-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(5): 2571-2574
doi:10.5923/j.ajmms.20261605.63
Received: Apr. 20, 2026; Accepted: May 15, 2026; Published: May 25, 2026

Comparative Assessment of the Adapted Therapeutic and Preventive Program of Dental Diseases in Children
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMatkulieva Sevara1, Khabibа Isakhodzhaevа1, Dilmurod Аbdullaev2
1PhD., Associate Professor, Tashkent State Medical University, Tashkent, Uzbekistan
2Doctor of Medical Sciences, Associate Professor, Tashkent State Medical University, Tashkent, Uzbekistan
Correspondence to: Khabibа Isakhodzhaevа, PhD., Associate Professor, Tashkent State Medical University, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

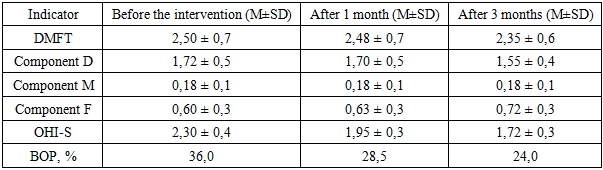
The analysis showed that regular preventive visits to the dentist are a key element in maintaining the dental health of children with visual impairment. Regular monitoring makes it possible to identify pathological changes at an early stage, adjust individual hygiene skills and reduce the risk of disease progression, which is especially important in conditions of limited self-control in this group of patients. Repeated examinations of children with visual impairment, conducted one and three months after the start of the adapted treatment and prevention program, were aimed at assessing its effectiveness in the short term. The purpose of these surveys was to determine the dynamics of the main clinical indicators of dental health, including the caries prevalence index (DMFT), the oral hygiene index (OHI-S) and the frequency of bleeding gums (BOP).
Keywords: Prevention, Dental index, Visual impairment
Cite this paper: Matkulieva Sevara, Khabibа Isakhodzhaevа, Dilmurod Аbdullaev, Comparative Assessment of the Adapted Therapeutic and Preventive Program of Dental Diseases in Children, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2571-2574. doi: 10.5923/j.ajmms.20261605.63.
1. Introduction
- Dental caries in young children remains one of the most serious global dental health problems. Recent epidemiological data from Shanghai (China) showed that among 1,281 five-year-olds, the prevalence of caries was 51.0%, with an average dmft index of 2.46. These data confirm the continuing high prevalence of caries in preschoolers and emphasize the need for comprehensive prevention programs aimed at modifiable behavioral risk factors [1,4,10]. These three parameters make it possible to comprehensively assess the condition of the hard tissues of the teeth, the level of daily hygiene and the presence of inflammatory changes in the periodontium [2,7]. Oral hygiene and the severity of diseases in children with visual impairment are noticeably worse, which is partly explained by difficulties in self—care - almost half of them (49.16%) did not adhere to any specific dental cleaning technique [3,12]. In addition, insufficient parental awareness and lack of professional recommendations contribute to the unfavorable state of the oral cavity [5,8,16]. A multivariate analysis confirmed that the use of fluoride, the frequency of brushing teeth and the level of education of parents significantly affect the experience of caries. [6,9]. These data strongly emphasize the need for targeted preventive measures and wider integration of visually impaired children into national oral health programs. The timing of one and three months is determined by the need to identify both the early and fixed effect of the program. The first control examination allows you to record the initial changes associated with increased motivation and activation of hygiene skills, and the second — to assess the sustainability of the results obtained and their impact on the stabilization of dental statu [11,15].
