous parameters, fibrinoid deposition, blood indices and CD31, CD34, VEGFR and CD95 expression. Placental dysfunction was characterized by villous remodeling, increased capillarization and fibrinoid deposition, decreased hemoglobin and erythrocytes, elevated platelets and fibrinogen, and gestational differences in VEGFR and CD95 expression. Combined morphometric, hematological and immunohistochemical assessment may serve as an additional diagnostic approach for placental circulatory pathology.
Keywords: Placenta, Placental insufficiency, Uteroplacental circulation, Morphometry, Hematology, Immunohistochemistry, CD31, CD34, VEGFR, CD95, Perinatal complications
Cite this paper: Ergasheva Dilyorakhon Islomjon kizi, Shakirov Sardor Abdusaminovich, Shokirova Sadokat Mukhammatsoliyevna, Integrated Pathomorphological, Hematological and Immunohistochemical Assessment of Placental Circulatory Disorders in Pregnancy, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2637-2641. doi: 10.5923/j.ajmms.20261605.77.
Article Outline
1. Introduction
- Placental circulatory disorders remain a major problem in obstetrics, perinatology and pathological anatomy. [1,2] The placenta is the principal functional interface of the mother-placenta-fetus system, providing gas exchange, trophic support, endocrine regulation and immunobiological protection. Therefore, impaired placental hemodynamics may lead to structural and functional insufficiency of placental tissue and contribute to fetal hypoxia, fetal growth restriction, preterm birth, intranatal asphyxia and perinatal loss. [3,4,7]Modern placental pathology does not regard morphological findings as isolated descriptive changes. [6,8,9] Current consensus approaches interpret placental lesions as tissue equivalents of defined pathogenetic processes, including maternal vascular malperfusion, fetal vascular malperfusion, inflammatory injury, immune-mediated injury, hypoxia, endothelial dysfunction and abnormal villous maturation. This approach is especially relevant when clinical, laboratory and morphological data are assessed together. [10,11,12] Endothelial injury, impaired angiogenesis and apoptosis are central mechanisms of placental dysfunction. CD31 and CD34 are commonly used to assess endothelial structures and vascular density. VEGFR reflects angiogenic responsiveness and vascular adaptation under hypoxic or ischemic conditions. CD95 is associated with apoptosis-related pathways and may indicate increased cellular turnover and tissue remodeling. [13,14,15] In parallel, hematological and coagulation parameters may reflect systemic maternal adaptation or decompensation in placental insufficiency.The aim of this study was to evaluate the pathomorphological, hematological and immunohistochemical features of placental circulatory disorders at 11, 23 and 30 weeks of gestation and to determine their diagnostic relevance for assessing placental dysfunction. [16,17]
2. Materials and Methods
- The study was devoted to the pathomorphological and hematological aspects of placental circulatory pathology. The material included placental tissue samples and peripheral blood samples from pregnant women. The analysis was organized according to three gestational observation points: 11, 23 and 30 weeks.At 11 weeks, the material was interpreted as reflecting early placental morphogenesis, trophoblast invasion, initial angiogenesis and early morphogenetic signs of possible subsequent uteroplacental dysfunction. At 23 and 30 weeks, placental changes were analyzed in relation to more mature uteroplacental and fetoplacental circulation and were compared with clinical and laboratory indicators.Histological examination was performed to assess villous architecture, stromal changes, vascularization, fibrinoid deposition and necrobiotic alterations. Histochemical staining was used to evaluate connective tissue remodeling and fibrinoid changes. Morphometric assessment included villous size, the number of villi per 1 mm², the number of capillaries per villus, the percentage area of fibrinoid deposits, placental weight, placental diameter and placental thickness.Hematological assessment included erythrocyte count, hemoglobin level, platelet count, fibrinogen concentration and hematocrit. Immunohistochemical examination was performed using CD31, CD34, VEGFR and CD95 markers. Quantitative evaluation included the total number of evaluated cells, the number of positive cells, the number of negative cells and the percentage of positive cells.
