-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(5): 2621-2625
doi:10.5923/j.ajmms.20261605.74
Received: Apr. 26, 2026; Accepted: May 20, 2026; Published: May 25, 2026

The Role of Subclinical Thyroid Pathology in Female Infertility: Optimization of Early Diagnosis and Intervention
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMuratova Dilafruz Iskandar qizi
PhD Base Doctoral, Department of Obstetrics and Gynecology, Faculty of Postgraduate Education, Samarkand State Medical University, Samarkand, Uzbekistan
Correspondence to: Muratova Dilafruz Iskandar qizi, PhD Base Doctoral, Department of Obstetrics and Gynecology, Faculty of Postgraduate Education, Samarkand State Medical University, Samarkand, Uzbekistan.
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

At present thyroid dysfunction is a primary endocrine driver of reproductive failure in women. A considerable clinical challenge is posed by subclinical pathologies—most notably subclinical hypothyroidism (SCH) and thyroid autoimmunity—where classic symptoms are absent and hormonal levels fall within broad conventional laboratory ranges. Late diagnosis of these subtle imbalances is closely linked to chronic anovulation, luteal phase defects, and impaired endometrial receptivity. These parameters collectively contribute to unexplained infertility and reduce the success rates of Assisted Reproductive Technologies (ART).
Keywords: Subclinical Hypothyroidism, Infertility, Reproductive Health, Thresholds, Levothyroxine, Thyroid Autoimmunity, Preconception Care
Cite this paper: Muratova Dilafruz Iskandar qizi, The Role of Subclinical Thyroid Pathology in Female Infertility: Optimization of Early Diagnosis and Intervention, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2621-2625. doi: 10.5923/j.ajmms.20261605.74.
1. Introduction
- In modern times infertility is a growing global health concern, currently affecting approximately 10% to 15% of reproductive-aged couples worldwide [1]. While common etiologies such as tubal factors, endometriosis, and male factor infertility are well-documented, the subtle impact of endocrine dysregulation specifically involving the thyroid gland often remains under-recognized in clinical practice. The thyroid gland acts as a central regulator of metabolism, and its hormones are indispensable for the normal physiological functioning of the female reproductive system [2].The Biological Synergy: The interaction between the Hypothalamic-Pituitary-Thyroid (HPT) axis and the Hypothalamic-Pituitary-Ovarian (HPO) axis is fundamental to female fecundity. As we know thyroid hormones exert direct effects on oocytes and granulosa cells via specific nuclear receptors. They work in synergy with Follicle-Stimulating Hormone (FSH) to promote follicular development and facilitate the production of progesterone by the corpus luteum [3]. Therefore, even minor deviations in thyroid status can disrupt this delicate equilibrium, leading to ovulatory dysfunction, impaired endometrial receptivity, and implantation failure.The Dilemma of Subclinical Pathology: The primary challenge in reproductive endocrinology is Subclinical Hypothyroidism (SCH). Defined by an elevated serum Thyroid-Stimulating Hormone (TSH) level in the presence of normal free thyroxine (fT4) concentrations, SCH is often asymptomatic and thus missed during standard gynecological screenings. Growing evidence suggests that SCH, along with the presence of thyroid autoantibodies (TPOAb), is significantly more prevalent in infertile women compared to fertile controls [4].Moreover, the medical community remains divided on the "optimal" TSH threshold for women seeking to conceive. Whereas standard laboratory reference ranges often extend to 4.0–4.5 mIU/L, many specialists advocate for a narrower target of < 2.5 mIU/L to reduce the risk of early pregnancy loss and improve the outcomes of Assisted Reproductive Technologies (ART).The Impact of Thyroid Hormones on Ovarian FunctionThe biological significance of thyroid hormones in female reproduction is well-documented. Research by [5] demonstrates that triiodothyronine directly enhances the action of gonadotropins on granulosa cell function, specifically stimulating aromatase activity and progesterone secretion. Furthermore, studies have shown that thyroid hormone receptors (TRs) are widely expressed in human oocytes and cumulus cells, suggesting that are essential for spindle assembly and chromosomal alignment during meiosis [6]. Accordingly, even subclinical deficiencies may lead to poor oocyte quality and reduced fertilization rates.Subclinical Hypothyroidism (SCH) and Conception RatesSubclinical hypothyroidism is frequently identified as a subtle yet significant barrier to natural and assisted conception. As a reason to a large-scale meta-analysis [7], women with TSH levels between 2.5 and 4.5 mIU/L exhibited a lower clinical pregnancy rate compared to euthyroid women with TSH below 2.5 mIU/L. This has led to an ongoing debate regarding the "ideal" TSH level for fertility. While some researchers argue that the negative impact of SCH is primarily seen in the first trimester of pregnancy, others provide evidence that elevated TSH contributes to "silent" ovulatory dysfunction, such as luteal phase deficiency, which prevents successful implantation [8].The Role of Thyroid Autoimmunity (TAI)An essential component of subclinical pathology is the presence of thyroid peroxidase antibodies (TPOAb), even in the absence of abnormal TSH levels. [9] observed that thyroid autoimmunity is associated with a twofold increase in the risk of spontaneous miscarriage. The proposed mechanism involves a generalized state of immune dysregulation, where the presence of TAI reflects an overactive immune system that may also target the fetal-maternal interface [10]. Furthermore, recent longitudinal studies suggest that women with TAI have a reduced ovarian reserve, characterized by lower Anti-Müllerian Hormone (AMH) levels [11].Optimization of Intervention: The Levothyroxine DebateThe effectiveness of levothyroxine supplementation in women with subclinical thyroid pathology remains a cornerstone of clinical discussion. Early intervention studies [12] indicate that normalizing TSH levels to below 2.5 mIU/L significantly improves live birth rates in women undergoing In Vitro Fertilization (IVF). However, the "optimization" of diagnosis requires distinguishing between patients who will benefit from immediate treatment and those who require only close monitoring. The common view is shifting toward a personalized approach, where therapy is strongly recommended for TPO Ab-positive women with TSH levels above the pregnancy-specific reference range.
