-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(5): 2516-2521
doi:10.5923/j.ajmms.20261605.52
Received: Apr. 28, 2026; Accepted: May 17, 2026; Published: May 21, 2026

Diagnostic and Prognostic Value of Hormonal Profile Parameters in Women with Folliculogenesis Disorders
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAkhmadzhanova M. A., Shukurov F. I.
Tashkent State Medical University, Tashkent, Uzbekistan
Correspondence to: Shukurov F. I., Tashkent State Medical University, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Introduction. Folliculogenesis disorders are among the major causes of female infertility, as they impair oocyte maturation, ovulation, and ovarian reserve. Evaluation of hormonal profile parameters may provide valuable diagnostic and prognostic information for the early detection of these reproductive disturbances. Objective. To evaluate the diagnostic and prognostic value of hormonal profile parameters in women with folliculogenesis disorders. Materials and Methods. This prospective comparative clinical and laboratory study included a total of 120 women of reproductive age. The participants were divided into four groups: Group I comprised 30 women of early reproductive age with folliculogenesis disorders; Group II included 30 women of middle reproductive age with folliculogenesis disorders; Group III consisted of 30 women of late reproductive age with folliculogenesis disorders; and the control group included 30 healthy women with preserved reproductive function. Serum levels of follicle-stimulating hormone (FSH), luteinizing hormone (LH), estradiol, progesterone, and anti-Müllerian hormone (AMH) were determined using enzyme-linked immunosorbent assay (ELISA). Transvaginal ultrasonography was performed to assess antral follicle count (AFC), dominant follicle formation, and endometrial thickness. Correlation and ROC analyses were carried out. Results: FSH levels were significantly higher in the study groups than in the control group, whereas AMH, estradiol, and progesterone levels were significantly lower. A strong positive correlation was found between AMH and AFC (r = 0.71; p < 0.001), while FSH demonstrated a negative correlation with AFC (r = –0.64; p < 0.001). ROC analysis showed that AMH had the highest diagnostic value, with an AUC of 0.89, whereas FSH demonstrated an AUC of 0.84. Conclusion: Comprehensive assessment of AMH, FSH, and progesterone in combination with echographic parameters has high clinical significance for the early detection of folliculogenesis disorders and for determining reproductive prognosis.
Keywords: Folliculogenesis, Hormonal profile, AMH, FSH, Ovarian reserve, Diagnosis, Prognosis
Cite this paper: Akhmadzhanova M. A., Shukurov F. I., Diagnostic and Prognostic Value of Hormonal Profile Parameters in Women with Folliculogenesis Disorders, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2516-2521. doi: 10.5923/j.ajmms.20261605.52.
Article Outline
1. Introduction
- Infertility is currently recognized as one of the most important medical and social challenges in global healthcare. According to the World Health Organization, approximately one in six people worldwide experiences infertility during their lifetime [1]. Within the structure of female infertility, ovulatory and folliculogenetic disorders occupy a special place, as oocyte maturation, dominant follicle selection, and subsequent ovulation represent central biological stages of successful reproduction [2]. Therefore, the early identification of abnormalities in folliculogenesis, particularly through the assessment of hormonal markers, is of considerable clinical importance not only for diagnosis but also for reproductive prognosis.Folliculogenesis is a multistage and highly coordinated process that extends from the activation of primordial follicles to the formation of a preovulatory follicle. This process depends not only on the activity of the hypothalamic-pituitary-ovarian axis, but also on local autocrine and paracrine interactions among the oocyte, granulosa cells, and theca cells [3]. Current evidence indicates that granulosa cells constitute the principal steroidogenic and regulatory component within the follicle, while their functional state directly influences follicular growth, dominant follicle selection, and oocyte competence [4].The endocrine regulation of folliculogenesis is primarily mediated by follicle-stimulating hormone (FSH), luteinizing hormone (LH), estradiol, and progesterone. FSH stimulates granulosa cell proliferation, aromatase activity, and antral follicle growth, whereas LH enhances androgen synthesis in theca cells, with subsequent conversion of androgens into estrogens within the granulosa layer [5]. Estradiol, in turn, serves as one of the key mediators of dominant follicle selection and transition to the preovulatory stage. In recent years, however, increasing attention has been paid to the role of LH not only in later stages but also in early folliculogenesis, further underscoring the need for a comprehensive evaluation of the hormonal profile when interpreting folliculogenesis disorders [6].In clinical reproductology, anti-Müllerian hormone (AMH) has become one of the most widely used biomarkers for the assessment of ovarian reserve. AMH is mainly produced by granulosa cells of preantral and small antral follicles and indirectly