3. Results
3.1. Morphometric Characteristics of Placental tissue
- Morphometric data showed dynamic structural remodeling of placental tissue across the studied gestational periods. Villous size decreased from 116.2 ± 4.6 µm at 11 weeks to 53.8 ± 2.4 µm at 30 weeks. At the same time, villous density increased from 43.8 ± 2.3 to 87.6 ± 3.9 villi per 1 mm², and the number of capillaries per villus increased from 3.5 ± 0.3 to 6.6 ± 0.5. Fibrinoid deposits also increased from 4.8 ± 0.7% to 14.5 ± 1.3%, suggesting progressive vascular and stromal remodeling under conditions of circulatory stress.
|
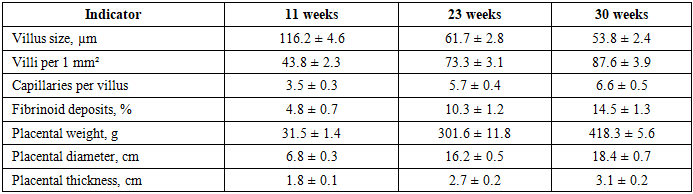
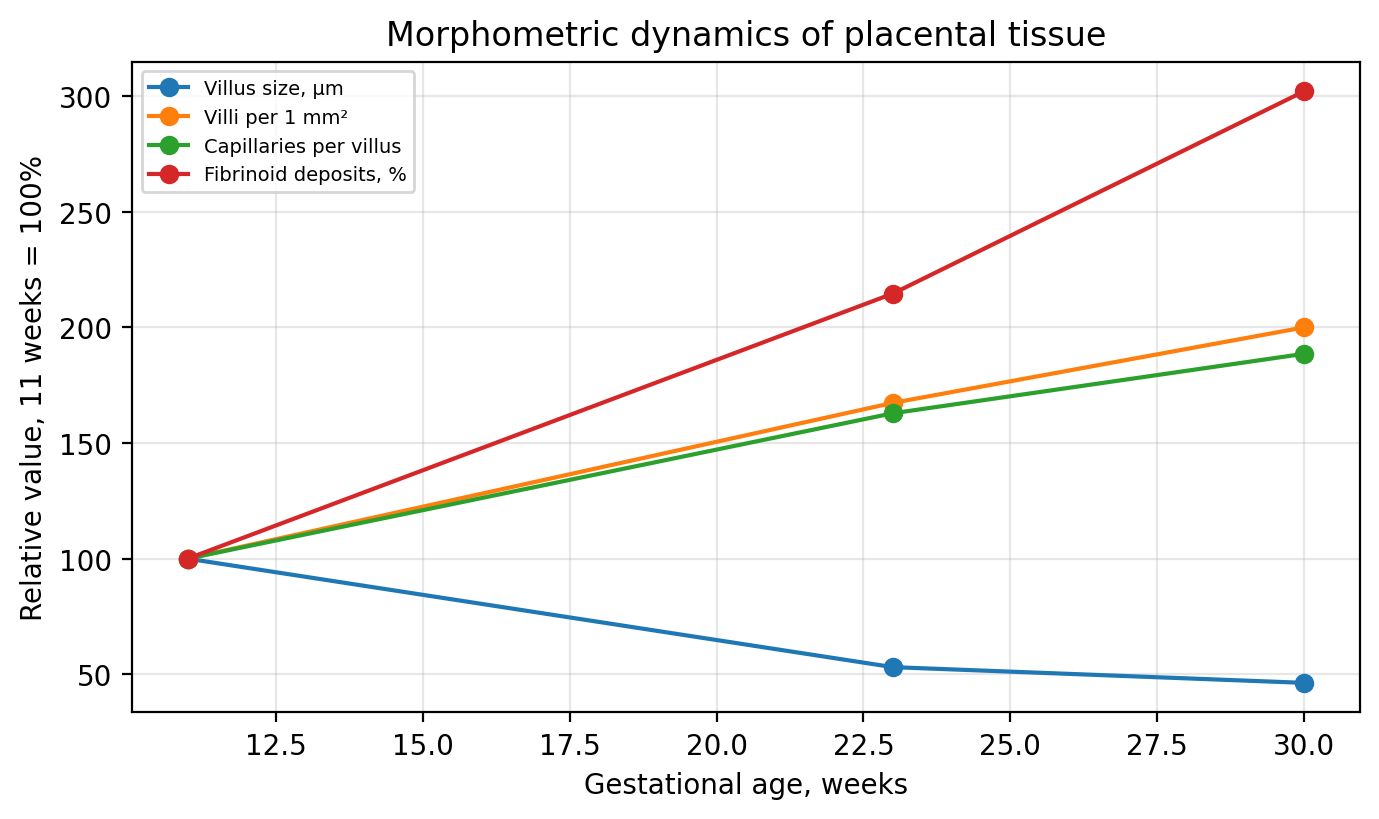 | Figure 1. Relative morphometric dynamics of placental tissue at 11, 23 and 30 weeks of gestation |
3.2. Hematological Changes
- The hematological profile demonstrated a pattern consistent with systemic maternal involvement in placental circulatory pathology. In the main group, erythrocyte count and hemoglobin were lower than in controls at all studied periods. The most pronounced decrease was observed at 30 weeks, where hemoglobin was 96 ± 0.6 g/L in the main group compared with 111 ± 1.4 g/L in controls. Platelet count and fibrinogen concentration were higher in the main group, indicating activation of hemostatic and coagulation-related mechanisms.
|
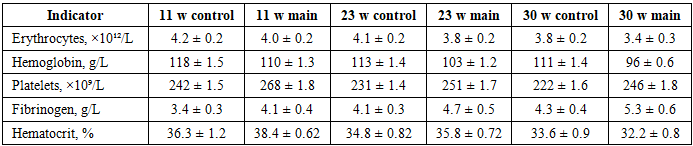