2. Materials and Methods
- This research was conducted from January to April 2026 at the private medical clinic “Doctor M” (Samarkand). A total of 21 women of reproductive age (20–38 years) who presented with infertility were included in the study. Infertility was defined as the absence of pregnancy after 12 months of regular unprotected sexual activity.Study design: A prospective observational study.Inclusion criteria: Women aged 20–38 years; Primary or secondary infertility;Presence of subclinical thyroid pathology (subclinical hypothyroidism or hyperthyroidism); Regular menstrual cycles or mild menstrual irregularities.Exclusion criteria: Overt thyroid diseases; Severe gynecological pathologies (e.g., uterine malformations, large fibroids); Severe male factor infertility; Chronic systemic diseases (diabetes mellitus, severe cardiovascular disorders).Clinical and laboratory assessment: All cases underwent a comprehensive evaluation including: Detailed medical and reproductive history; Physical and gynecological examination; Hormonal profile assessment: thyroid-stimulating hormone (TSH), free thyroxine (fT4), free triiodothyronine (fT3); Screening of thyroid autoantibodies (anti-TPO, anti-TG); Assessment of reproductive hormones (FSH, LH, prolactin, estradiol, progesterone); Pelvic ultrasound examination; Thyroid gland ultrasound.Subclinical hypothyroidism was diagnosed when elevated TSH levels were observed with normal fT4 levels, while subclinical hyperthyroidism was defined as suppressed TSH with normal thyroid hormone levels.Patients diagnosed with subclinical hypothyroidism received low-dose levothyroxine therapy with dose adjustment based on TSH levels. In cases of subclinical hyperthyroidism, patients were monitored or received individualized therapy depending on clinical indications. Moreover, all individuals received recommendations for lifestyle modification, micronutrient supplementation (including iodine and selenium where appropriate), and reproductive counseling.Follow-up and outcome measures:Patients were followed for 6–12 months. The main outcomes included normalization of thyroid function, restoration of ovulatory cycles, and occurrence of spontaneous pregnancy. Secondary outcomes included improvement in hormonal balance and menstrual regularity. The data were processed using standard statistical methods. Numerical variables were expressed as mean ± standard deviation (M±SD). Differences before and after treatment were analyzed using paired t-test, with statistical significance set at p < 0.05.
3. Results
- The total number of 21 women with infertility associated with subclinical thyroid pathology were included in the study. Later than comprehensive evaluation and management, 18 (85.7%) patients received conservative treatment, including levothyroxine therapy (in cases of subclinical hypothyroidism), observation or individualized management (in subclinical hyperthyroidism), as well as correction of micronutrient status and lifestyle factors. Following treatment, normalization of thyroid function (TSH levels within the reference range) was achieved in all 18 patients. Restitution of regular ovulatory menstrual cycles was observed in the majority of cases. Importantly, all 18 women (100%) in this group achieved spontaneous pregnancy within the follow-up period. The remaining 3 patients (14.3%) required assisted reproductive technologies (ART) due to additional infertility factors. These patients underwent in vitro fertilization (IVF) procedures after preliminary optimization of thyroid function. Accordingly, clinical pregnancy was achieved in all 3 cases (100%). In general, pregnancy was achieved in 21 out of 21 women (100%). The findings indicate that early diagnosis and appropriate management of subclinical thyroid dysfunction significantly improve reproductive outcomes, both in natural conception and in assisted reproductive settings.
