-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(5): 2626-2631
doi:10.5923/j.ajmms.20261605.75
Received: Apr. 21, 2026; Accepted: May 13, 2026; Published: May 27, 2026

Differential Diagnosis of Biliary Atresia and Other Causes of Neonatal Cholestasis: 10 Years of Clinical Experience
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLTuichiev Galibjon Urmonjonovich1, Nematjonov Farrukh Zokirjon ugli2, Aliev Mahmud Muslimovich3, Gofurov Adham Anvarovich4, Yuldashev Rustam Zafardjanovich5
1Andijan Branch of Kokand University, Associate Professor of the Candidate of Medical Science, Andijan, Uzbekistan
2Andijan State Medical Institute, Assistant of the Department of Pediatric Surgery, Andijan, Uzbekistan
3Tashkent Pediatric Medical Institute, Professor of the Department of Pediatric Surgery, Doctor of Medical Science, Tashkent, Uzbekistan
4Andijan State Medical Institute, Head of the Department of Pediatric Surgery, Doctor of Medical Science, Andijan, Uzbekistan
5Republican Specialized Scientific and Practical Medical Center of Pediatrics, PhD, DSC, Tashkent, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The purpose of the study: To evaluate diagnostic criteria for biliary atresia (BA) and other causes of neonatal cholestasis in children based on 10 years of clinical experience. Materials and methods: The retrospective study included 157 newborns and infants with signs of cholestasis who were hospitalized at the Republican Specialized Scientific and Practical Medical Center of Pediatrics (Tashkent) in 2013-2023. The diagnostic algorithm included ultrasound examination (ultrasound) of the abdominal organs, transient elastometry (TE) of the liver, as well as, according to indications, hepatobiliary scintigraphy and MRI with cholangiography. The diagnosis would have been surgically confirmed (by intraoperative cholangiography or liver biopsy) in 43 patients. In another 88 children, BA was regarded as suspected based on a combination of clinical, laboratory and imaging data. The remaining patients were diagnosed with other diagnoses unrelated to BA using a comprehensive examination, including genetic methods in some cases. Results: Suspected BA was detected in 131 patients (83.4%), of which 43 (32.8%) had their diagnosis surgically confirmed. The sign of a fibrous triangle on ultrasound was detected in 38.3%, gallbladder abnormalities — in 65.5% of cases; at the same time, in 35.8% of patients, the gallbladder was visualized as morphologically normal. The average cookie hardness according to the TE data in children with suspected BA was significantly higher than in other forms of cholestasis (p<0.05), especially in patients older than 90 days. In a sample of six patients who underwent scintigraphy, the absence of intestinal excretion of the radiopharmaceutical was noted in all; The diagnosis of BA was confirmed in four of them. MR cholangiography (n=12) revealed signs of cystic BA, cystic transformation of choledochus, and syndromic BA with polysplenia. Conclusion: The combination of ultrasound and transient elastometry improves the accuracy of early diagnosis of suspected biliary atresia. However, an integrated approach is of key importance, taking into account laboratory data and additional imaging methods, which makes it possible to distinguish BA from other causes of cholestasis in a timely manner and determine the optimal treatment strategy.
Keywords: Biliary atresia, Neonatal cholestasis, Ultrasound, Transient elastometry
Cite this paper: Tuichiev Galibjon Urmonjonovich, Nematjonov Farrukh Zokirjon ugli, Aliev Mahmud Muslimovich, Gofurov Adham Anvarovich, Yuldashev Rustam Zafardjanovich, Differential Diagnosis of Biliary Atresia and Other Causes of Neonatal Cholestasis: 10 Years of Clinical Experience, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2626-2631. doi: 10.5923/j.ajmms.20261605.75.