reflects the functional status of the follicular pool [7]. Nevertheless, interpretation of AMH alone is not always sufficient. Conventional hormones such as FSH, LH, estradiol, and progesterone also provide clinically relevant information for evaluating reproductive potential. In particular, elevated basal FSH is regarded as a relatively late but clinically significant indicator of declining ovarian function, whereas the LH/FSH ratio may help differentiate certain ovulatory disorders. Current evidence suggests that antral follicle count (AFC) and AMH have greater informative value than day-3 FSH for the assessment of ovarian reserve; however, combining laboratory and instrumental indicators appears more appropriate for improving prognostic accuracy [8].Although the physiology of folliculogenesis, the clinical significance of AMH, and the utility of ovarian reserve testing have been widely discussed in the literature, relatively few studies have specifically addressed the comprehensive evaluation of the diagnostic and prognostic value of hormonal profile parameters in women with folliculogenesis disorders. In particular, the relationships among different hormones, their association with follicular growth and ovarian reserve markers, and the most informative marker combinations for early clinical decision-making remain insufficiently clarified. From this perspective, the present study is relevant because it aims to provide a deeper assessment of the clinical significance of hormonal profile parameters and to improve reproductive prognosis in women with folliculogenesis disorders.
2. Purpose of the Research
- The aim of the study was to comprehensively evaluate the clinical, diagnostic, and prognostic significance of hormonal profile parameters in women with folliculogenesis disorders.
3. Materials and Methods
- This study was designed as a prospective comparative clinical and laboratory investigation. A total of 120 women of reproductive age were enrolled. According to age characteristics and clinical status, the participants were divided into four groups: Group I included 30 women of early reproductive age (18–35 years) with folliculogenesis disorders; Group II included 30 women of middle reproductive age (36–39 years) with folliculogenesis disorders; Group III included 30 women of late reproductive age (40–43 years) with folliculogenesis disorders; and the control group consisted of 30 healthy women with preserved reproductive function.The inclusion criteria were as follows: reproductive age, clinically and instrumentally confirmed folliculogenesis disorder, and voluntary written informed consent to participate in the study.The exclusion criteria included organic ovarian diseases, severe somatic and endocrine pathologies, oncological diseases, acute inflammatory processes, and a history of hormonal drug use within the previous 3 months.General clinical and anamnestic data were collected from all participants, including age, age at menarche, characteristics of the menstrual cycle, reproductive history, gynecological and somatic diseases, previous surgical interventions, as well as the duration and type of infertility. At the main stage of the study, serum levels of the following reproductive hormones were determined: follicle-stimulating hormone (FSH), luteinizing hormone (LH), estradiol (E2), progesterone, and anti-Müllerian hormone (AMH).Hormonal assessment was performed during functionally significant phases of the menstrual cycle. FSH, LH, estradiol, and AMH were measured during the early follicular phase, on days 3–5 of the cycle, whereas progesterone was assessed during the luteal phase, usually on days 21–23. Blood samples were collected in the morning under fasting conditions in accordance with standard aseptic procedures. Hormone concentrations were determined by enzyme-linked immunosorbent assay (ELISA).All participants underwent transvaginal ultrasonography of the pelvic organs. During the examination, ovarian volume, stromal condition, antral follicle count (AFC), dominant follicle formation, endometrial thickness, and endometrial structure were assessed. Ultrasonographic findings were analyzed in relation to hormonal parameters. Folliculogenesis disorder was diagnosed on the basis of the following criteria: absence or delay of dominant follicle formation, arrest of follicular growth, signs of anovulation, changes in antral follicle count, and deviations of FSH, LH, AMH, estradiol, and progesterone levels from normal values.The obtained data were processed using modern statistical methods. Distribution patterns, mean values, and standard deviations were calculated. Intergroup differences were assessed using parametric and non-parametric methods. Correlation analysis was performed to determine the relationships between hormonal parameters and instrumental markers of folliculogenesis. ROC analysis was applied to evaluate diagnostic and prognostic significance. In addition, a group-wise bubble scatter plot was constructed to visualize the relationship between mean AMH, AFC, and FSH values across the study groups. Statistical significance was accepted at p < 0.05.The study was conducted in accordance with established bioethical principles. Written informed consent was obtained from all participants, and the confidentiality of personal data was ensured throughout the study.
