-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(5): 2495-2500
doi:10.5923/j.ajmms.20261605.49
Received: Apr. 20, 2026; Accepted: May 16, 2026; Published: May 20, 2026

Independent Risk Factors for Rirs Failure in Pediatric Nephrolithiasis
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLRakhmatullaev A. A.1, 2, Isroilov A. A.1, Ruziev M. Yu.2
1Tashkent State Medical University, Tashkent, Uzbekistan
2Republican Specialized Scientific and Practical Medical Center of Pediatrics, Tashkent, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

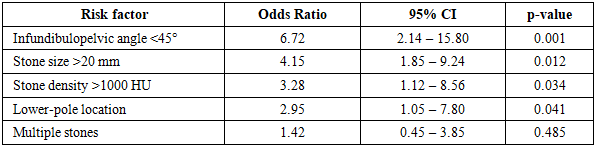
Background. No validated pediatric-specific scoring system exists to predict retrograde intrarenal surgery (RIRS) outcomes in children. This study aimed to identify independent risk factors for RIRS failure and to develop a prognostic tool for surgical decision-making. Methods. In a prospective cohort of 54 children (aged 6 months – 18 years) who underwent RIRS for renal stones, multivariate logistic regression was used to identify independent predictors of failure. A scoring system – P-RPS (Pediatric RIRS Prediction Score) – was constructed and validated by ROC analysis. Results. Three independent predictors were identified: infundibulopelvic angle <45° (OR=6.72, p=0.001), stone size >20 mm (OR=4.15, p=0.012), and stone density >1000 HU (OR=3.28, p=0.034). The P-RPS (0-5 points) achieved AUC=0.895, sensitivity 88.4%, and specificity 91.2%. A traffic-light algorithm stratified patients into green (0-1, SFR 94-98%), yellow (2-3, SFR 80-90%), and red (4-5, mini-PCNL recommended) zones. Conclusion. The P-RPS is a simple, high-accuracy predictive tool enabling personalized surgical planning in pediatric nephrolithiasis.
Keywords: P-RPS scoring system, Retrograde intrarenal surgery, Pediatric nephrolithiasis, Risk factors, Logistic regression, Stratified treatment algorithm, Infundibulopelvic angle
Cite this paper: Rakhmatullaev A. A., Isroilov A. A., Ruziev M. Yu., Independent Risk Factors for Rirs Failure in Pediatric Nephrolithiasis, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2495-2500. doi: 10.5923/j.ajmms.20261605.49.
1. Introduction
- Retrograde intrarenal surgery has emerged as one of the most promising minimally invasive approaches for managing renal calculi in children, offering the appeal of a natural-orifice technique that avoids parenchymal puncture and substantially reduces radiation exposure compared with percutaneous access [1,2]. As flexible ureteroscope technology and holmium laser systems have continued to evolve, the indications for RIRS in the pediatric population have expanded progressively, with several centers now reporting stone-free rates between 83% and 92% across a broad range of stone sizes and locations [3,4,21].Yet even the most enthusiastic proponents of the technique acknowledge that RIRS does not perform equally well in every clinical scenario. Scattered observations across the literature suggest that the infundibulopelvic angle, stone burden, and calyceal anatomy each exert an independent influence on surgical success, but the relative weight of these factors has never been formally quantified in a pediatric cohort through multivariate modeling [5,6]. In adult practice, several predictive instruments have been proposed – the Resorlu-Unsal Stone Score, the R.I.R.S. scoring system, the modified Seoul National University Renal Stone Complexity score, and the S.T.O.N.E. nephrolithometry – yet their reported discriminatory power has varied considerably, with area-under-the-curve values ranging from 0.617 to 0.868 depending on the tool and the validation cohort [7,8]. More importantly, none of these instruments was developed for or validated in the pediatric population, whose anatomical proportions, ureteral caliber, and collecting system geometry differ meaningfully from those of adults [9,10,20].The absence of a pediatric-specific predictive tool leaves surgeons in a position where the choice between RIRS and mini-percutaneous nephrolithotomy often relies on subjective clinical judgment rather than a standardized, evidence-based framework. This gap carries tangible consequences: an unsuccessful RIRS attempt means an additional anesthesia session, wasted operative resources, prolonged parental anxiety, and – in the worst case – avoidable complications for the child [2,11].The present study was designed to address this unmet need through two interconnected objectives. First, we sought to identify the independent risk factors for RIRS failure in children using multivariate logistic regression analysis. Second, we aimed to translate those statistical findings into a clinically usable prognostic scoring system – the Pediatric RIRS Prediction Score (P-RPS) – and to construct a stratified treatment algorithm capable of guiding surgical decision-making before the child reaches the operating room.