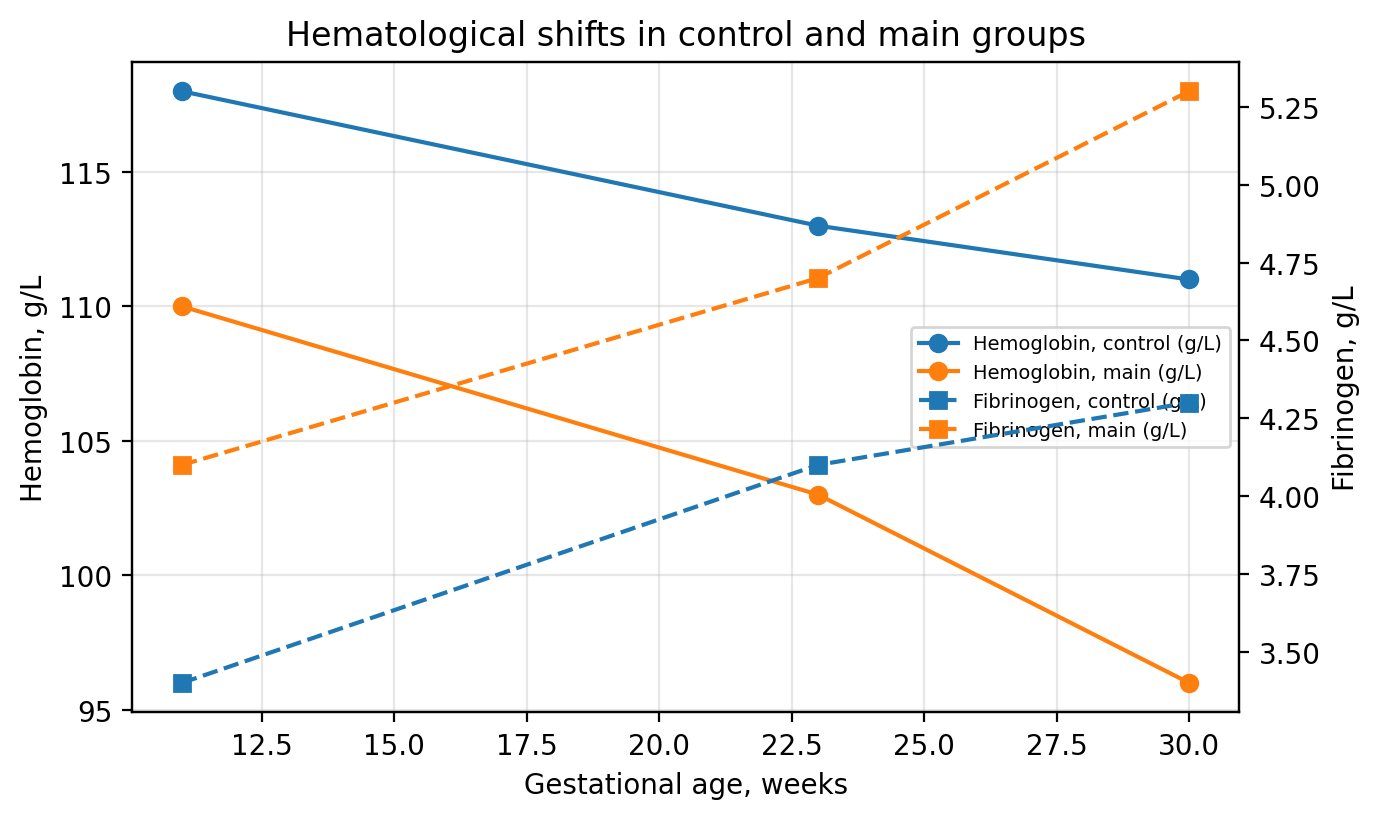 | Figure 2. Hemoglobin and fibrinogen changes in the control and main groups |
3.3. Immunohistochemical Profile
- Immunohistochemical assessment showed high expression of endothelial markers CD31 and CD34 throughout the studied gestational periods. CD31-positive cells accounted for 90.7%, 89.5% and 88.9% at 11, 23 and 30 weeks, respectively. CD34 positivity was 87.8%, 85.2% and 84.0%. VEGFR expression showed marked gestational variation, with a decrease at 23 weeks and renewed elevation at 30 weeks. CD95 positivity was 72.2% at 11 weeks, 58.1% at 23 weeks and 63.5% at 30 weeks, reflecting apoptosis-associated remodeling of placental tissue.
|
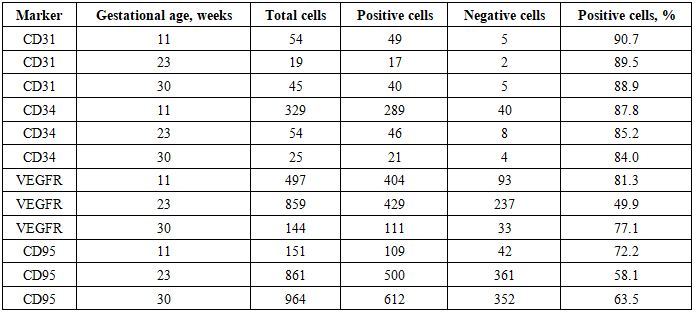
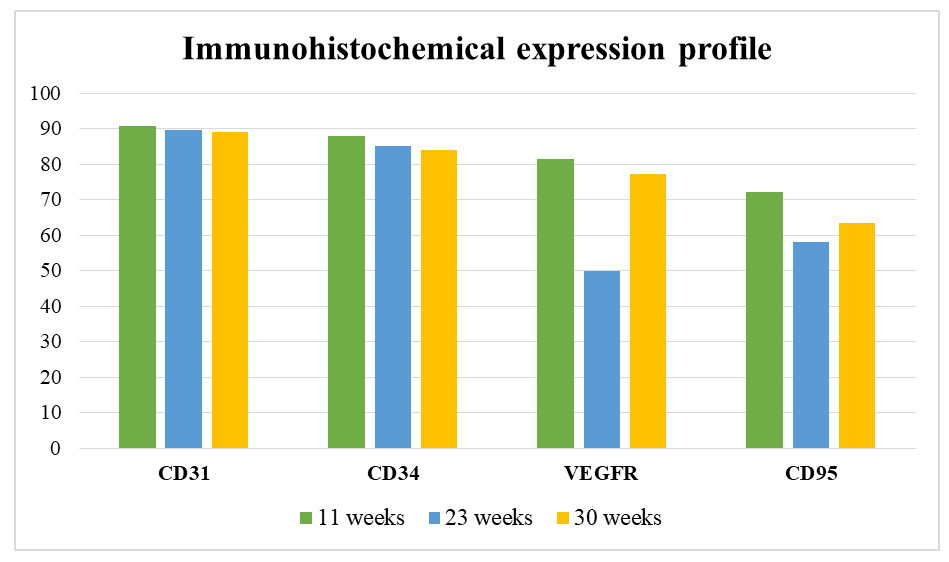 | Figure 3. Percentage of positive cells for CD31, CD34, VEGFR and CD95 |
4. Discussion
- The obtained findings demonstrate that placental circulatory pathology is reflected not by a single isolated sign but by a complex constellation of tissue, vascular, hematological and immunohistochemical changes. The reduction in villous size together with increased villous density and capillarization may be interpreted as a manifestation of adaptive villous remodeling. This response is directed at maintaining exchange surface area and compensating for reduced uteroplacental perfusion.The simultaneous expansion of fibrinoid