4. Results
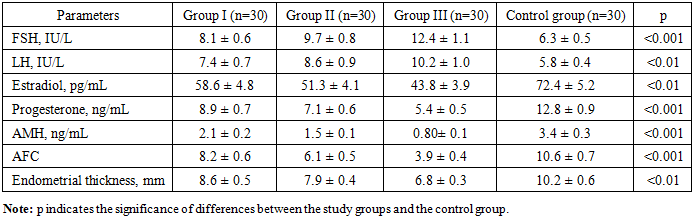
- During the study, differences in hormonal profile parameters were identified in women with folliculogenesis disorders according to reproductive age stage. Although endocrine alterations in women of early, middle, and late reproductive age followed a similar pattern, their severity increased progressively with advancing age. In the control group, hormonal parameters remained within physiological ranges, whereas the study groups demonstrated significant laboratory shifts reflecting follicular growth disturbances, ovulatory dysfunction, and impaired ovarian reserve.Comparative analysis of the hormonal profile across the groups showed that serum FSH levels were 8.1 ± 0.6 IU/L in Group I, 9.7 ± 0.8 IU/L in Group II, and 12.4 ± 1.1 IU/L in Group III, compared with 6.3 ± 0.5 IU/L in the control group (p < 0.001). LH levels were also elevated in the study groups compared with the control group. Specifically, LH concentrations were 7.4 ± 0.7 IU/L in Group I, 8.6 ± 0.9 IU/L in Group II, and 10.2 ± 1.0 IU/L in Group III, whereas the control value was 5.8 ± 0.4 IU/L (p < 0.01). Estradiol levels demonstrated a decreasing trend in women with folliculogenesis disorders: 58.6 ± 4.8 pg/mL in Group I, 51.3 ± 4.1 pg/mL in Group II, and 43.8 ± 3.9 pg/mL in Group III, compared with 72.4 ± 5.2 pg/mL in the control group (p < 0.01).Progesterone levels were also significantly lower in the study groups. The values were 8.9 ± 0.7 ng/mL in Group I, 7.1 ± 0.6 ng/mL in Group II, and 5.4 ± 0.5 ng/mL in Group III, whereas the control group showed a value of 12.8 ± 0.9 ng/mL (p < 0.001). Anti-Müllerian hormone showed the most pronounced differences. AMH levels were 2.1 ± 0.2 ng/mL in Group I, 1.5 ± 0.1 ng/mL in Group II, and 0.80 ± 0.1 ng/mL in Group III, compared with 3.4 ± 0.3 ng/mL in the control group (p < 0.001) (Table 1).
