-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(5): 2580-2583
doi:10.5923/j.ajmms.20261605.65
Received: Mar. 28, 2026; Accepted: Apr. 20, 2026; Published: May 25, 2026

Assessment of Affective Disorders in Rheumatoid Arthritis
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLUrolova Dilafruz Abdurazzoq qizi
Assistant at the Department of Psychiatry and Narcology, Tashkent State Medical University, Tashkent, Uzbekistan
Correspondence to: Urolova Dilafruz Abdurazzoq qizi, Assistant at the Department of Psychiatry and Narcology, Tashkent State Medical University, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Rheumatoid arthritis (RA) is a chronic autoimmune inflammatory disease of connective tissue, primarily affecting small joints. The long-term course of the disease leads to severe physical disability, reduced quality of life, and impaired social adaptation. In recent years, it has been established that RA causes not only somatic, but also serious mental health problems. Studies indicate that anxiety-depressive disorders (ADD) occur in 30–80% of RA patients, which is 4–7 times higher compared to the general population. Background: To assess the prevalence and clinical characteristics of anxiety-depressive disorders in patients with rheumatoid arthritis, as well as their impact on the course of RA. Additionally, to evaluate the correlation between the severity of ADD and clinical indicators of RA. Methods: The study included 217 patients with a confirmed diagnosis of RA who underwent treatment in the rheumatology department in Tashkent. The patients’ age ranged from 25 to 65 years, with a mean age of 48.3 ± 8.7 years. Among them, 79% were women and 21% were men. Patients were divided into two groups: Group I (n=108) with signs of anxiety-depressive disorders; Group II (n=109) without significant ADD. Socio-anamnestic questionnaire, SF-36 Health Survey, HADS (Hospital Anxiety and Depression Scale), PHQ-9 (Patient Health Questionnaire-9), statistical methods: descriptive statistics, Student’s t-test, correlation analysis. Results: According to the socio-anamnestic survey, anxiety-depressive disorders were more common in women (78%), in unmarried individuals (64%), and in patients without permanent employment (59%). HADS results: 65% of patients showed varying degrees of anxiety and depression. Severe anxiety was observed in 42%, severe depression in 33%, and a combination of anxiety and depression in 25%. PHQ-9 results: 38% of patients demonstrated signs of moderate to severe depression. SF-36 results: patients with ADD had significantly lower quality of life; physical functioning, psychological well-being, and social functioning were markedly reduced (p<0.01). Conclusions: The findings show that anxiety-depressive disorders aggravate the course of rheumatoid arthritis: pain sensitivity increases, treatment adherence decreases, and social and psychological adaptation worsens. The higher prevalence of ADD among women, unmarried, and unemployed patients highlights the significant role of socio-psychological factors. Therefore, treatment of RA patients should involve not only rheumatologists, but also psychiatrists and psychotherapists.
Keywords: Rheumatoid arthritis, Joints, Depression, Anxiety-depressive disorder, Antidepressants
Cite this paper: Urolova Dilafruz Abdurazzoq qizi, Assessment of Affective Disorders in Rheumatoid Arthritis, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2580-2583. doi: 10.5923/j.ajmms.20261605.65.
1. Introduction
- Rheumatoid arthritis (RA) is a chronic autoimmune inflammatory disease of connective tissue that primarily affects small joints. The long-term course of the disease can lead to severe physical disability, reduced quality of life, and impaired social functioning. In recent years, it has become clear that RA causes not only somatic but also significant psychological problems [1,2,3]. Studies show that 30–80% of patients with RA experience anxiety and depressive disorders, which is 4–7 times higher than in the general population. International data indicate that 50–70% of RA patients have mental health disturbances, particularly anxiety and depression. The chronic nature of the disease, persistent pain syndrome, decreased quality of life, and limitations in social activity often contribute to the development of anxiety-depressive spectrum disorders [4,5,6]. In particular, affective and psychological disturbances associated with autoimmune diseases such as RA and systemic lupus erythematosus (SLE) are of special importance.Despite the fact that RA is widely diagnosed in clinical practice and anxiety-depressive disorders (ADD) are highly prevalent among these patients, such conditions are often not identified in a timely manner, and appropriate treatment is not prescribed. This is mainly because clinicians tend to focus primarily on the somatic manifestations of the disease [7,8,9,10].Depression, in many cases, should not be regarded as an independent disorder but rather as part of the patient’s overall, integrated clinical condition. Underestimation of depression may lead to worsening of both the patient’s general state and the course of the underlying disease [11,12,13,14,15].According to a study by Ayşe Unal, Hakan Nur, and colleagues, only 14% of patients with RA and anxiety-depressive disorders are willing to openly discuss their mental health with a rheumatologist. The remaining patients either do not recognize their depressive symptoms, attribute all problems to RA and expect improvement with reduced disease activity, or simply ignore these symptoms. As a result, fewer than 19% of patients with RA and ADD receive adequate psychopharmacological or psychotherapeutic care.According to G.J. Treharne et al., 9% of patients with RA have experienced suicidal thoughts at least once in their lifetime. If depression is also present, this figure rises to 30%. Among patients with systemic lupus erythematosus, suicidal ideation or attempts are observed in 12% of cases.Interestingly, despite poor adherence to medical recommendations, patients with RA and anxiety-depressive disorders tend to seek medical care more frequently and are hospitalized more often compared to patients with other diagnoses. At the same time, depression has a significantly negative impact on daily functioning, self-care, and physical activity at home and in the workplace among patients with RA. The aim of this study was to investigate the prevalence and clinical characteristics of anxiety-depressive disorders in patients with rheumatoid arthritis (RA) and to determine their impact on the course of RA. Additionally, the study aimed to assess the relationship between the severity of anxiety-depressive disorders and clinical indicators of RA.