1. Introduction
- Biliary atresia (BA) is a rare but severe fibroobliterating biliary tract disease of unknown etiology that manifests itself in the neonatal period. According to various data, its frequency ranges from 1:5,000 to 1:22,000 newborns [1-7]. BA is the main cause of surgical (obstructive) cholestasis in infants and occupies a leading place among indications for liver transplantation in pediatrics [8]. Timely Kasai surgery (portoenteroanastomosis), preferably before the age of 60-90 days, significantly improves bile outflow, slows down the development of fibrosis, and reduces the likelihood of liver transplantation [9,10]. However, early diagnosis would pose a significant clinical challenge, both in resource-limited settings and in advanced healthcare systems. The main difficulty lies in the need to differentiate BA from other causes of neonatal cholestasis, such as idiopathic neonatal hepatitis, progressive familial intrahepatic cholestasis (FVC), Alajille syndrome, congenital liver fibrosis, cystic transformations of choledochus, as well as infections (for example, CMV) and metabolic diseases [10-15]. All of these conditions may have similar clinical manifestations: prolonged jaundice, acolic stools, and hepatomegaly. Among the biochemical markers of cholestasis, elevated levels of direct bilirubin, gamma-glutamyltransferase (GGT), and alkaline phosphatase are of particular importance, but they are not specific and require interpretation in combination with imaging data [13]. Ultrasound examination (ultrasound) of the abdominal organs remains the main method of primary diagnosis [16-18]. It allows you to assess the shape and size of the gallbladder, the presence of signs of a "fibrous triangle" in the gate of the cookie, and also exclude other abnormalities in the development of the biliary tract. However, the sensitivity and specificity of ultrasound depends on the specialist's experience and can be reduced in the early stages of the disease. Additional information is provided by magnetic resonance cholangiopancreatography (MRCPG) and hepatobiliary scintigraphy, but the availability of these methods is often limited, especially in countries with limited resources [19]. In recent years, the method of transient elastometry (TE) has been actively introduced, which allows noninvasively assessing the stiffness of cookies as an indirect sign of the severity of fibrosis [20,21]. Given the rapid progression of fibrosis in BA, TE can serve as an additional diagnostic tool. It is assumed that the combination of ultrasound and elastometry increases the accuracy of early detection of BA and allows timely referral of the patient for surgical intervention. However, there is still insufficient data on the diagnostic effectiveness of this approach in conditions of limited resources. In this regard, the purpose of this study is to evaluate the informative value of ultrasound of the abdominal cavity and transient liver elastometry in the early diagnosis of suspected biliary atresia in children with neonatal cholestasis based on 10 years of experience.
2. Materials and Methods
- Sample design and characteristicsA retrospective study was conducted covering the period from January 2013 to December 2023. The analysis included 157 newborns and infants (<6 months) with signs of neonatal cholestasis — acholic stools and conjugated hyperbilirubinemia. All patients were hospitalized at the Republican Specialized Scientific and Practical Medical Center of Pediatrics (Tashkent). The initial examination and ultrasound screening were conducted in two regional institutions, after which the patients were sent to a specialized center for further examination and verification of the diagnosis.Diagnostic algorithmsAll patients underwent a standard biochemical evaluation, including the measurement of alanine aminotransferase (ALT), aspartate aminotransferase (AST), total and direct bilirubin, gamma-glutamyl transferase (GGT), alkaline phosphatase (ALP), albumin, fibrinogen, and the international normalized ratio (INR). These parameters were used to assess hepatocellular injury, cholestasis, and the synthetic function of the liver.In cases of suspected cytomegalovirus infection, serological testing (IgM/IgG) was performed, along with polymerase chain reaction (PCR) when indicated.Ultrasound examination of the abdominal organs was performed in all patients. The size and morphology of the gallbladder (presence, length, shape, wall), the presence of signs of a "fibrous triangle" in the gate of the cookie, the condition of the extrahepatic bile ducts, the structure of the cookie, the presence of ascites, the size of the spleen and its possible anomalies were evaluated. Signs of portal hypertension (splenomegaly, collaterals) were taken into account [18].Transient elastometry of cookies (TE) (FibroScan) was performed according to the indications in patients without signs of ascites, since the presence of free fluid in the abdominal cavity prevents reliable registration of tissue elasticity. The measurements were performed using a specialized children's S-probe (Small probe) sensor designed for patients with a body weight of less than 10-15 kg, which allowed us to obtain valid values of cookie hardness in infants. The