-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(5): 2632-2636
doi:10.5923/j.ajmms.20261605.76
Received: Apr. 29, 2026; Accepted: May 22, 2026; Published: May 27, 2026

Features of the Immune Response and Clinical Course of Community-Acquired Pneumonia in Children with Congenital Heart Defects
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAzizova N. D.1, Andapulatov A. A.2, Shamsiev F. M.3
1Doctor of Medical Sciences, Department of Pulmonology, Republican Specialized Scientific and Practical Medical Center of Pediatrics of the Ministry of Health of the Republic of Uzbekistan
2Сlinical and Diagnostic Characteristics in Children with Congenital Heart Defects and Pneumonia of the Ferghana Region Republic of Uzbekistan
3Doctor of Medical Sciences, Professor, Head of the Department of Pulmonology, Republican Specialized Scientific and Practical Medical Center of Pediatrics of the Ministry of Health of the Republic of Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Congenital heart defects remain one of the leading causes of morbidity, disability, and mortality in children worldwide. The presence of congenital cardiovascular abnormalities significantly increases the risk of infectious and inflammatory complications, particularly community-acquired pneumonia, which is characterized by a severe clinical course and high probability of adverse outcomes. This article is devoted to the study of the features of the immune response and the clinical manifestations of community-acquired pneumonia in children with congenital heart defects. A prospective clinical study included 140 children aged from 0 to 3 years who underwent treatment at the Republican Specialized Scientific and Practical Medical Center of Pediatrics and the Regional Children’s Multidisciplinary Medical Center of Fergana. The study assessed clinical symptoms, anamnestic data, laboratory and instrumental parameters, as well as indicators of cellular and humoral immunity. Special attention was paid to the analysis of cytokine status, including the determination of serum levels of TNF-α, IL-1β, IL-4, IL-6, IL-8, and IFN-γ using enzyme-linked immunosorbent assay. The obtained results demonstrated that community-acquired pneumonia in children with congenital heart defects is accompanied by a more severe clinical course characterized by respiratory failure, prolonged intoxication syndrome, severe dyspnea, cyanosis, myocardial dysfunction, and significant hemodynamic disturbances. The majority of hospitalized patients were children of the first year of life, among whom ventricular septal defect, atrial septal defect, and Tetralogy of Fallot predominated. Echocardiographic examination revealed a decrease in myocardial contractility, enlargement of heart chambers, increased pulmonary artery pressure, and more frequent occurrence of pericardial effusion in children with combined pathology.
Keywords: Congenital heart defects, Community-acquired pneumonia, Children, Immune response, Cytokines, Inflammatory process, Hemodynamic disorders, TNF-α, IL-6, IL-8, IL-1β, Immunoregulation, Respiratory failure
Cite this paper: Azizova N. D., Andapulatov A. A., Shamsiev F. M., Features of the Immune Response and Clinical Course of Community-Acquired Pneumonia in Children with Congenital Heart Defects, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2632-2636. doi: 10.5923/j.ajmms.20261605.76.
Article Outline
1. Introduction
- Despite modern advances in cardiology and cardiac surgery, congenital heart defects remain a frequent cause of disability and mortality in childhood and include a wide range of phenotypes that differ in morphology, physiology, and other factors, which necessitates a differentiated study of the mechanisms underlying the development of this pathology. Congenital malformations are the most common pathology among newborns, one-third of which are congenital heart defects (CHD). In Uzbekistan, about 10 thousand children with CHD who require surgery are born annually. Of these, from 50 to 70% require emergency care. [1,2] Mortality in such CHDs is extremely high: by the end of the first week, 29% die; by the first month, 42%; by the first year of life, 87%; by the first month, 42%; by the first year of life, 87%. The study of the incidence rate, types of CHD, as well as risk factors for their development may serve as a basis for the development of therapeutic and preventive programs aimed at reducing this pathology in the region. Moreover, a further increase in the prevalence of CHD is predicted. The increase in the proportion of children with CHD is also facilitated by modern surgical treatment methods, which ensure the survival of children with almost all defects and, as a consequence, the rapid growth of the population of adolescents and adults with operated CHD. [3,4]The article examines the features of the immune response and the clinical course of community-acquired pneumonia in children with congenital heart defects. Changes in the indicators of cellular and humoral immunity, as well as their relationship with the severity of the disease, duration of the course, and outcomes, are analyzed. Particular attention is paid to the role of immune dysfunction in the development of complicated forms of pneumonia. [5,6,9]The obtained data make it possible to deepen the understanding of the pathogenetic mechanisms of the disease in this category of patients and can be used to optimize diagnosis, predict the course of the disease, and determine treatment strategies. [10,11,12]Objective of the study: To investigate the features of the immune response and the clinical course of community-acquired pneumonia in children with congenital heart defects in order to identify factors influencing the severity of the disease and the development of complications.
2. Materials and Methods of the Study
- In accordance with the objectives set, we conducted a prospective study of 140 children with congenital heart defects (CHD) and community-acquired pneumonia who were treated at the Republican Specialized Scientific and Practical Medical Center of Pediatrics and at the Regional Children’s Multidisciplinary Medical Center of Fergana. The children were aged from 0 to 3 years, including 60 patients with CHD and 60 children with CHD and community-acquired pneumonia (comparison group). All children with CHD admitted to the RSSPMC of Pediatrics were registered with a cardiac surgeon. The reason for admission to the RSSPMC of Pediatrics was a sharp deterioration in the child’s condition, weakness accompanied by dyspnea, severe anxiety, cyanosis of the skin, and increased body temperature. Clinical and anamnestic data, chest X-ray results, and laboratory parameters were taken into account. Immunological studies were also performed. The quantitative levels of cytokines – IL-1β, IL-4, IL-6, IL-8, TNF-α, and IFN-γ in blood serum were determined by enzyme-linked immunosorbent assay using the semi-automatic immunoassay analyzer “Multiskan FC” (Finland).
