-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(5): 2593-2596
doi:10.5923/j.ajmms.20261605.68
Received: Apr. 16, 2026; Accepted: May 22, 2026; Published: May 25, 2026

Experience of Using a Protephage in the Treatment of Liver Abscess by the Method of Minimally Invasive Drainage
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMatmurotov K. Zh., Pulatov U. I., Kasimov U. K., Ikramov A. Ya.
Tashkent State Medical University, Tashkent, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Liver abscess is a critical emergency condition in abdominal surgery, significantly worsening the course of the underlying disease and the patients' condition. Objective: To analyze the clinical, laboratory, instrumental, and microbiological data of patients diagnosed with liver abscesses, and to evaluate the efficacy of minimally invasive abscess cavity drainage combined with debridement of the purulent cavity using Proteofag-polivalent. Materials and Methods: A scientific study was conducted involving 19 patients (aged 29–63 years; 57.9% women, 42.1% men) with liver abscesses, treated in the Department of Purulent Surgery and Surgical Complications of Diabetes at the Multidisciplinary Clinic of Tashkent State Medical University in 2025–2026. All patients underwent minimally invasive drainage of liver abscesses with debridement of the cavity using polyvalent proteases and antiseptics. Results: All patients were comprehensively evaluated. A minimally invasive drainage of liver abscesses under ultrasound guidance was performed. Against the background of , comprehensive therapy—including antibacterial and anti-inflammatory treatment and daily abscess cavity debridement—showed positive dynamics. All patients were discharged to an outpatient follow-up phase in stable, satisfactory condition with drains removed after 5–7 days, under the supervision of polyclinic physicians. Conclusion: Minimally invasive drainage with active irrigation using protephagic and antiseptic solutions is an effective method for rapid abscess cavity cleansing and allowed avoidance of traumatic surgical intervention.
Keywords: Protephage
Cite this paper: Matmurotov K. Zh., Pulatov U. I., Kasimov U. K., Ikramov A. Ya., Experience of Using a Protephage in the Treatment of Liver Abscess by the Method of Minimally Invasive Drainage, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2593-2596. doi: 10.5923/j.ajmms.20261605.68.
1. Introduction
- According to pooled data, the incidence of liver abscesses ranges from 8 to 15 cases per 100,000 inhabitants per year, and mortality fluctuates between 5 and 26%. The formation of purulent foci in the liver is accompanied by severe complications such as liver failure and cholangiogenic sepsis [4,8,9]. According to some authors, multiple large bilobar liver abscesses with intraluminous sequestra are an indication for open, including resective, surgical interventions [9,12,14]. On the other hand, in recent years there has been an increase in publications attesting to the advantages of minimally invasive percutaneous puncture-drainage techniques under ultrasound or CT control, which are the primary method of treatment [9,15]. The advantages of this method include minimal invasiveness, relative safety, better tolerance in debilitated patients, and the absence of the need for anesthesia. The use of minimally invasive technologies reduces the risk of peritoneal infection, postoperative wound abscesses, the development of postoperative hernias, and adhesions [2,7,13]. For intra-organ abscesses in the liver, "Pigtail" ("pig's tail") drains are used. The "Pigtail" device is a sterile, thin, long catheter that, upon final placement, forms the shape of a pig's tail, hence the device's name [3,5,10,11]. When draining the abscess cavity, it is irrigated daily with antiseptic and antibiotic solutions, followed by daily ultrasound monitoring to assess the degree of reduction. Normalization of body temperature and clinical blood tests, absence of discharge through the drain, and reduction of the abscess cavity are criteria for drain removal [1,4,10]. The average duration of drainage is (15.1±5.4) days [3,6,11].The aim of our study was to analyze the clinical, laboratory, instrumental, and microbiological data of patients diagnosed with liver abscesses, and to evaluate the efficacy of minimally invasive abscess cavity drainage combined with debridement of the purulent cavity with "Proteophage-Polivalent."
2. Materials and Methods
- The basis of this work is the examination and treatment results of 19 patients with liver abscesses who were hospitalized in the Department of Purulent Surgery and Surgical Complications of Diabetes at the Multidisciplinary Clinic of Tashkent State Medical University in 2025–2026. All patients underwent minimally invasive drainage of the liver abscess cavity, followed by irrigation with antiseptics and exposure to "Proteophage-polivalent."
 | Figure 1. Distribution of patients by gender in the main and control groups: men — 4 patients in each group; women — 5 patients in the main group and 6 patients in the control group |
3. Results
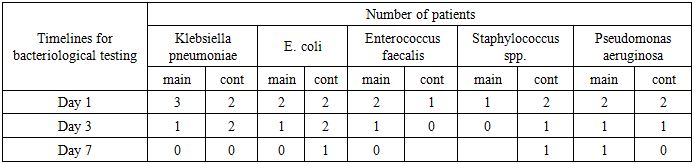
- The analysis of the bacteriological examination results of the exudate showed that on day 1, all observations revealed pronounced microbial contamination dominated by conditionally pathogenic flora. By day 3, a significant decrease in the number of detectable microorganisms was noted, especially in the main group. The most pronounced positive dynamic was observed for Klebsiella pneumoniae, Escherichia coli, and Enterococcus faecalis. By the 7th day, the growth of the aforementioned microorganisms was virtually absent. However, Staphylococcus spp. and Pseudomonas aeruginosa persisted in isolated cases, which may indicate their relative resistance to the therapy administered.
|
4. Conclusions
- Minimally invasive drainage of a liver abscess and decontamination of its cavity using "Proteophage-Polivalent" is an effective and alternative treatment method for liver abscesses, which can be applied regardless of the abscess's size and location. Active use and debridement of the hepatic cavity with "Proteophaga-polivalent" solutions allows for increased effectiveness of minimally invasive drainage of a liver abscess and accelerates the recovery of liver dysfunction parameters, promoting faster debridement of the purulent cavity and reducing the duration of systemic antibiotic therapy, as well as shortening patients' hospital stays.