|
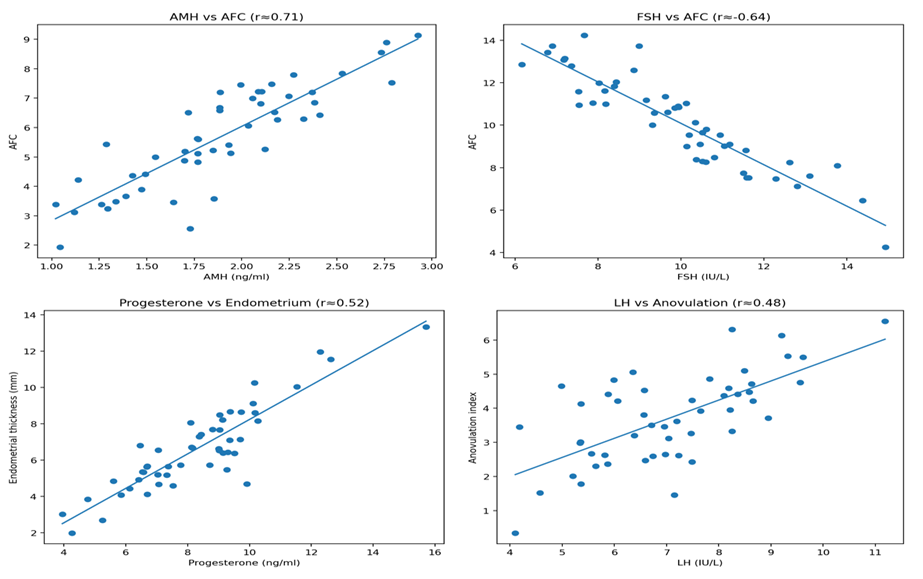 | Figure 1. Correlation between hormonal parameters and instrumental markers of folliculogenesis |
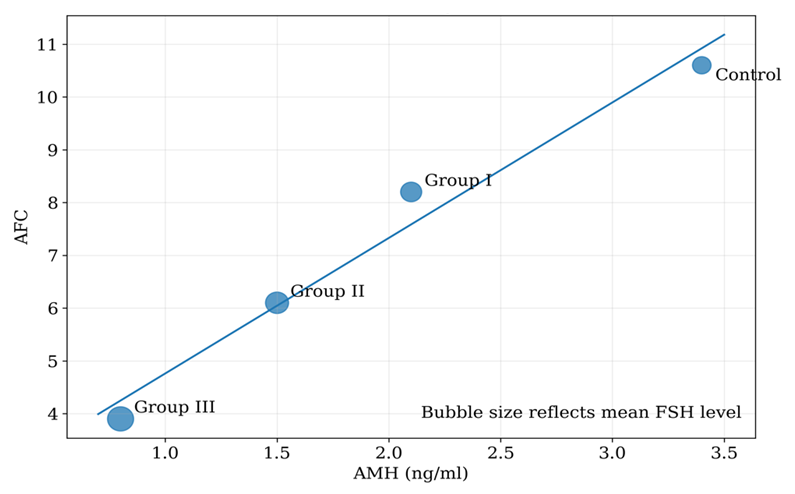 | Figure 2. Group-wise relationship between AMH, AFC and FSH levels in women with folliculogenesis disorders |
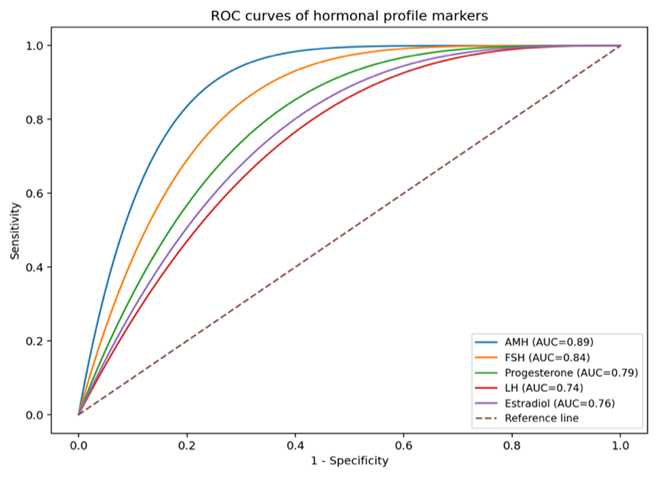 | Figure 3. ROC analysis of the diagnostic value of hormonal profile parameters in detecting folliculogenesis disorders |
5. Discussion
- The findings of the present study demonstrated complex pathogenetic relationships between hormonal profile parameters and indices of ovarian function in women with folliculogenesis disorders. The obtained data confirm that advancing reproductive age is accompanied by a progressive decline in ovarian reserve and increasing endocrine imbalance. This observation is consistent with previous studies showing restructuring of the hypothalamic-pituitary-ovarian axis during ovarian aging [3,8,11].In our study, elevated FSH levels were associated with diminished ovarian reserve. This is in agreement with the data reported by di Clemente et al., who described compensatory increases in gonadotropin secretion in the setting of declining ovarian reserve [11]. In addition, the negative correlation between FSH and AFC (r = -0.64) is well supported in the literature and reflects depletion of the follicular pool.The decrease in AMH levels and its strong positive correlation with AFC (r = 0.71) further confirm that this hormone is one of the most reliable markers for the assessment of ovarian reserve. Previous studies by Cedars [3], Moolhuijsen and Visser [8], and di Clemente et al. [11] have also identified AMH as a dependable biomarker reflecting follicle number and ovarian function. Moreover, age-related decline in AMH has been directly linked to a reduction in reproductive potential.The group-wise bubble scatter plot additionally confirmed this pattern, showing that lower AMH and AFC values were accompanied by higher FSH levels across the patient groups, particularly in women of late reproductive age.The decrease in progesterone levels and its positive correlation with endometrial thickness indicate that luteal phase insufficiency adversely affects implantation potential. These findings suggest that adequate luteal hormonal support plays an important role in maintaining endometrial receptivity and favorable reproductive conditions.The increase in LH levels and its association with