-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(5): 2501-2510
doi:10.5923/j.ajmms.20261605.50
Received: Apr. 24, 2026; Accepted: May 17, 2026; Published: May 20, 2026

Artificial Intelligence in Hysteroscopic Imaging: A Narrative Review of Current Developments and Future Perspectives
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKhudoyarova Dildora Rakhimovna1, Musayeva Malika Shakhobovna2
1DSc, Professor, Samarkand State Medical University, Samarkand, Uzbekistan
2Obstetrician-Gynecologist, Freelance Applicant, Samarkand State Medical University, Samarkand, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Artificial intelligence (AI) is increasingly transforming medical imaging by enhancing diagnostic accuracy and reducing observer variability. In hysteroscopy, interpretation remains largely dependent on subjective visual assessment, highlighting the need for objective decision-support tools. This narrative review analyzes current developments in AI-assisted hysteroscopic imaging, summarizes evidence from related gynecologic and endoscopic applications, and evaluates existing limitations. While preliminary studies demonstrate technical feasibility, large-scale validation and standardized datasets are still lacking. Ongoing digital health reforms in CIS countries, including Uzbekistan, create favorable conditions for future implementation. AI-assisted hysteroscopy represents a promising direction toward more standardized and objective diagnosis of endometrial pathology.
Keywords: Artificial intelligence, Hysteroscopy, Endometrial pathology, Gynecologic imaging, Deep learning, Computer vision, Video analysis, Clinical decision support systems
Cite this paper: Khudoyarova Dildora Rakhimovna, Musayeva Malika Shakhobovna, Artificial Intelligence in Hysteroscopic Imaging: A Narrative Review of Current Developments and Future Perspectives, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2501-2510. doi: 10.5923/j.ajmms.20261605.50.
1. Introduction
- Hysteroscopy remains the gold standard for the direct visualization of the uterine cavity and plays a pivotal role in the diagnosis of endometrial hyperplasia, polyps, submucosal fibroids, and early-stage endometrial carcinoma. Despite technological improvements in optics and image resolution, diagnostic interpretation in hysteroscopy largely depends on the clinician’s subjective visual assessment, experience, and training level. Interobserver variability in the evaluation of endometrial patterns remains a significant clinical issue, particularly in borderline or early malignant lesions [2,9].The growing global burden of endometrial pathology, including endometrial cancer, further underscores the need for improved diagnostic accuracy and reproducibility. According to recent global cancer statistics, endometrial cancer incidence continues to rise worldwide, emphasizing the importance of early and precise detection strategies [3]. In this context, optimization of visual diagnostic methods, including hysteroscopy, is of high clinical relevance.Over the past decade, artificial intelligence (AI) has emerged as a transformative force in medical imaging. Advances in machine learning and deep learning, particularly convolutional neural networks (CNNs), have demonstrated remarkable performance in radiology, digital pathology, and endoscopic imaging [6,14]. AI-assisted systems have already shown the ability to improve detection rates, reduce missed lesions, and enhance diagnostic standardization in gastrointestinal endoscopy [15]. These achievements suggest that similar approaches may be successfully adapted for hysteroscopic imaging.The transition from subjective interpretation to algorithm-assisted objective evaluation represents a paradigm shift in visual diagnostics. AI systems are capable of analyzing complex image features, including texture, vascular patterns, color distribution, and dynamic changes in video streams—parameters that may be inconsistently perceived by human observers. In addition, real-time video analysis has become increasingly feasible due to improvements in computational power and optimized neural network architectures [6].In gynecology, AI applications have expanded rapidly in ultrasound diagnostics, reproductive medicine, and oncological risk stratification [1,10,13]. Recent literature from Central Asia and CIS countries indicates growing interest in AI implementation in gynecologic oncology and reproductive health, though large-scale validated systems in hysteroscopy remain scarce [4,8,11,12]. Emerging discussions within the region highlight AI as a strategic tool for future clinical development rather than merely an experimental technology [7]. In Uzbekistan, ongoing healthcare reforms focused on digital transformation, telemedicine, and innovation in medical education create a favorable environment for integrating AI-based diagnostic tools. While telemedicine and digital health infrastructure are actively developing [17], AI-assisted hysteroscopic systems have not yet been widely implemented, indicating both a gap and an opportunity for research and innovation.Given these considerations, hysteroscopy represents a particularly suitable domain for AI integration. The procedure generates high-resolution visual data in a controlled anatomical environment, making it technically compatible with computer vision methodologies. However, current evidence remains fragmented, and comprehensive synthesis of available studies is needed.The objective of this narrative review is to critically analyze the current state of artificial intelligence applications in hysteroscopic imaging, evaluate the available clinical evidence and technological approaches, identify existing limitations and research gaps, and explore future perspectives for transitioning from subjective visual interpretation toward objective, algorithm-assisted diagnostic support in endometrial pathology.