2. Methods
- This analysis draws on data from a prospective comparative cohort study conducted between 2016 and 2025 at two referral institutions in Tashkent, Uzbekistan: the Republican Specialized Pediatric Scientific-Practical Medical Center and «Centromed» Clinic. Ethical approval was obtained from the institutional review board, and written informed consent was provided by the legal guardians of all participants. The study protocol conformed to the principles of the Declaration of Helsinki.The analytical cohort for the present investigation comprised 54 consecutive children aged 6 months to 18 years who underwent RIRS for renal calculi measuring 10 to 30 mm. Children with uncorrectable coagulopathy, acute pyelonephritis, severe skeletal deformities, or staghorn calculi were excluded. Every patient underwent a uniform preoperative workup that included renal ultrasonography, non-contrast multislice computed tomography, and standard laboratory testing. From the CT datasets, the following parameters were systematically recorded for each patient: maximum stone diameter in millimeters, stone density in Hounsfield units, number and laterality of calculi, stone location within the collecting system, infundibulopelvic angle of the affected calyx, and infundibular length. The degree of pelvicalyceal dilatation was graded according to the Society for Fetal Urology classification.All RIRS procedures were performed under general endotracheal anesthesia with perioperative antibiotic prophylaxis. A ureteral access sheath (9.5-11.5 Fr) was placed in every case to maintain low intrarenal pressure. Holmium:YAG laser lithotripsy was carried out using a dusting strategy (energy 0.3-0.5 J, frequency 15-20 Hz) through an age-appropriate flexible ureteroscope. Double-J stents were inserted in all patients and removed after two to three weeks.The primary outcome was surgical failure, defined as the presence of residual fragments exceeding 4 mm on imaging at the three-month follow-up visit. Secondary outcomes included operative duration, complication rates graded by the modified Clavien-Dindo classification [12], and 12-month recurrence data. Stone-free status was assessed by ultrasonography and plain radiography at 1 to 3 days, 1 month, and 3 months after surgery.The statistical analysis proceeded in three stages. In the first stage, bivariate correlations between each candidate predictor and the binary outcome variable (success vs. failure) were calculated using Pearson's coefficient for continuous variables and point-biserial correlation for categorical ones. In the second stage, all variables reaching statistical significance (p<0.05) in the bivariate analysis were entered into a multivariate binary logistic regression model to identify independent predictors of failure. For each predictor, the odds ratio and 95% confidence interval were computed. In the third stage, the statistically significant independent predictors were used to construct the P-RPS scoring system, with point allocations proportional to the magnitude of each variable's odds ratio. The discriminatory performance of the resulting score was evaluated by receiver operating characteristic analysis, and the area under the curve, sensitivity, specificity, positive predictive value, and negative predictive value were calculated at the optimal cutoff point determined by the Youden index. All analyses were performed using IBM SPSS Statistics 26.0 and MedCalc 19.0, with significance set at p<0.05.
3. Results
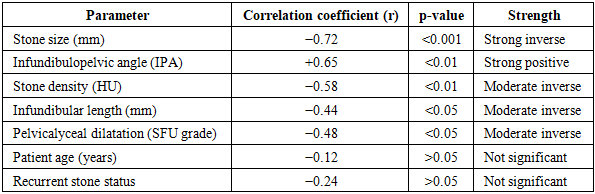
- The study cohort consisted of 54 children with a mean age of 6.8±2.9 years, of whom 31 (57.4%) were boys. Mean stone size was 16.2±5.4 mm, and mean stone density was 942±285 HU. Stones were located in the renal pelvis or upper and middle calyces in 36 patients (66.7%) and in the lower pole in 14 (25.9%), with 4 patients (7.4%) harboring multiple calculi in mixed locations. At three months, 50 of 54 patients (92.6%) had achieved stone-free status or had only clinically insignificant residual fragments, while 4 patients (7.4%) met the definition of surgical failure.Bivariate correlation analysis revealed that five clinical-anatomical variables demonstrated a statistically significant association with RIRS outcome. Stone size showed a strong inverse correlation (r=−0.72, p<0.001), the infundibulopelvic angle displayed a strong positive correlation (r=+0.65, p<0.01), stone density exhibited a moderate inverse correlation (r=−0.58, p<0.01), infundibular length demonstrated a moderate inverse correlation (r=−0.44, p<0.05), and pelvicalyceal dilatation grade showed a moderate inverse relationship (r=−0.48, p<0.05). Patient age (r=−0.12, p>0.05) and recurrent stone status (r=−0.24, p>0.05) did not reach statistical significance. These findings are detailed in Table 1.