anovulatory conditions indicate that pituitary hormonal imbalance plays a significant role in ovulatory dysfunction. This is particularly consistent with pathogenetic models observed in conditions such as polycystic ovary syndrome, where LH hypersecretion contributes to impaired ovulation.ROC analysis demonstrated the high diagnostic performance of AMH (AUC = 0.89) and FSH (AUC = 0.84). Previous studies have likewise confirmed the high diagnostic performance of AMH in the assessment of ovarian reserve, supporting its clinical value as a sensitive and specific marker [7,8,10,11]. FSH, while somewhat less powerful, remains a clinically meaningful parameter for diagnostic assessment.At the same time, the moderate AUC values of progesterone, LH, and estradiol indicate that these hormones are primarily of additional value in the assessment of functional disturbances. This finding underscores the importance of evaluating the hormonal profile in an integrated rather than isolated manner.The present results also showed that combined analysis of hormonal and echographic parameters provides high efficiency for early detection of folliculogenesis disorders and for the assessment of reproductive prognosis. This approach is consistent with the modern concept of individualized diagnosis and management in reproductive medicine.Nevertheless, the study has certain limitations. The relatively small sample size and the single-center design may limit the generalizability of the findings. Future multicenter studies involving larger populations are warranted to further validate these results.
6. Conclusions
- Hormonal profile parameters in women with folliculogenesis disorders change consistently across reproductive age stages, and these alterations become more pronounced with advancing age. Increased FSH levels, decreased AMH concentrations, and progesterone deficiency represent the main endocrine features reflecting impaired follicular function, diminished ovarian reserve, and disrupted ovulatory mechanisms. The strong positive correlation between AMH and AFC, as well as the negative correlation between FSH and ovarian reserve indicators, confirms the pathogenetic relationship between hormonal and echographic parameters. Comprehensive assessment of AMH, FSH, progesterone, and echographic markers has high clinical significance for early diagnosis, individual risk stratification, and prediction of reproductive outcomes in women with folliculogenesis disorders.