2. Methods of Literature Review
- This narrative review was conducted to synthesize current evidence regarding the application of artificial intelligence (AI) in hysteroscopic imaging and related fields. A comprehensive literature search was performed in the electronic databases PubMed/MEDLINE, Scopus, Web of Science, and Google Scholar covering the period from January 2015 to March 2025. The search strategy combined Medical Subject Headings (MeSH) and free-text terms including “hysteroscopy,” “artificial intelligence,” “machine learning,” “deep learning,” “computer vision,” “endometrial pathology,” “endometrial cancer,” “gynecologic imaging,” and “AI-assisted endoscopy.”Eligible publications included original clinical studies, pilot investigations, validation studies, systematic reviews, meta-analyses, position statements, and consensus recommendations addressing AI-based image or video analysis in hysteroscopy or closely related endoscopic and gynecologic imaging domains. Studies focusing on gastrointestinal endoscopy, digital pathology, radiologic imaging, and other AI-driven diagnostic modalities were also included when they provided transferable methodological insights applicable to hysteroscopic imaging [6,14,15].Publications were excluded if they were editorials without analytical content, non-peer-reviewed opinion pieces, conference abstracts without full-text availability, or studies published prior to 2015 unless considered foundational for contextual understanding.Special attention was given to research conducted in the Commonwealth of Independent States (CIS) and Central Asia, including Uzbekistan, to assess regional progress in AI integration within gynecology and digital health systems [4,8,11,12,17]. For non-English publications, titles and bibliographic information were translated into English for citation consistency, with the original language indicated in brackets in the reference list. Given the narrative nature of the review, formal meta-analytic statistical synthesis was not performed. Instead, studies were qualitatively analyzed and thematically grouped according to: (1) technological methodology, (2) clinical application domain, (3) diagnostic performance, and (4) implementation challenges. This approach allowed for comprehensive evaluation of both technological developments and their translational relevance to hysteroscopic practice. The initial literature search identified 146 publications. After removal of duplicates and screening of titles and abstracts, 58 articles underwent full-text evaluation. Finally, 32 publications were included in the narrative synthesis, including original studies, systematic reviews, consensus statements, and methodological papers related to AI-assisted gynecologic and endoscopic imaging. The review was structured in accordance with the principles of the SANRA (Scale for the Assessment of Narrative Review Articles) framework to improve methodological transparency and narrative review quality.