|
|
 | Table 3. Clinical outcomes stratified by P-RPS risk category |
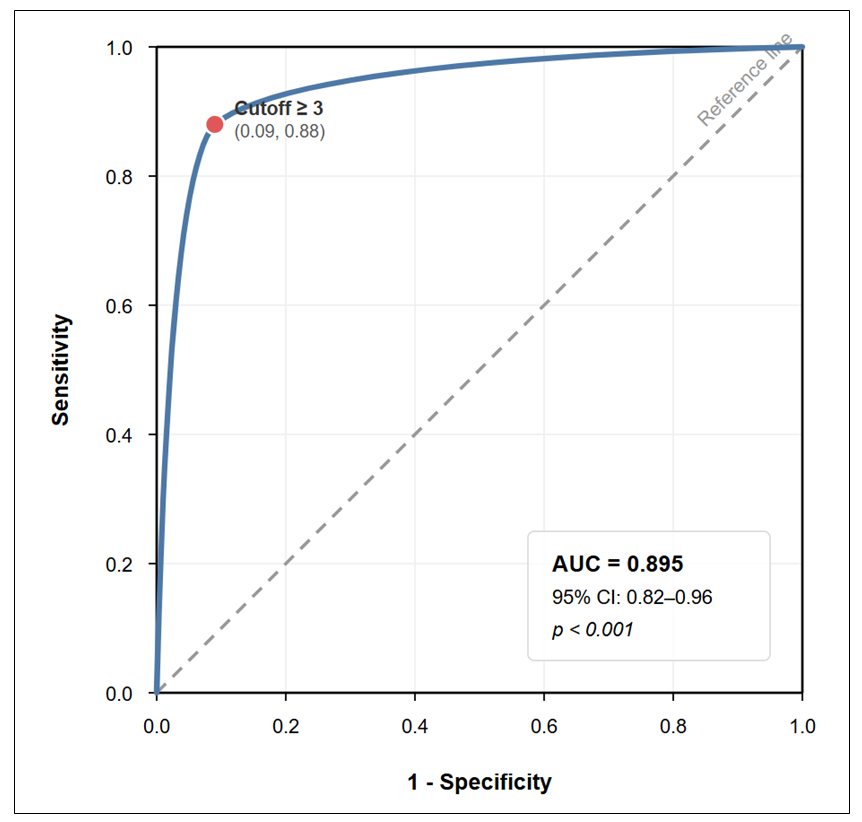 | Figure 1. ROC curve demonstrating the diagnostic performance of the P-RPS scoring system |
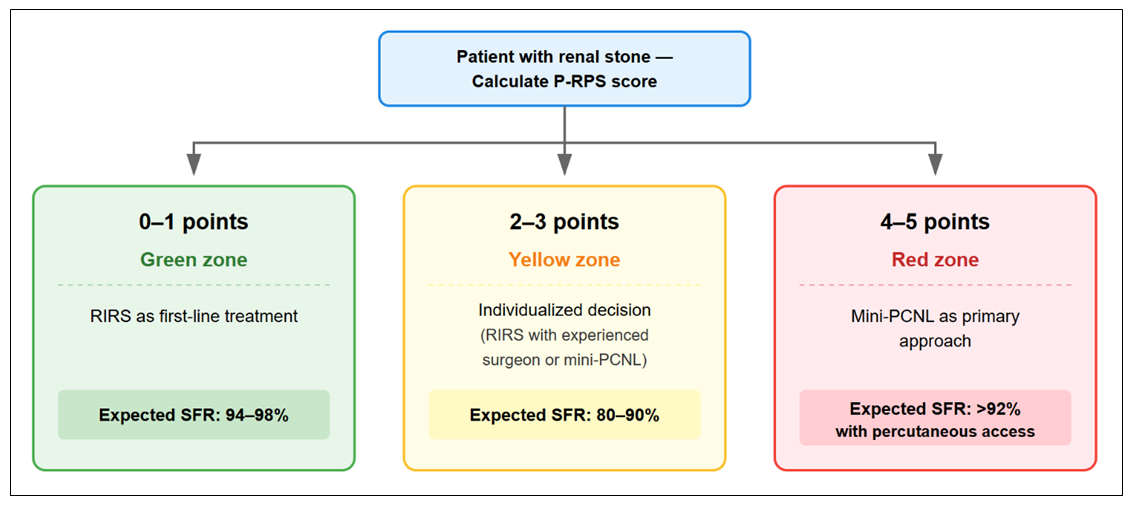 | Figure 2. P-RPS-based stratified treatment algorithm for pediatric renal stone management (traffic-light model) |
4. Discussion
- The central finding of this study is that RIRS failure in children is not a random event but rather follows a predictable pattern governed by three measurable anatomical and morphometric variables: the infundibulopelvic angle, stone size, and stone density. By integrating these predictors into a simple five-point scoring system, we were able to stratify patients into clinically meaningful risk categories that closely correspond to their expected surgical outcomes. The discriminatory power of the resulting P-RPS instrument, reflected in an AUC of 0.895, compares favorably with existing adult-focused scoring tools and – to our knowledge – represents the first validated predictive system designed specifically for the pediatric RIRS population.The hierarchy of risk factors we identified resonates with what has been reported in adult series. Resorlu and colleagues, in their original description of the RUSS, identified lower-pole location with an IPA below 45 degrees as one of four key determinants of stone-free status after flexible ureteroscopy [13]. More recently, Tufano et al. demonstrated in a large retrospective analysis of 800 adult procedures that IPA and stone volume were the strongest independent predictors of residual fragments, a finding that mirrors our own regression output [14]. However, the magnitude of the IPA effect in our pediatric cohort (OR=6.72) exceeded the values typically reported in adults, possibly because the smaller calyceal dimensions and the relatively larger endoscope-to-calyx ratio in children further limit instrument maneuverability when the angle is acute [3,15,22].The observation that stone density above 1000 HU independently predicted failure (OR=3.28) has a straightforward physical explanation: harder stones absorb laser energy less efficiently and require extended dusting time, which in turn increases the volume of residual debris and the likelihood that some fragments will remain trapped in dependent calyces [16,19]. This finding aligns with earlier reports in adult practice but has not, to our knowledge, been specifically demonstrated in a pediatric cohort before the present study.A particularly noteworthy result was the absence of a significant independent effect for stone multiplicity (OR=1.42, p=0.485). This is reassuring because it suggests that modern flexible ureteroscopes possess sufficient maneuverability to address multiple calculi within a single session, provided the anatomy is otherwise favorable – a point previously implied by Gatti et al. in their experience with dedicated pediatric instruments [4]. From a practical standpoint, this means that the mere presence of more than one stone should not automatically disqualify a child from RIRS.When set against existing