obtained values of cookie elasticity were considered as an additional guideline for complex diagnostics, without using strict threshold criteria.Scintigraphy with TC-99m-labeled radiopharmaceutical was performed selectively with questionable ultrasound and/or elastometry results. The main diagnostic criterion in favor of BA was considered to be the absence of imaging of the radiopharmaceutical in the intestine for 24 hours.Magnetic resonance imaging (MRI) of the abdominal organs with cholangiography (MRCPG) was performed in patients with suspected biliary tract abnormalities, cystic forms of BA, syndromic variants (for example, with polysplenia), vascular abnormalities. The method made it possible to visualize the anatomy of the bile ducts and assess the accompanying changes.In some cases, depending on the clinical picture, additional chest X-rays were performed (to detect spinal abnormalities), echocardiography (to diagnose congenital heart defects), as well as genetic studies, especially in cases of suspected Alajille syndrome or progressive familial intrahepatic cholestasis. The conduct of these examinations depended on the availability of the method and clinical feasibility.Diagnostic criteria• Confirmed biliary atresia (n = 43): the diagnosis was established based on intraoperative cholangiography and/or histological findings from a liver biopsy taken during Kasai surgery.• Suspected biliary atresia (n = 88): the diagnosis was made in the presence of stable cholestasis in combination with characteristic ultrasound signs (absence or hypoplasia of the gallbladder, a symptom of a "fibrous triangle"), high cookie stiffness with transient elastometry (>20 kPa), lack of intestinal excretion of radiopharmaceutical with scintigraphy (if present), and also when other causes of cholestasis are excluded.• Cholestasis of other etiology (n = 26): diagnoses in this group were established on the basis of clinical laboratory and imaging data. In particular, Alajil syndrome was diagnosed in the presence of ≥3 of the following signs: abnormalities of the vertebral bodies (of the "butterfly" type), congenital heart defects, posterior embryotoxin, characteristic facial features, if present, confirmation of mutations in the JAG1/NOTCH2 genes. Progressive familial intrahepatic cholestasis (FVC) — the diagnosis was based on the clinical picture and biochemical data (including GGT levels); genetic confirmation was carried out selectively. Neonatal and CMV hepatitis were verified according to a set of clinical and laboratory criteria. Cystic transformation of the choledochus (CT) - confirmed by ultrasound, MRI or MSCT (in cases of dilation of the extrahepatic and intrahepatic bile ducts).The data was analyzed using IBM SPSS Statistics software, version 23. Quantitative variables with a normal distribution are presented as the mean and standard deviation (m ± SD). The parameters were compared between groups of patients with suspected BA and with cholestasis of other etiology using the Student's t-test for independent samples. The differences at the p < 0.05 level were considered statistically significant. The relationship between the quantitative variables was assessed using the Pearson correlation coefficient.
3. Results
- The study included 157 newborns and infants with neonatal cholestasis examined between 2013 and 2023. According to the results of the comprehensive diagnosis, BA was confirmed or regarded as suspected in 131 patients (83.4%; group I), of which 43 children had the diagnosis verified intraoperatively. Other causes of cholestasis were found in 26 patients (16.6%; group II). The average age of diagnosis would have been 84.3 ± 3.0 days; only 15% of the children were examined before the age of two months. In patients with cholestasis of a different etiology, the age at the time of admission was significantly higher (p = 0.01). The sex composition of the groups did not differ statistically.The etiology of cholestasis in group II (n = 26) was distributed as follows: Alazhil syndrome was diagnosed in 12 cases, cystic transformation of choledochus in 4 patients, neonatal hepatitis (including CMV infection) in 4 cases, progressive familial intrahepatic cholestasis (FVC) in 3, congenital liver fibrosis. in 2 cases, and Beckwith—Wiedemann syndrome in 1 case. Alajil syndrome was manifested by a typical clinical picture of neonatal cholestasis in combination with butterfly-type vertebral body abnormalities (according to thoracic radiography), heart defects (tetrad of Fallot, pulmonary artery stenosis), posterior embryotoxon (ophthalmologically) and characteristic facial features. Genetic confirmation of the diagnosis was carried out selectively. CT scan was the cause of cholestasis in four patients. She was characterized by episodic acholia, a transient increase in enzyme levels, and clinical improvement with the use of ursodeoxycholic acid. Differentiation with the cystic form of AD was carried out using ultrasound and MR cholangiography: CT scans visualized large cysts of the intrahepatic and intrahepatic ducts, whereas with cystic ad, a small isolated formation in the gates of the cookie. The use of color Doppler mapping (CDMA) made it possible to exclude the vascular nature of the formation (Fig. 1).
