Fattakhova Yu. E.
Tashkent State Medical University, Tashkent, Uzbekistan
Correspondence to: Fattakhova Yu. E., Tashkent State Medical University, Tashkent, Uzbekistan.
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
The purpose of the study was to determine the prognostic significance of the level of micronutrients and markers of systemic inflammation in the worsening of the clinical course of chronic obstructive pulmonary disease (COPD) associated with anxiety and depressive disorders. Materials and methods. We examined 100 patients with COPD aged 38-82 years who were treated in the pulmonology department of the Republican Scientific and Practical Medical Center and 30 practically healthy controls, matched by age and gender. Clinical and functional assessment, spirometry, determination of the severity of shortness of breath according to the mMRC scale, the impact of the disease on daily life according to CAT, psychometric evaluation according to the HADS and CES-D scales, as well as laboratory determination of C-reactive protein, fibrinogen, vitamin D, magnesium and zinc were carried out. To assess the prognostic significance, logistic regression analysis was used to calculate the odds ratio (OR) and 95% confidence intervals. Results. Anxiety-depressive syndrome was detected in 78.0% of patients. COPD patients with anxiety and depressive disorders were characterized by a more severe course of the disease: lower FEV1 (35.1 1.5% vs. 55.9 5.6%; p 20 mg l (OR 4.4; 95% CI 1.8-10.8; p 0.001) and decreased 25(OH)D levels 30 ng ml (OR 3, 8; 95% CI 1, 6-9, 0; p 0, 003).
Keywords:
COPD, Anxiety and depressive disorders, Micronutrients, Vitamin D, Magnesium, Zinc, Systemic inflammation, Forecast
Cite this paper: Fattakhova Yu. E., Prognostic Significance of Micronutrients and Markers of Systemic Inflammation in the Aggravation of the Clinical Course of Chronic Obstructive Pulmonary Disease Associated with Anxiety and Depressive Disorders, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2488-2494. doi: 10.5923/j.ajmms.20261605.48.
1. Introduction
Chronic obstructive pulmonary disease is among the most significant chronic non-communicable diseases and maintains a stable position among the leading causes of disability, reduced quality of life, and premature mortality in the adult population [1,2,5,9,14]. The modern understanding of COPD extends beyond solely a bronchopulmonary process: the disease is viewed as a systemic pathology with a multifactorial pathogenesis, in which chronic inflammation, oxidative stress, immune dysregulation, and various comorbid conditions play an important role [2,3,5,9]. This is precisely why assessing the clinical course of COPD is currently impossible without analyzing extrapulmonary manifestations that can modify the disease's prognosis.One of the most clinically significant comorbid conditions in COPD is anxiety-depressive disorders. Their prevalence in this category of patients, according to various authors, remains high and can reach 30-60%, and in certain clinical samples, even higher values [4,6,12,15]. Anxiety and depression are not limited to a worsening of psycho-emotional well-being: they are associated with an increased subjective perception of dyspnea, reduced adherence to basic therapy, decreased exercise tolerance, and an increased frequency of exacerbations and re-hospitalizations [1,4,6,15]. Thus, psycho-emotional comorbidity can be considered one of the factors that exacerbate the course of COPD and influence its clinical phenotype.The pathogenetic link between COPD and anxiety-depressive disorders is largely mediated by chronic systemic inflammation. Elevated levels of C-reactive protein and fibrinogen are considered a laboratory reflection of inflammatory process activity and an unfavorable prognosis in COPD [3,10,13]. Concurrently, data have accumulated regarding the role of inflammation in the development and maintenance of depressive symptomatology, including neuroinflammatory changes, hypothalamic-pituitary-adrenal axis dysregulation, and neurotransmitter imbalance [7,10,13]. In this regard, the assessment of inflammatory markers in patients with COPD and anxiety-depressive symptoms is of not only diagnostic but also prognostic interest.No less important is the study of micronutrient status. Vitamin D, magnesium, and zinc are involved in immune regulation, antioxidant defense, maintenance of muscle function, and central nervous system functioning [7,8,10,11]. Vitamin D deficiency is associated with more pronounced inflammation, impaired lung function, and an increased risk of unfavorable COPD progression [7,8,10]. Magnesium and zinc insufficiency are considered factors that disrupt neurotransmitter and metabolic processes, contributing to the exacerbation of both respiratory symptoms and psycho-emotional disorders [8,11]. Therefore, a combined assessment of inflammatory biomarkers and micronutrients can provide a more comprehensive understanding of the mechanisms that worsen COPD associated with anxiety-depressive disorders.Despite the existence of individual studies focusing on the role of inflammation, vitamin D deficiency, or psycho-emotional disorders in COPD, a comprehensive assessment of their prognostic significance within a unified clinical-laboratory approach remains underdeveloped [1,3,7,8,10,11]. The search for markers that would allow for the early identification of patients at high risk of unfavorable clinical progression and, consequently, justify a more personalized management strategy is particularly relevant. This has determined the direction of the present study.Purpose of the studyTo determine the prognostic significance of the level of micronutrients and markers of systemic inflammation in the worsening of the clinical course of chronic obstructive pulmonary disease associated with anxiety and depressive disorders.