3. Results
- Artificial intelligence (AI) in medical imaging refers to computational systems capable of recognizing patterns, extracting clinically relevant features, and supporting diagnostic decision-making from visual data. Over the past decade, rapid advances in computational power, availability of annotated medical datasets, and development of deep learning architectures have significantly expanded the clinical applicability of AI in image and video analysis [6,14].From Machine Learning to Deep LearningTraditional machine learning (ML) approaches in medical imaging relied on manually engineered features such as texture descriptors, color distribution, and geometric parameters selected by experts for subsequent classification. Although these methods demonstrated utility in controlled datasets, their performance was often limited by restricted generalizability and dependence on predefined feature extraction strategies.The emergence of deep learning (DL), particularly convolutional neural networks (CNNs), significantly expanded the capabilities of medical image analysis. Unlike conventional ML algorithms, CNNs automatically learn hierarchical image features directly from raw image data, enabling improved lesion detection, segmentation, and classification [6,14]. In radiology, digital pathology, and gastrointestinal endoscopy, deep learning systems have achieved diagnostic performance comparable to expert assessment in selected tasks [3,5,15].In gynecologic imaging, AI-based approaches have already demonstrated clinical utility in ultrasound diagnostics, reproductive medicine, and oncologic risk assessment [1,10,13]. These advances provide an important methodological foundation for the future development of AI-assisted hysteroscopic imaging.Convolutional Neural Networks and Image ClassificationConvolutional neural networks are currently the dominant deep learning architecture for medical image analysis because of their ability to identify spatial patterns associated with tissue morphology, vascular architecture, and surface irregularities. In endoscopic imaging, CNN-based systems have demonstrated high accuracy in lesion detection and characterization, particularly in colorectal neoplasia [15].These developments are directly relevant to hysteroscopy, where subtle visual abnormalities may indicate atypical hyperplasia or early malignant transformation. Beyond simple binary classification, modern CNN models can support multiclass lesion categorization, segmentation of suspicious regions, and probability-based risk estimation, thereby improving diagnostic standardization and support clinical decision-making.However, current hysteroscopic AI studies remain limited by relatively small datasets, retrospective study designs, and insufficient external validation, restricting the generalizability of reported performance metrics.Video-Based AI and Real-Time ProcessingUnlike static imaging modalities, hysteroscopy generates continuous video data, introducing additional analytical complexity. Video-based AI models must account for temporal information, motion artifacts, variable lighting conditions, and dynamic changes in tissue appearance.Recent developments in video-based deep learning—including recurrent neural networks (RNNs), long short-term memory (LSTM) models, and transformer-based architectures—enable the integration of temporal context into diagnostic algorithms. In gastrointestinal endoscopy, real-time AI-assisted systems have successfully demonstrated frame-by-frame lesion detection during live procedures [15].The ability to process video streams in real time is particularly relevant for hysteroscopy, where intraoperative decision-making may influence biopsy targeting or therapeutic intervention. However, successful implementation requires standardized imaging protocols, robust dataset annotation, and external clinical validation.Explainable AI and Clinical InterpretabilityInterpretability remains a critical requirement for clinical implementation of artificial intelligence systems. Deep learning models are frequently criticized for their “black-box” nature, which may reduce clinician trust and complicate regulatory approval. Explainable AI (XAI) methods, including saliency maps, heat maps, and attention-based visualization techniques, aim to improve transparency by identifying image regions that contribute most strongly to algorithmic predictions [3,5]. In hysteroscopic imaging, such approaches may be particularly valuable because visual pattern recognition remains central to gynecologic diagnostic practice and specialist training.Nevertheless, standardized frameworks for explainability in hysteroscopic AI have not yet been established, and the clinical utility of these methods requires further validation.Data Quality, Validation, and Clinical TranslationRecent medical AI research increasingly emphasizes that algorithmic performance depends not only on model architecture but also on data quality, diversity, and external validation [6,14]. Studies have shown that models trained on limited or homogeneous datasets may fail when applied to new populations or imaging systems.For hysteroscopic AI development, this implies the necessity of:• multicenter data collection,• standardized annotation protocols verified by histopathology,• robust validation cohorts, and• transparent reporting of performance metrics (sensitivity, specificity, AUC, calibration).International discussions in digital medicine highlight that clinical integration requires not only technical robustness but also regulatory compliance, workflow compatibility, and clinician acceptance [6].In summary, modern artificial intelligence technologies—particularly deep learning and video-based neural architectures—provide powerful tools for objective analysis of medical images. While successful implementation has already been demonstrated in radiology, pathology, and gastrointestinal endoscopy, adaptation to hysteroscopic imaging requires consideration of gynecologic-specific variability, standardized datasets, and clinically validated frameworks. These