-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(5): 2588-2592
doi:10.5923/j.ajmms.20261605.67
Received: Apr. 28, 2026; Accepted: May 23, 2026; Published: May 25, 2026

Effectiveness of a Complex of Minimally Invasive Surgical Interventions in Patients with Liver Abscesses
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMatmurotov K. Zh.1, Pulatov U. I.1, Bobokulova Sh. A.1, Yakhshiboev S. Sh.2
1Tashkent State Medical University, Tashkent, Uzbekistan
2Urgench State Medical Institute, Urgench, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Objective: To evaluate the effectiveness of a complex of minimally invasive surgical interventions in the treatment of liver abscesses. Materials and Methods. This study included 83 patients with liver abscesses who underwent inpatient treatment in the Department of Purulent Surgery at the Multidisciplinary Clinic of Tashkent State Medical University. Depending on the surgical approach used, patients were divided into two groups. The first (control) group consisted of 46 patients (55.4%) treated between 2017 and 2020. The second (main) group included 37 patients (44.6%) treated between 2021 and 2024. In patients of the main group, minimally invasive procedures were performed using individually selected techniques, taking into account the location of the pathological focus in the liver. Additionally, superselective intra-arterial catheter therapy was applied. Based on an analysis of the results of using combined minimally invasive technologies in patients with liver abscesses, the surgical approach was improved. Increased treatment efficacy was achieved through the optimization of the intra-arterial catheter therapy technique, as well as the rational selection of the negative pressure level during drainage of the abscess cavity.
Keywords: Liver abscess, Abscess drainage, Arterial catheterization, Minimally invasive treatment
Cite this paper: Matmurotov K. Zh., Pulatov U. I., Bobokulova Sh. A., Yakhshiboev S. Sh., Effectiveness of a Complex of Minimally Invasive Surgical Interventions in Patients with Liver Abscesses, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2588-2592. doi: 10.5923/j.ajmms.20261605.67.
1. Introduction
- The diagnosis and treatment of liver abscesses remain one of the most complex and significant challenges in abdominal surgery [1,2,4,9,14]. Despite advances in modern technology, this condition continues to be associated with a high risk of complications and adverse outcomes.In recent years, there has been an increase in the number of severe destructive diseases of the abdominal organs, particularly acute pancreatitis, which is currently considered one of the leading causes of pylephlebitis with subsequent formation of liver abscesses. Traumatic injuries to the abdominal organs also play a significant role [3,5,10].At the same time, there has been an increase in the number of surgical interventions on the bile ducts, including minimally invasive and open surgeries involving the placement of stents and transhepatic drains. This, in turn, contributes to an increase in the incidence of cholangio-genic liver abscesses. Despite accumulated clinical experience, treatment outcomes for this patient population remain unsatisfactory. The complication rate reaches 55%, and the mortality rate ranges from 12 to 38% for solitary abscesses and can reach 77–90% for multiple liver lesions [1,5,6,11,14].In recent decades, minimally invasive methods for treating liver abscesses have proven to be highly effective. Their main advantages include minimal invasiveness, the ability to perform the procedure under local anesthesia, and the possibility of performing them in various hospital departments, including intensive care units. In addition, these technologies are cost-effective [2,6,7,13]. According to several studies, hepatic artery catheterization, as well as puncture and drainage of abscesses under imaging guidance, are technically feasible and highly effective treatment methods. Their implementation has made it possible to significantly reduce the number of open surgical procedures, lower the incidence of postoperative complications, and shorten the length of patient hospital stays [8,12,13].
2. Materials and Methods
- This study analyzed the outcomes of surgical treatment in 83 patients with liver abscesses. The clinical data were collected at the Department of Infectious Surgery of the Tashkent State Medical University’s Multidisciplinary Clinic between 2017 and 2024.Depending on the surgical approach used, all patients were divided into two groups. The first group (the comparison group) included 46 patients (55.4%) who underwent treatment between 2017 and 2020. In patients in this group, surgical interventions were performed according to a traditional protocol, which included catheterization of the celiac trunk followed by intra-arterial catheter therapy without regard to the location and nature of the pathological focus, as well as drainage of the liver abscess cavity.The second (main) group included 37 patients (44.6%) who were treated between 2021 and 2024. In this group, the surgical approach was determined on an individual basis, taking into account the location, size, and severity of the inflammatory process. Long-term intra-arterial catheter therapy (LITACT) was performed selectively, depending on the affected segment of the liver. After drainage of the abscess cavity, a negative pressure system was connected on the 3rd–4th day. Regardless of the surgical technique chosen, all patients received comprehensive conservative therapy, which included antibacterial, antifungal, infusion, and intensive medical interventions. When selecting a treatment strategy in the comparison group, the severity of the patient’s condition, the nature of the pathological process, and the sensitivity of the microflora to antibacterial drugs were taken into account.Analysis of the localization of the pathological process showed that liver abscesses were most frequently detected in cases of combined involvement of segments VII–VIII (18.0%). A comparison of the groups yielded comparable figures: 17.4% in the comparison group and 19.0% in the main group. In most cases, combined segmental involvement was noted, with segments V–VI and IV–V, VIII being the most frequently affected (14.4% each). The lowest frequency was observed for abscesses localized in segments I and IV—1.2% of the total number of cases. Based on the size of the pathological lesion, it was found that in 39 patients (47.0%) the abscess diameter exceeded 8.0 cm, indicating delayed presentation for medical care and resulting in technical difficulties in selecting a surgical treatment method. In 32 patients (38.6%), the size of the abscesses ranged from 5.0 to 8.0 cm. An increase in the size of the lesion was accompanied by a pronounced inflammatory reaction in the perifocal tissues, which required a differentiated approach to the selection of treatment strategies and the prevention of postoperative complications. The smallest group consisted of patients with abscesses up to 2.0 cm in diameter (4 cases), who underwent predominantly conservative treatment with puncture of the lesion. In the main group, treatment for such patients was limited to intra-arterial catheter therapy, taking into account the segmental localization of the inflammatory process. Combined minimally invasive treatment methods were used in all patients. In the comparison group, liver abscess drainage was performed under ultrasound guidance in combination with celiac trunk catheterization for intra-arterial pharmacotherapy (see Fig. 1).