2. Materials and Methods
The study was carried out on the basis of the Department of Pulmonology of the Republican Scientific and Practical Medical Center. The study included 100 patients with a verified diagnosis of COPD, aged 38 to 82 years, who were hospitalized. Diagnosis was based on GOLD (2020) criteria 9. The control group for laboratory comparison consisted of 30 practically healthy individuals matched by age and gender.Inclusion criteria were a verified diagnosis of COPD, voluntary informed consent to participate in the study, and the patient’s ability to adequately assess his condition. Exclusion criteria included refusal to participate, severe comorbidity, history of mental illness, alcoholism or drug abuse, or other conditions that would prevent compliance with the study procedure.All patients underwent clinical and anamnestic assessment, spirometry with determination of FEV1, assessment of the degree of dyspnea using the mMRC scale and symptom load using the CAT questionnaire. Psychoemotional status was studied using the HADS hospital anxiety and depression scale and the CES-D scale. The laboratory block included determination of the levels of C-reactive protein, fibrinogen, 25(OH)D, magnesium and zinc.Statistical processing was carried out using generally accepted methods of variation statistics. Quantitative data are presented as mean and standard deviation or median and interquartile range, depending on the nature of the distribution. Between-group differences were assessed using Student's t test; qualitative characteristics were presented in the form of absolute and relative values. To analyze the prognostic significance of laboratory parameters, logistic regression was used to calculate odds ratios and 95% confidence intervals. Differences were considered statistically significant at p 0.05.
3. Results
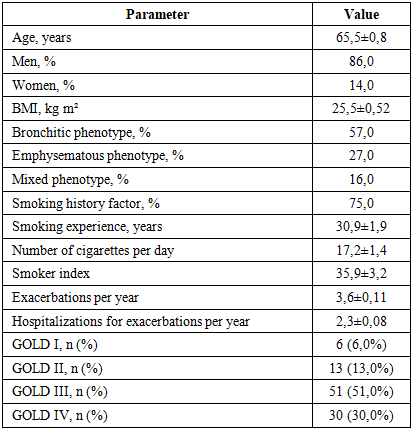