technological foundations establish the basis for future development of AI-assisted hysteroscopy and the transition from subjective interpretation to objective diagnostic support.Current Applications of AI in Gynecologic ImagingThe integration of artificial intelligence (AI) into gynecologic imaging has expanded substantially over the past decade, particularly in ultrasound diagnostics, digital pathology, reproductive medicine, and gynecologic oncology. Although direct applications in hysteroscopic imaging remain limited, advances in related imaging modalities provide both methodological foundations and clinical evidence supporting future implementation.Ultrasound is the most widely used imaging modality in gynecology, and consequently, it has become a primary field for AI implementation. Deep learning models have demonstrated high performance in automated measurement of endometrial thickness, classification of ovarian masses, and prediction of malignancy risk [1,10,13].AI-based ultrasound systems assist in segmentation of endometrial borders, texture analysis, and vascular pattern recognition—parameters that are also relevant in hysteroscopic visualization. Studies have shown that machine learning models can improve diagnostic consistency and reduce operator dependency, particularly in less experienced clinicians [1,13].In gynecologic oncology, AI-driven ultrasound models have been developed to differentiate benign from malignant adnexal masses with performance comparable to expert examiners [10]. These developments illustrate how pattern-recognition algorithms can enhance objective assessment in imaging modalities traditionally dependent on operator skill.Digital pathology has become one of the most successful domains for AI in gynecology. Deep learning algorithms have been applied to whole-slide histopathological images for classification of endometrial hyperplasia and endometrial carcinoma [5]. Such systems can analyze cellular architecture, nuclear atypia, and glandular complexity at a scale not feasible for manual assessment.The relevance of these advances to hysteroscopy lies in the integration of multimodal diagnostics. Combining hysteroscopic image analysis with histopathology-based AI systems may enable improved biopsy targeting and more accurate preoperative risk stratification. This integrative approach aligns with current trends in precision medicine and data-driven clinical decision-making [3].AI applications in gynecologic oncology extend beyond imaging into risk prediction models, genomic analysis, and outcome forecasting. Machine learning models have been developed for early detection of gynecologic cancers, including endometrial malignancies [4].Recent literature from Central Asia and CIS countries indicates increasing attention to AI-assisted early cancer detection strategies, although large-scale validated systems remain limited [4,8]. These regional initiatives reflect growing recognition of AI as a tool for improving oncologic screening and diagnostic pathways.In addition, AI-based decision-support systems are being explored for endometriosis management and personalized treatment planning [7]. These examples demonstrate the broader applicability of AI in gynecology and reinforce the feasibility of extending similar methodologies to hysteroscopic imaging.Reproductive medicine has become a rapidly advancing area for AI implementation. Machine learning models have been used to predict in vitro fertilization (IVF) outcomes, assess embryo quality, and evaluate endometrial receptivity [10].The success of AI in embryo image analysis and time-lapse video assessment illustrates the capability of deep learning systems to process dynamic visual data—an ability directly relevant to hysteroscopic video interpretation. Moreover, the transition from static morphological grading to objective algorithm-based scoring in reproductive medicine parallels the potential evolution of hysteroscopy from subjective visualization to quantitative analysis.In the CIS region and Uzbekistan, AI research in gynecology is emerging but remains primarily conceptual or pilot in nature. Recent publications discuss AI as a strategic direction for reproductive medicine, urogynecology, oncology, and telemedicine integration [4,8,11,12,17].Telemedicine expansion and digital health reforms provide infrastructural prerequisites for AI deployment [17]. However, validated AI systems specifically targeting hysteroscopic imaging have not yet been widely implemented, highlighting both a technological gap and a significant research opportunity.Overall, current applications of AI in gynecologic imaging demonstrate robust progress in ultrasound diagnostics, digital pathology, oncology, and reproductive medicine. These achievements provide compelling evidence that algorithm-assisted visual analysis can improve diagnostic objectivity and reproducibility. While hysteroscopic AI remains underdeveloped compared to other modalities, the technological foundations and clinical precedents established in related fields strongly support its future development and integration into gynecologic practice.Artificial Intelligence in Hysteroscopic ImagingArtificial intelligence (AI) in hysteroscopic imaging represents an emerging but still underdeveloped domain within gynecologic diagnostics. While AI-assisted systems have become increasingly established in gastrointestinal endoscopy and radiologic imaging [6,15], their direct application to hysteroscopy remains limited to pilot studies and early-stage investigations. Nevertheless, existing evidence suggests that hysteroscopic imaging possesses several characteristics that make it technically suitable for AI integration.Published Studies and Early Clinical EvidenceThe number of peer-reviewed studies specifically addressing AI-based analysis of hysteroscopic images is relatively small. Available research has primarily focused on static image classification rather than full video-stream analysis. In preliminary investigations, deep learning algorithms have been trained to differentiate benign from