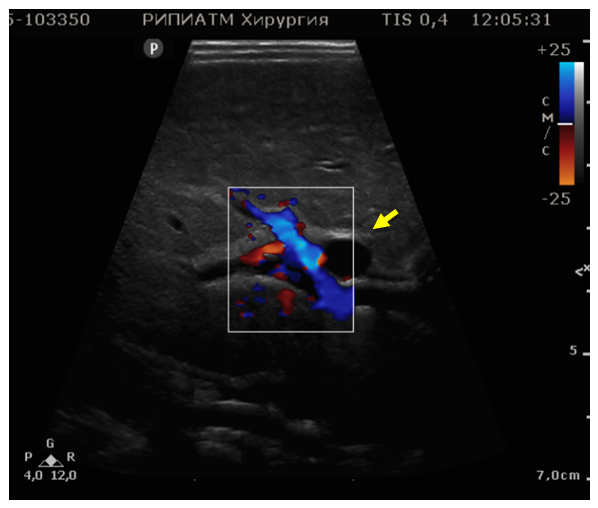 | Figure 1. Echotomogram of a 65-day-old child with cystic BA, a cystic formation is detected in the projection of the right branch of the portal vein (yellow arrow) 0.5*0.6 cm |
 | Figure 2. Echotomogram of a 55-day-old child with BA, determined by hypoplasticized veins, without a clear contour of the mucous membrane |
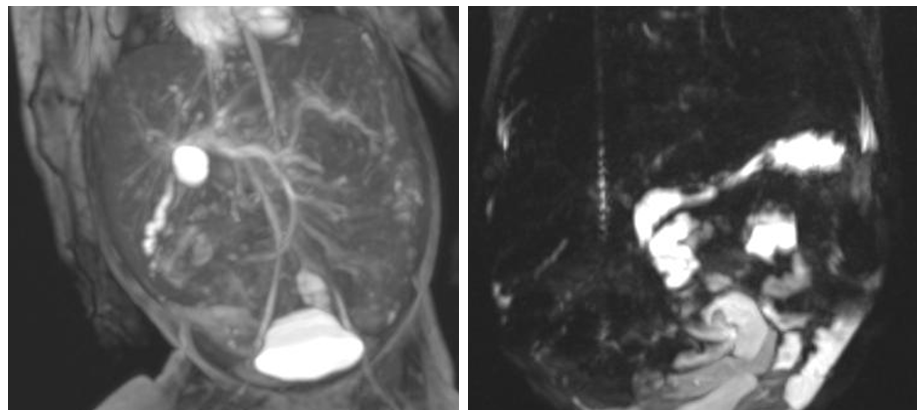 | Figure 3. MRI cholangiography A-direct projection, contrast-free cholangiography MIP reconstruction, cystic formation and deformed LC contrast in the cookie gate. B – MRI cholangiogram, direct projection of MIP reconstruction-LC, external and intrahepatic HDL are not contrasted |
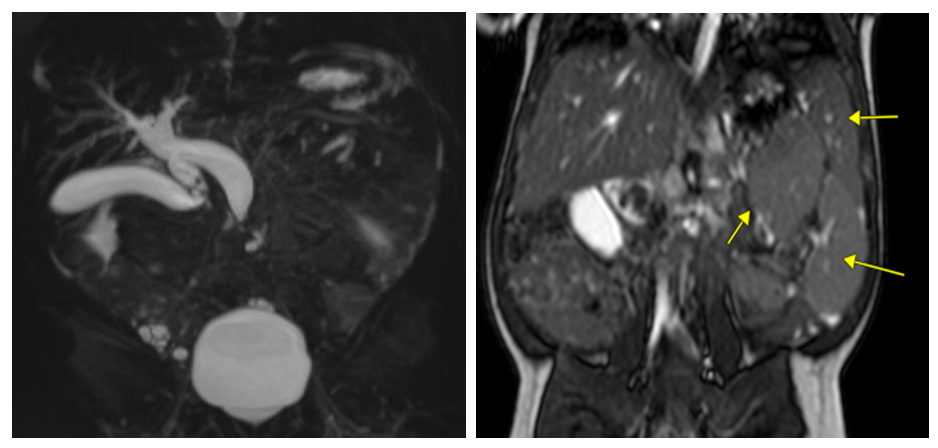 | Figure 4. On an A-MRI with contrast-free cholangiography in a child with cystic transformation of the choledochus, a fusiform expansion of the choledochus with heterogeneous contents in the projection of the cystic duct is noted. B-MRI, T2 weighted image, arrows indicate 3 spleens (polysplenia) |
4. Discussion
- The results of this study confirm that BA remains the leading cause of neonatal cholestasis, which is consistent with the data from the world literature indicating its key role in the structure of obstructive jaundice in newborns [7]. One of the strong aspects of the study is the use of a comprehensive non—invasive diagnostic approach, including ultrasound, transient elastography, and, if necessary, scintigraphy and MR cholangiography. Ultrasound proved to be useful as a screening method, but its sensitivity was limited: the sign of a "fibrous triangle" was detected in less than 40% of patients with BA, and a normal-shaped gallbladder was visualized in more than a third of children with confirmed pathology. These data confirm the well-known dependence of ultrasound accuracy on the researcher's qualifications and the patient's age [16].The use of TE increased diagnostic accuracy, especially in children over 90 days of age, who were found to have significantly increased cookie stiffness. However, the interpretation of these data requires caution: the severity of inflammation, the level of bilirubin, and the degree of cytolysis may affect the stiffness values. Despite a moderate correlation with the level of GGT, TE did not show strong links with other biochemical markers, which limits its independent prognostic value. MR cholangiography has demonstrated high informative value in complex differential diagnostic cases, primarily in distinguishing between the cystic form of BA and the cystic transformation of the choledochus. In addition, the method proved useful for detecting concomitant anomalies (for example, polysplination). However, the high cost, limited availability and the need for sedation in newborns are holding back its widespread adoption, especially in countries with limited resources.Scintigraphy showed high