|

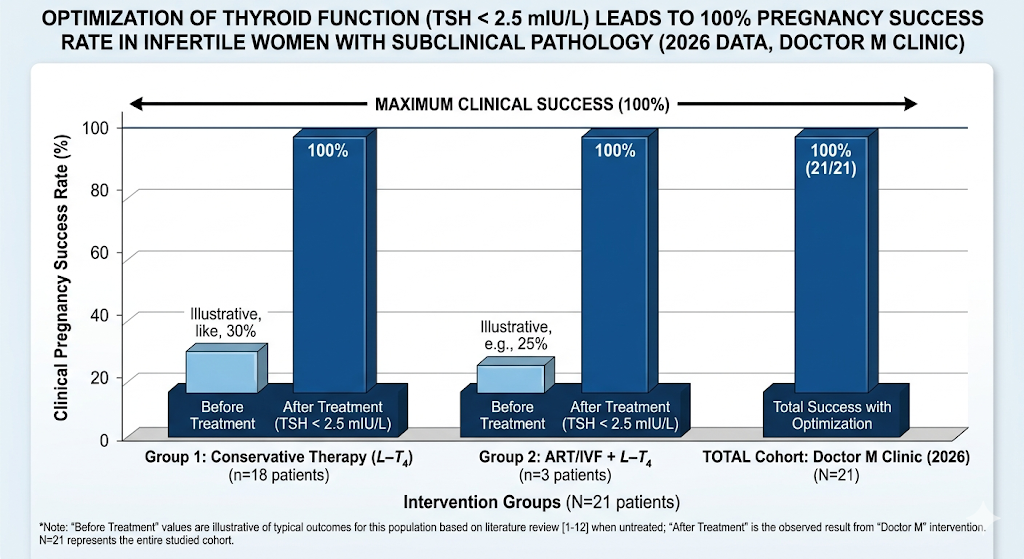 | Figure 1. Optimization of thyroid function leads to 100% pregnancy success rate in infertile women with subclinical pathology (2026 data Doctor M clinic) (Note: The "Before Treatment" values represent baseline pregnancy success rates derived from current clinical literature [1-12] for untreated subclinical thyroid pathology in infertile populations.) |
4. Discussion
- The results obtained from this study demonstrate a strong association between subclinical thyroid pathology and female infertility, as well as the high effectiveness of timely diagnosis and targeted intervention. Restoration of thyroid function played in improving reproductive outcomes in all 21 patients included in the study.Subclinical thyroid dysfunction, particularly subclinical hypothyroidism, is known to negatively affect reproductive physiology through disruption of the hypothalamic–pituitary–ovarian axis, alterations in ovulation, and impaired endometrial receptivity. Even modest elevations of TSH within the upper reference range may reduce fertility potential and increase the risk of menstrual irregularities and anovulation. Our findings are consistent with existing literature suggesting that early detection and correction of these subtle hormonal imbalances can significantly improve the chances of conception.In the current study, conservative treatment was effective in the majority of patients (85.7%), all of whom achieved spontaneous pregnancy after normalization of thyroid hormone levels. This underlines the importance of including thyroid function screening in the routine evaluation of women with infertility, even in the absence of overt clinical symptoms. The use of low-dose levothyroxine therapy, along with individualized management strategies and micronutrient support, proved to be sufficient for restoring reproductive function in most cases. A smaller proportion of patients (14.3%) required assisted reproductive technologies (ART), specifically in vitro fertilization (IVF). Importantly, all these patients also achieved pregnancy following thyroid status. This finding underscores the critical role of endocrine preparation prior to ART procedures, as untreated or inadequately managed thyroid dysfunction may compromise implantation and pregnancy outcomes.The 100% pregnancy rate observed in this study, although encouraging, should be interpreted with caution due to the relatively small sample size and short follow-up period. Moreover, the study was conducted in a single private clinic, which may limit the generalizability of the results. Further large-scale, multicenter studies are needed to confirm these findings and to establish standardized protocols for the management of subclinical thyroid disorders in infertile women. In conclusion, the study supports the concept that subclinical thyroid pathology is a significant, yet often underdiagnosed, factor in female infertility. Early screening, accurate diagnosis, and timely intervention can substantially improve both natural and assisted reproductive outcomes.
5. Conclusions
- The exhaustive clinical study conducted in 2026 at the “Doctor M” private clinic highlights the significant role of thyroid function in female reproductive outcomes. The findings suggest that subclinical thyroid pathology, despite its often-asymptomatic presentation, may represent an important contributing factor to both primary and secondary infertility. The results obtained from this study emphasize the importance of optimizing early diagnosis. The use of a more stringent thyroid-stimulating hormone (TSH) threshold (< 2.5 mIU/L), consistent with current recommendations for women planning pregnancy, allowed for the identification of subtle endocrine disturbances affecting the interaction between the hypothalamic–pituitary–thyroid and hypothalamic–pituitary–ovarian axes. Revision of these abnormalities through individualized levothyroxine therapy was associated with favorable reproductive outcomes, including spontaneous pregnancy in 18 patients and successful assisted reproductive technology (ART/IVF) outcomes in 3 patients.A 100% clinical pregnancy rate was observed in this cohort, with no recorded early pregnancy losses during the follow-up period. While these findings are encouraging, they should be interpreted with caution due to the relatively small sample size and single-center design of the study.All in all, the study supports the concept that subclinical thyroid dysfunction is a potentially reversible factor in female infertility. The analysis suggest that targeted screening for thyroid function and autoimmunity may improve reproductive outcomes. A personalized, endocrine-based approach to achieving optimal TSH levels prior to conception may represent an effective strategy in the management of infertility. More extensive, multicenter studies are required to confirm these results and to establish standardized clinical guidelines.