malignant endometrial lesions using labeled hysteroscopic images confirmed by histopathology [2]. These early models demonstrated promising diagnostic performance; however, sample sizes were limited, and external validation was rarely performed.More recent discussions in gynecologic literature emphasize the theoretical potential of AI in hysteroscopy as part of a broader digital transformation in reproductive and oncologic care [7,11,13]. However, most publications remain conceptual reviews rather than reports of large-scale clinical implementation.Compared to ultrasound or digital pathology, where AI validation studies include thousands of cases [5,10], hysteroscopic AI research is still at an exploratory stage. This discrepancy highlights both the novelty of the field and the need for multicenter dataset development.Most early studies rely on frame-based image analysis. While useful for proof-of-concept development, static-image approaches do not fully capture the dynamic characteristics of hysteroscopic procedures. Hysteroscopy generates continuous video data with variations in illumination, angle of visualization, fluid medium, and tissue movement.Video-based AI systems, already validated in gastrointestinal endoscopy [15], incorporate temporal information and motion consistency into lesion detection algorithms. Applying similar methodologies to hysteroscopy could enable real-time identification of suspicious vascular networks, irregular surface patterns, or atypical endometrial architecture.However, several challenges must be addressed before clinical translation becomes feasible:• standardized recording protocols;• high-quality annotated datasets;• histopathological confirmation of each labeled case;• multicenter external validation.Without these elements, algorithmic generalizability remains limited.Potential AI applications in hysteroscopy include detection and classification of:• endometrial carcinoma;• atypical hyperplasia;• benign polyps;• submucosal fibroids;• inflammatory changes.In oncologic contexts, early identification of subtle vascular irregularities may improve diagnostic sensitivity, especially in cases where visual differences are minimal [3]. Integration of AI-derived probability scores could assist clinicians in biopsy targeting and procedural decision-making.Benign pathologies may also benefit from automated pattern recognition. AI-assisted differentiation between hyperplasia and focal polypoid lesions could reduce unnecessary biopsies and improve procedural efficiency.One promising direction is multimodal integration—combining hysteroscopic AI analysis with ultrasound imaging, histopathological digital slides, and clinical risk models [5,10]. Such integration aligns with current trends in precision medicine and personalized diagnostics.For example, AI-assisted digital pathology systems already demonstrate high performance in endometrial lesion classification [5]. Linking these outputs with hysteroscopic visual analysis could create a comprehensive diagnostic framework that bridges macroscopic and microscopic evaluation.In CIS countries, including Uzbekistan, AI research in gynecology is gaining conceptual momentum but remains largely exploratory [4,8,11,12]. Publications from the region highlight the potential role of AI in oncologic screening, endometriosis management, and reproductive medicine [7,13]. However, clinically validated AI systems for hysteroscopic imaging have not yet been reported in large-scale practice.Digital health reforms and telemedicine expansion provide infrastructure conducive to AI deployment [17]. The absence of established AI-assisted hysteroscopy platforms in the region may therefore represent not a limitation but an opportunity for original research and leadership.Beyond diagnostic enhancement, AI-assisted hysteroscopy could serve as a training tool. Visualization overlays, lesion probability mapping, and automated feedback systems may reduce learning curves for young specialists. In regions where access to highly experienced hysteroscopists is limited, AI support could improve standardization of care. Moreover, algorithmic analysis may reduce medico-legal risks associated with diagnostic variability—a concern widely discussed in medical literature [3].In summary, artificial intelligence in hysteroscopic imaging remains at an early but promising stage of development. Preliminary studies demonstrate feasibility, and technological advances in related medical fields confirm the potential for real-time objective assessment. However, large-scale validation studies, standardized data acquisition, and regulatory frameworks are necessary before widespread clinical adoption can occur. The next stage of research must focus on video-based models, multicenter collaboration, and integration into clinical decision-support systems to achieve a meaningful transition from subjective visual interpretation to objective diagnostic support.As summarized in Table 1, currently available evidence regarding artificial intelligence in hysteroscopic imaging remains limited but increasingly promising. Most published studies are retrospective and rely on relatively small single-center datasets with predominantly internal validation. Nevertheless, preliminary investigations demonstrate that deep learning systems may achieve high diagnostic performance in detecting endometrial malignancy. The study by Takahashi et al. reported diagnostic accuracy exceeding 90%, while the recently developed ECCADx system demonstrated sensitivity of 95.2% and specificity of 91.3% in lesion classification. At the same time, substantial heterogeneity persists regarding dataset composition, annotation protocols, and validation methodology. The absence of large standardized multicenter repositories remains one of the major barriers to clinical translation. These findings indicate that AI-assisted hysteroscopy is technically feasible and clinically promising; however, prospective multicenter validation and workflow-oriented implementation studies are still required before routine adoption can be recommended.