sensitivity, however, as previously reported, the specificity of the method is limited: in our study, two out of six patients with no intestinal excretion of the BA isotope were not confirmed. This highlights the need to use scintigraphy strictly according to indications and only in combination with other imaging techniques.It is noteworthy that not all patients with suspected BA had their diagnosis surgically confirmed. This is due, firstly, to the late treatment - most patients were admitted older than 90 days, when, in our clinical opinion, performing Kasai surgery was no longer considered rational [22]. Secondly, in some cases, parents informed of the prognosis refused surgical intervention, preferring delayed primary liver transplantation. These factors should be taken into account when interpreting the results, as some cases remain without morphological verification. Also noteworthy is the relatively high proportion of Alajil syndrome among non-BA cholestasis (46.1%), which probably reflects an improvement in regional diagnosis, including the use of radiography, echocardiography, and ophthalmological examination. Genetic verification was carried out selectively, which is another limitation of the study. Similarly, in progressive familial intrahepatic cholestasis (FVC), the diagnosis was based primarily on clinical and laboratory data; molecular genetic diagnosis was not available in all cases. General limitations include the retrospective design, uneven examination (not all methods were available to all patients), as well as a relatively small number of observations in the non-BA group, which affects the statistical assessment of rare forms of cholestasis.In general, the presented study highlights the relevance of an integrated approach to the diagnosis of BA and demonstrates that the combination of ultrasound and TE can serve as an effective basis for a non-invasive diagnostic algorithm. A promising direction should be considered the development and validation of unified diagnostic protocols for countries with limited resources, as well as the introduction of early screening programs to control the stool color of newborns, which have proven effective in other countries.
5. Conclusions
- Biliary atresia remains the main cause of neonatal cholestasis in Uzbekistan. The combination of ultrasound and transient elastography demonstrates high diagnostic value, especially in children over 90 days of age. However, the limited sensitivity of ultrasound and the variability of TE data require an integrated approach using additional imaging techniques. The lack of surgical verification in some patients is associated with late treatment and refusal of surgery in favor of delayed liver transplantation. The results highlight the need for early detection of BA, standardization of diagnostic algorithms, and improved access to specialized care in resource-limited settings.