2. Materials and Methods
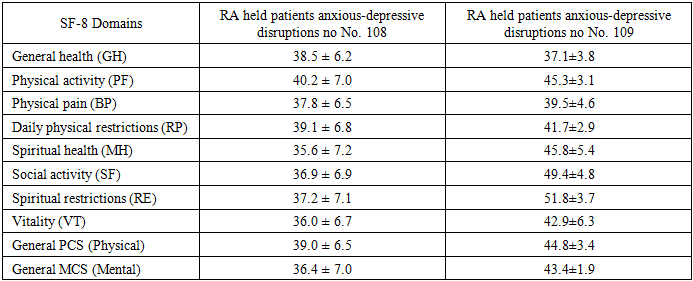
- The study included 217 patients with a confirmed diagnosis of rheumatoid arthritis who were treated in the rheumatology department in Tashkent. The patients’ age ranged from 25 to 65 years, with a mean age of 48.3 ± 8.7 years. Among them, 79% were female and 21% were male. The patients were divided into two groups: Group I (n = 108): patients with signs of anxiety-depressive disorders; Group II (n = 109): patients without clinically significant anxiety-depressive symptoms: Socio-anamnestic questionnaire, SF-36 Health Survey, Hospital Anxiety and Depression Scale (HADS), Patient Health Questionnaire-9 (PHQ-9), Statistical methods: descriptive statistics, Student’s t-test, and correlation analysis. All patients with rheumatoid arthritis were assessed for levels of anxiety and depression using the Hospital Anxiety and Depression Scale (HADS). In addition, overall health status was evaluated using the SF-8 scale, and both trait and state anxiety levels were determined using the Spielberger–Khanin Anxiety Inventory. The statistical significance of differences between groups was assessed using contingency table analysis based on Fisher’s exact test and Pearson’s χ² test. Quantitative variables with normal distribution were compared using Student’s t-test, while non-normally distributed variables were analyzed using the Mann–Whitney nonparametric test. During clinical examination, biochemical analyses were performed using blood samples. Taking all of the above into account, mental status, subjective and objective anamnestic data, medical records (including case histories, archival data, and outpatient charts), as well as conclusions from specialists in hematology and neurology, were analyzed. Somatic status assessment was based on clinical examination results obtained by the staff of clinical departments.
3. Result and Discussion
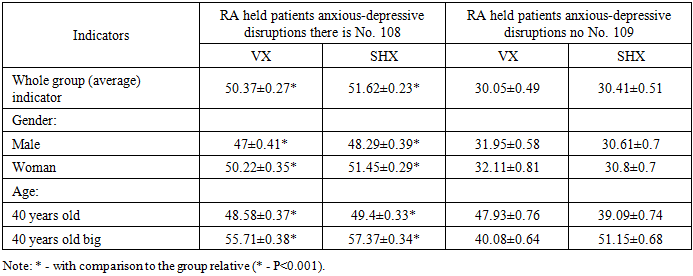
- According to the socio-anamnestic survey, anxiety-depressive disorders were more frequently observed among women (78%), unmarried individuals (64%), and patients without permanent employment (59%). In our study, participants were divided into two groups based on the Hospital Anxiety and Depression Scale (HADS): patients with Rheumatoid arthritis with anxiety-depressive disorders and patients with rheumatoid arthritis without anxiety-depressive disorders. The psycho-emotional status of both groups was further assessed using the Spielberger–Khanin Anxiety Inventory (Table 1).
|
|
4. Conclusions
- Affective disorders are widespread among patients with rheumatoid arthritis and are often underdiagnosed. Anxiety-depressive disorders aggravate the course of RA, increase pain intensity, and reduce treatment adherence. Early diagnosis and treatment of these disorders (including the use of antidepressants) improve both mental and somatic conditions of patients. A multidisciplinary approach (rheumatologist + psychiatrist) increases treatment effectiveness and improves patients’ quality of life.The use of diagnostic and treatment algorithms for affective disorders in patients with rheumatoid arthritis allows for early detection of anxiety-depressive conditions, optimal selection of treatment strategies, and improved therapeutic outcomes. This contributes to reducing chronic anxiety-depressive conditions, improving patients’ social adaptation, and decreasing the burden on primary healthcare services.Implementation of this algorithm in clinical practice will help improve patients’ quality of life and reduce the overall burden of mental disorders among the population of patients with rheumatoid arthritis.