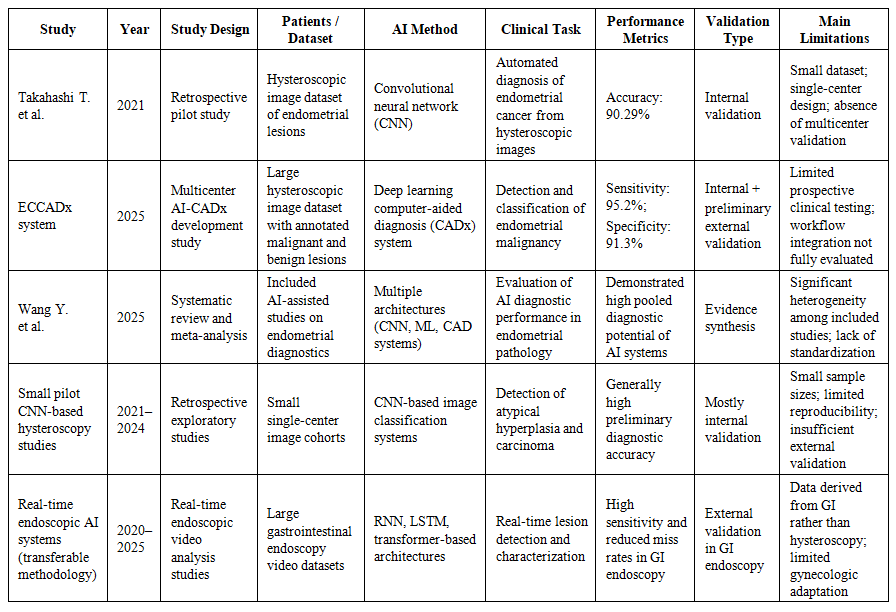 | Table 1. Published Studies on Artificial Intelligence in Hysteroscopic Imaging |
 | Table 2. Evolution of AI Methods in Medical Imaging |
 | Table 3. AI Development in CIS and Uzbekistan |
4. Conclusions
- Artificial intelligence represents a promising direction for improving diagnostic objectivity and reproducibility in hysteroscopic imaging. Although current evidence remains limited and largely exploratory, preliminary studies demonstrate the technical feasibility of AI-assisted detection and classification of endometrial pathology. Advances achieved in gastrointestinal endoscopy, radiology, and digital pathology further support the potential clinical relevance of computer-assisted hysteroscopic diagnostics [5,6,15].Future progress in this field will depend on the development of large multicenter hysteroscopic datasets with histopathologically verified annotations and standardized image acquisition protocols. Establishing unified annotation frameworks and harmonized reporting standards is essential to improve algorithm comparability, reproducibility, and external validity. Prospective multicenter validation studies should become a priority in order to evaluate algorithmic performance across diverse patient populations, imaging systems, and clinical environments.An additional promising direction involves multimodal integration of hysteroscopic imaging with digital pathology, ultrasound diagnostics, and clinical risk prediction models. Such integrated AI platforms may improve biopsy targeting, facilitate individualized risk stratification, and support precision gynecologic diagnostics.At the same time, successful clinical implementation will require the development of transparent regulatory pathways, including standards for algorithm validation, safety monitoring, explainability, and data governance. A phased implementation strategy may be most appropriate, beginning with decision-support and educational systems, followed by real-time intraoperative assistance and ultimately broader integration into routine clinical workflows.In the context of ongoing digital health reforms in CIS countries and Uzbekistan, AI-assisted hysteroscopy represents a strategically important area for future interdisciplinary research and innovation. With appropriate validation, standardization, and regulatory oversight, AI technologies may substantially reduce interobserver variability, improve early detection of endometrial pathology, and contribute to more objective and standardized gynecologic care.