predictive tools, the P-RPS appears to offer a meaningful improvement in discriminatory accuracy within the pediatric setting. The RUSS, validated externally by Sfoungaristos et al. in an adult series, achieved an AUC of 0.707 [17], while Selmi et al. reported AUC values between 0.725 and 0.755 for four different scoring systems applied to adult RIRS outcomes [7]. Tufano et al. found an AUC of 0.735 for Ito's nomogram, the best-performing tool in their 800-patient comparison [14]. Even the R.I.R.S. scoring system, which achieved an AUC of 0.868 in one recent prospective study [18], falls short of the 0.895 observed for P-RPS. While these comparisons must be interpreted cautiously given the different populations and study designs involved, they suggest that a pediatric-tailored instrument incorporating age-relevant anatomical variables may outperform generic adult tools when applied to children.The clinical translation of the P-RPS into a traffic-light algorithm provides surgeons with an actionable decision framework. The green zone (0-1 points) identifies children for whom RIRS is expected to succeed in over 94% of cases – making percutaneous access unnecessary and its attendant risks of parenchymal injury, bleeding, and radiation unjustified [2,10]. The red zone (4-5 points) identifies children in whom an RIRS attempt carries a nearly sevenfold risk of failure and where mini-PCNL, with its reported stone-free rates exceeding 92% in similar patients, represents the more rational first-line choice [3,11]. Perhaps most valuable is the yellow zone (2-3 points), which explicitly acknowledges clinical uncertainty and invites shared decision-making – a concept increasingly recognized as integral to patient-centered surgical care [16].Several limitations warrant mention. Our cohort, while prospectively enrolled, included only 54 RIRS patients, limiting the statistical power for subgroup analyses and precluding a formal split-sample internal validation. The P-RPS has not yet been tested in an independent external cohort, and its generalizability beyond the two participating centers remains to be confirmed. Additionally, the scoring system does not account for operator experience, which may influence outcomes independently of anatomical factors.
5. Conclusions
- Multivariate logistic regression analysis identified three independent predictors of RIRS failure in children: an infundibulopelvic angle below 45 degrees (OR=6.72), stone size exceeding 20 mm (OR=4.15), and stone density above 1000 HU (OR=3.28). Based on these findings, the P-RPS scoring system was developed and demonstrated high predictive accuracy (AUC=0.895, sensitivity 88.4%, specificity 91.2%). The derived traffic-light treatment algorithm stratifies patients into low-, intermediate-, and high-risk groups, enabling personalized surgical planning. Children scoring 0-1 points are optimal candidates for RIRS, those with 4-5 points should be directed toward mini-PCNL, and the intermediate group requires individualized assessment. Multicenter external validation of the P-RPS is warranted to confirm its generalizability and clinical utility.