2. Materials and Methods
- Prior to the start of the adapted treatment and prevention program, 120 visually impaired children aged 7 to 12 years underwent a comprehensive dental examination, which included an assessment of the condition of the hard tissues of the teeth, the level of oral hygiene and periodontal health. The data obtained indicated that the dental status of the majority of participants was at a level requiring targeted intervention. The average value of the caries prevalence index (DMFT) was 2.50 ± 0.7, reflecting the high prevalence of the carious process in the group. At the same time, component D (untreated carious teeth) prevailed — 1.72 units on average, which indicates insufficient coverage of timely treatment. Component M (teeth removed due to caries) The minimum value was 0.18, and component F (filled teeth) was 0.60, which may indicate both insufficient availability of dental care and a low level of preventive visits.The oral hygiene index (OHI-S) averaged 2.30 ± 0.4, which corresponds to a satisfactory but far from optimal level. More than half of the children (54.2%) were in the category of "satisfactory hygiene", a third (31.7%) were in the category of "poor hygiene", and only 14.1% demonstrated a "good" level of cleanliness of dental surfaces. The incidence of bleeding gums (BOP) reached 36.0%, which indicates the presence of inflammatory changes in periodontal disease in a significant proportion of children. In most cases, bleeding was recorded in the molars and premolars, which is probably due to the inaccessibility of these areas during self-cleaning and insufficient parental supervision. Taken together, these data highlight the need to implement a comprehensive program aimed at developing sustainable hygiene habits, increasing parental control, and improving the availability of preventive dental services. The high proportion of untreated carious teeth, insufficient hygiene and frequent signs of periodontal inflammation create the prerequisites for further deterioration of dental health if timely and targeted measures are not taken.Dynamics after 1 month. A repeat examination conducted one month after the start of the implementation of the adapted treatment and prevention program revealed positive changes in all evaluated clinical indicators, with the exception of the DMFT index, which demonstrates a slow dynamics of changes. The average DMFT value decreased from 2.50 ± 0.7 to 2.48 ± 0.7, which is not statistically significant, but reflects the beginning of the process of reducing component D (untreated carious teeth) from 1.72 to 1.70 due to timely treatment of the detected lesions. Component F (filled teeth) increased from 0.60 to 0.63, which indicates active intervention and elimination of existing carious cavities.The most noticeable changes occurred in the indicators of oral hygiene. The average OHI-S index decreased from 2.30 ± 0.4 to 1.95 ± 0.3, which corresponds to the transition of a significant proportion of children from the category of "poor hygiene" to "satisfactory". The proportion of children with a good level of hygiene increased from 14.1% to 26.7%. This improvement is explained by regular parental supervision, motivational conversations, as well as the use of visual and tactile teaching methods recommended in programs for visually impaired children.An important achievement was to increase awareness among the children themselves: during oral interviews, many could explain why it was necessary to brush your teeth twice a day, why it was important to use a fluoride paste, and how cleaning your tongue helped keep your breath fresh. Thus, the program had a comprehensive impact it formed not only new skills, but also a motivational base for their long-term preservation.
|
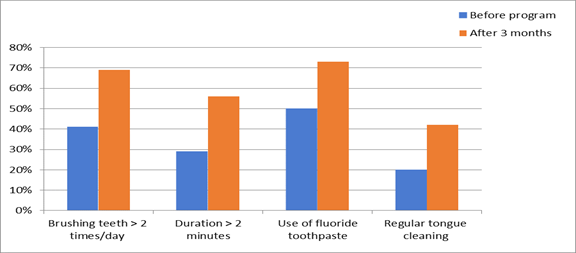 | Figure 1. Changes in hygiene habits before and after the implementation of the program (n = 120) |
3. Conclusions
- Taken together, these results confirm that an adapted therapeutic and preventive program, including sensory learning methods, motivational conversations, active parental involvement and regular monitoring, can not only quickly improve dental health, but also consolidate the achieved effect. Three months after the start of the intervention, most of the participants showed a significant decrease in plaque levels, a decrease in periodontal inflammation, and a stabilization of carious status.The analysis showed that the introduction of an adapted therapeutic and preventive program not only improved the dental health of children with visual impairment, but also had a significant positive impact on their emotional state. Three months after the start of the program, the proportion of children with high levels of anxiety had almost halved, while the number of participants with low levels of anxiety had more than doubled.These changes are especially important because reducing anxiety increases a child's willingness to cooperate with a doctor, reduces the need for additional behavioral management methods, and creates favorable conditions for preventive and curative measures. The results obtained confirm that the integration of sensory adaptations, psychological support and gradual adaptation to the dental environment is an effective strategy for working with visually impaired children.