deposits indicates that adaptation is accompanied by stromal and vascular injury. Excess fibrinoid deposition may impair intervillous exchange and reduce placental reserve capacity. In this context, morphometric assessment is diagnostically important because it objectifies structural remodeling and allows comparison between gestational stages.Hematological findings support the concept that placental circulatory disorders are associated with systemic maternal changes. Lower erythrocyte and hemoglobin values in the main group may aggravate fetal oxygen deficiency. Increased platelet count and fibrinogen concentration indicate a shift toward hemostatic activation. Such changes are consistent with the pathophysiology of endothelial dysfunction, microcirculatory injury and placental malperfusion.The immunohistochemical data refine this interpretation. High CD31 and CD34 expression indicates preserved but actively remodeled endothelial and microvascular structures. VEGFR variation may reflect changes in angiogenic demand under hypoxic stress. The pattern of CD95 expression suggests that apoptosis-associated mechanisms participate in placental adaptation and injury. Therefore, the combined use of endothelial, angiogenic and apoptosis-related markers provides more informative diagnostic interpretation than isolated morphological assessment.The study has practical implications for pathological anatomy and obstetric care. A combined assessment of villous morphology, fibrinoid deposition, maternal hematological profile and immunohistochemical markers may improve recognition of placental dysfunction and support identification of pregnancies at increased risk of adverse perinatal outcomes. The approach is also useful for retrospective analysis of complicated pregnancies and for developing standardized diagnostic-prognostic criteria.
5. Conclusions
- Placental circulatory disorders are characterized by coordinated pathomorphological, hematological and immunohistochemical changes. The main morphometric features include reduced villous size, increased villous density and capillarization, and progressive fibrinoid deposition.In the main group, the hematological profile was characterized by lower erythrocyte and hemoglobin values and higher platelet and fibrinogen levels compared with controls, indicating the involvement of oxygen transport and hemostatic mechanisms.CD31 and CD34 expression reflected endothelial and microvascular remodeling, whereas VEGFR and CD95 characterized angiogenic stress and apoptosis-associated tissue reorganization.Integrated assessment of placental morphology, maternal hematological parameters and immunohistochemical markers may be used as an additional diagnostic approach for early identification of placental dysfunction.