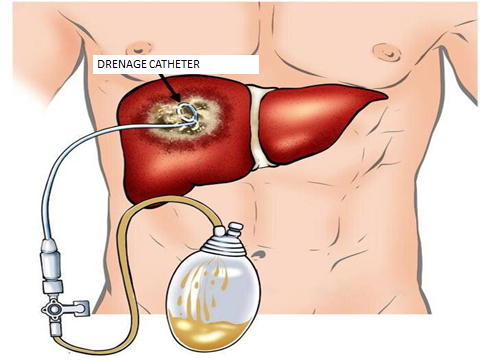 | Figure 1. Minimally invasive drainage of a liver abscess |
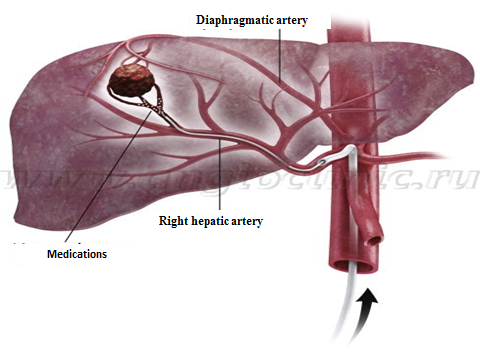 | Figure 2. Superselective catheterization of the hepatic artery |
3. Results
- To objectively assess the effectiveness of the treatment, all patients underwent multislice computed tomography of the abdominal organs with contrast enhancement of the drainage system. A comparative analysis showed that the use of a differentiated combined approach increased the rate of favorable outcomes in the main group by 10.4%, indicating a higher probability of recovery following the initial intervention. In addition, a decrease in the proportion of patients requiring repeat surgeries (from 17.4% to 10.8%) was noted, as well as a reduction in the mortality rate (from 6.5% to 2.7%) (see Fig. 3).
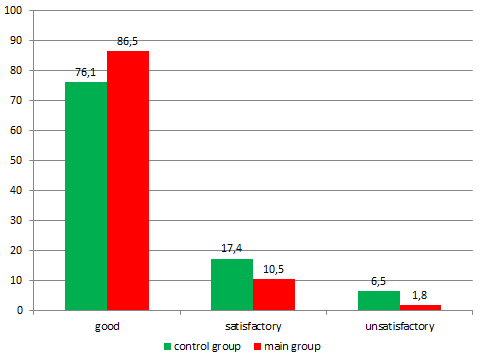 | Figure 3. Comparison of short-term outcomes |
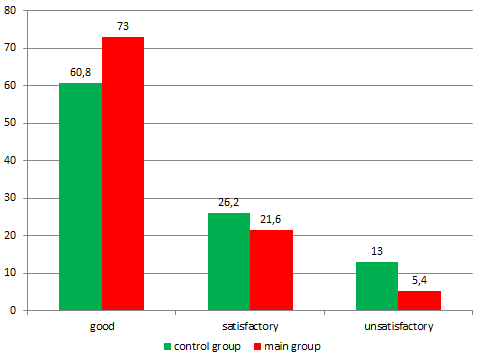 | Figure 4. Comparison of long-term outcomes |
4. Discussion
- Overall, this study convincingly demonstrates the effectiveness of a combination of minimally invasive treatment methods for liver abscesses. Further refinement of this technique to reduce the incidence of adverse treatment outcomes and a thorough analysis of the results in the context of evidence-based medicine will lead to the widespread adoption of this surgical approach in all medical and preventive care facilities. The global trend in the development of modern surgery, including in purulent surgery, is also considered a promising direction and requires further research to determine the optimal indications for this surgical method. It should be noted that the surgical treatment of purulent-inflammatory liver diseases presents significant clinical complexity and requires the individualization of therapeutic strategies. Liver abscess remains a severe nosological form characterized by a high risk of complications and fatalities, especially in patients with comorbidities. Thus, summarizing the data obtained, it can be concluded that the use of a differentiated combined minimally invasive approach in the puncture-drainage treatment of liver abscesses statistically significantly reduces the frequency of repeat surgical interventions and the mortality rate among patients. In addition, an acceleration in the recovery of liver function, faster resolution of the residual cavity and eradication of the pathological infectious focus, as well as a reduction in the duration of antibiotic therapy and the length of hospital stay, were also noted.
5. Conclusions
- 1. Traditional approaches to minimally invasive surgical treatment of liver abscesses result in primary recovery in only 76.1% of patients. At the same time, the rate of repeat surgical interventions is 17.4%, and the mortality rate can reach 6.5%. 2. An improved, differentiated approach to minimally invasive interventions, including superselective catheterization of the hepatic arteries (taking into account the location of the pathological focus: right side—segments V–VIII, left side—segments I–IV) combined with the use of VAC therapy (in the appropriate mode) demonstrates high clinical efficacy. This surgical approach helps reduce the incidence of postoperative complications, lower the risk of disease recurrence, and improve long-term treatment outcomes in patients with liver abscess. 3. Further detailed study and identification of all surgical aspects regarding the absolute or relative indications for this surgical strategy require large randomized clinical trials that will demonstrate the necessity of selecting a specific approach with statistically significant evidence-based data.