3. Results and Discussion
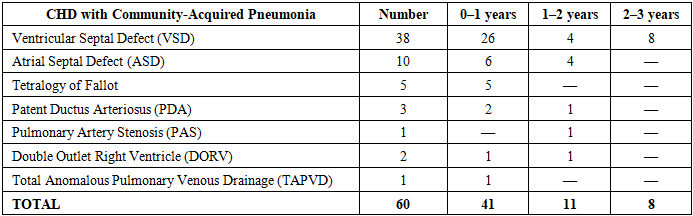
- In children of the CHD group, the following were observed: ventricular septal defect (VSD) in 16 children, including 12 aged 0–1 year, 3 aged 1–2 years, and 1 child aged 2–3 years; atrial septal defect (ASD) in 20 children, including 10 aged 0–1 year, 6 aged 1–2 years, and 4 aged 2–3 years. Tetralogy of Fallot (TOF) was identified in 11 children, including 9 aged 0–1 year, 1 child aged 1–2 years, and 1 child aged 2–3 years.As can be seen from the table, among the majority of children with CHD and community-acquired pneumonia, ventricular septal defect (VSD) was the most common and was observed most frequently in children under 1 year of age – 26 children (43.3%). At the age of 1–2 years, there were 4 children (6.7%), and at the age of 2–3 years – 8 children (13.3%). Atrial septal defect (ASD) was diagnosed less frequently — in 10 children (16.7%), and Tetralogy of Fallot — in 5 patients (8.3%). Other forms of CHD with community-acquired pneumonia occurred only in isolated cases (Table 1).
|
|
|
4. Conclusions
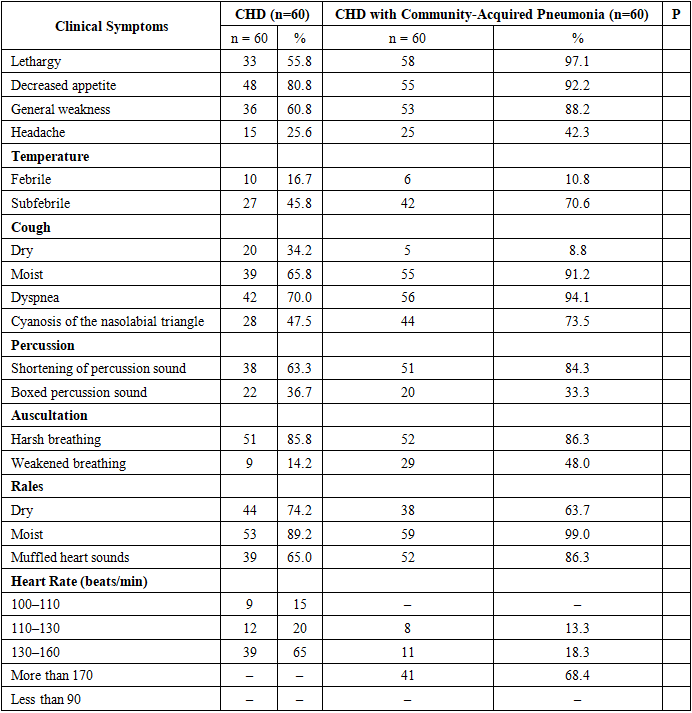
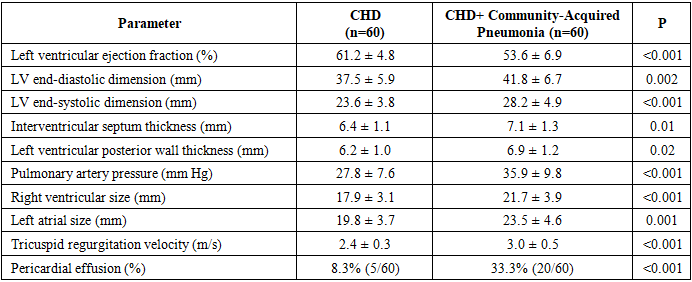
- 1. In children with congenital heart defects, community-acquired pneumonia is characterized by a more severe clinical course accompanied by pronounced respiratory failure, intoxication syndrome, and a high frequency of hospitalization in severe condition. In the structure of congenital heart defects among the examined patients, ventricular septal defect, atrial septal defect, and Tetralogy of Fallot predominated, while children of the first year of life represented the most vulnerable group. 2. The addition of community-acquired pneumonia in children with CHD leads to a significant deterioration of hemodynamic parameters: a decrease in myocardial contractile function, enlargement of the heart chambers, increased pulmonary artery pressure, and a higher incidence of pericardial effusion. 3. Clinical and functional changes are accompanied by pronounced activation of the systemic inflammatory response, manifested by a significant increase in the levels of pro-inflammatory cytokines (TNF-α, IL-1β, IL-6, IL-8). 4. A disturbance of immune regulation was revealed, characterized by an imbalance between pro- and anti-inflammatory cytokines: against the background of increased IL-4 in isolated CHD, its relative decrease was observed when combined with pneumonia, indicating exhaustion of compensatory anti-inflammatory mechanisms. 5. A relationship was established between the severity of the cytokine response and the severity of the clinical course of the disease, confirming the significant role of immune disorders in the pathogenesis of community-acquired pneumonia in children with CHD. 6. The obtained data substantiate the need for early diagnosis, comprehensive assessment of immune status, and a differentiated approach to the treatment of this category of patients in order to reduce the risk of complications and mortality.