Clinical and demographic characteristics of the examined cohort are presented in Table 1. The presented data show that the study included a predominantly elderly population of patients with COPD with a high proportion of men, a significant tobacco load and a predominance of severe stages of the disease. Already at the initial stage, attention is drawn to the high frequency of exacerbations and hospitalizations, which reflects the clinical severity of the observed sample.Table 1. Initial clinical and demographic characteristics of patients with COPD
 |
| |
|
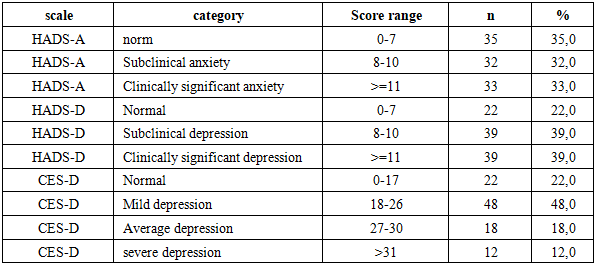
The next step was to assess the prevalence of anxiety and depressive symptoms. As can be seen from Table 2 and Figure 1, signs of anxiety and depression of varying severity were found in the majority of the patients examined. Particularly indicative is the high proportion of subclinical and clinically pronounced disorders, which emphasizes the need for systematic psychometric screening in routine monitoring of patients with COPD.Table 2. Distribution of anxiety and depressive symptoms in patients with COPD
 |
| |
|
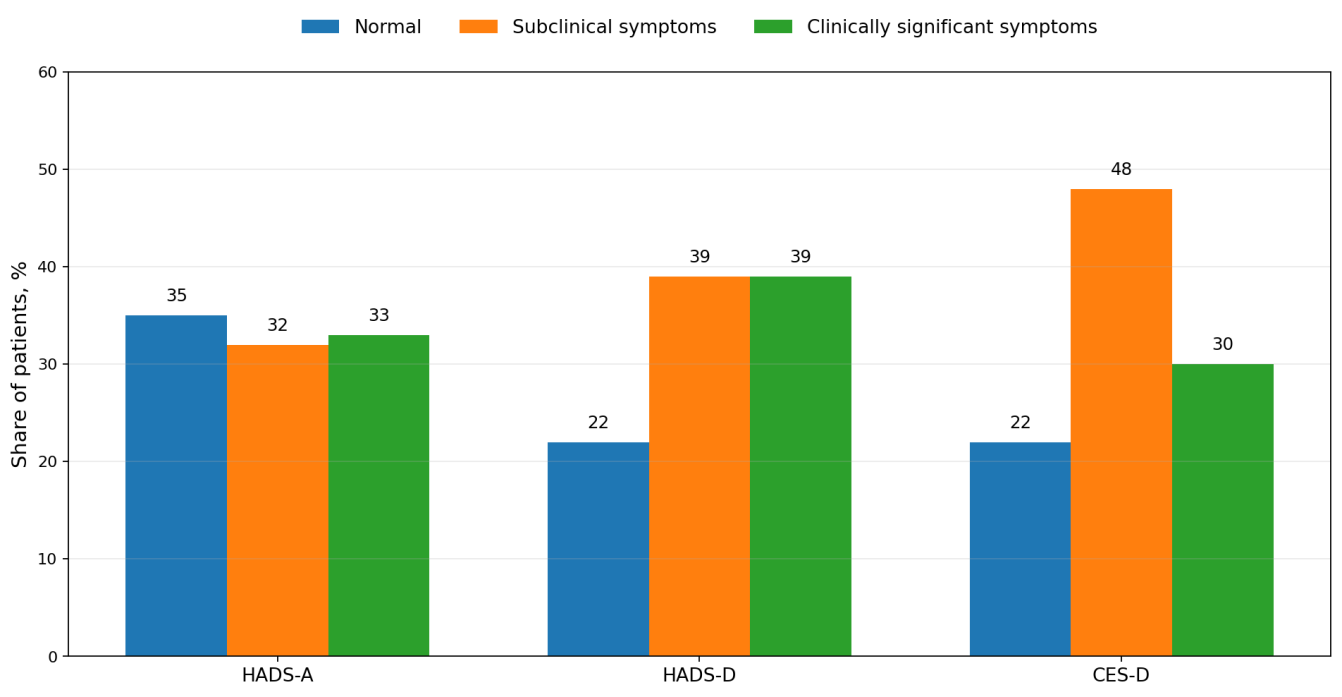 | Figure 1. Distribution of anxiety-depressive symptoms according to the HADS and CES-D scales |
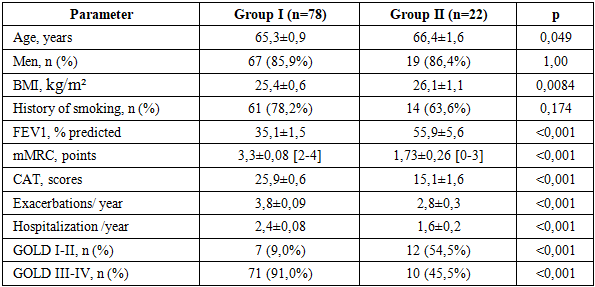
Based on the results of HADS and CES-D, patients were divided into two subgroups: group I - patients with anxiety-depressive syndrome, group II - patients without it. The proportion of patients with clinically significant psycho-emotional disorders was 78.0%, which further emphasizes the high frequency of comorbid mental symptoms in the inpatient cohort of COPD patients.Table 3. Distribution of patients depending on the presence of anxiety-depressive syndrome
 |
| |
|
A comparative analysis of clinical and functional parameters showed that the presence of anxiety-depressive syndrome is associated with a more severe course of COPD (Table 4). Despite the comparability of the groups by gender, smoking and a number of baseline characteristics, patients in group I had a lower FEV1, higher mMRC and CAT values, as well as a greater number of exacerbations and hospitalizations. A smooth transition from demographic comparison to functional differences allows us to consider the identified changes as clinically significant and not random.Table 4. Clinical and functional differences between groups of patients with COPD
 |
| |
|
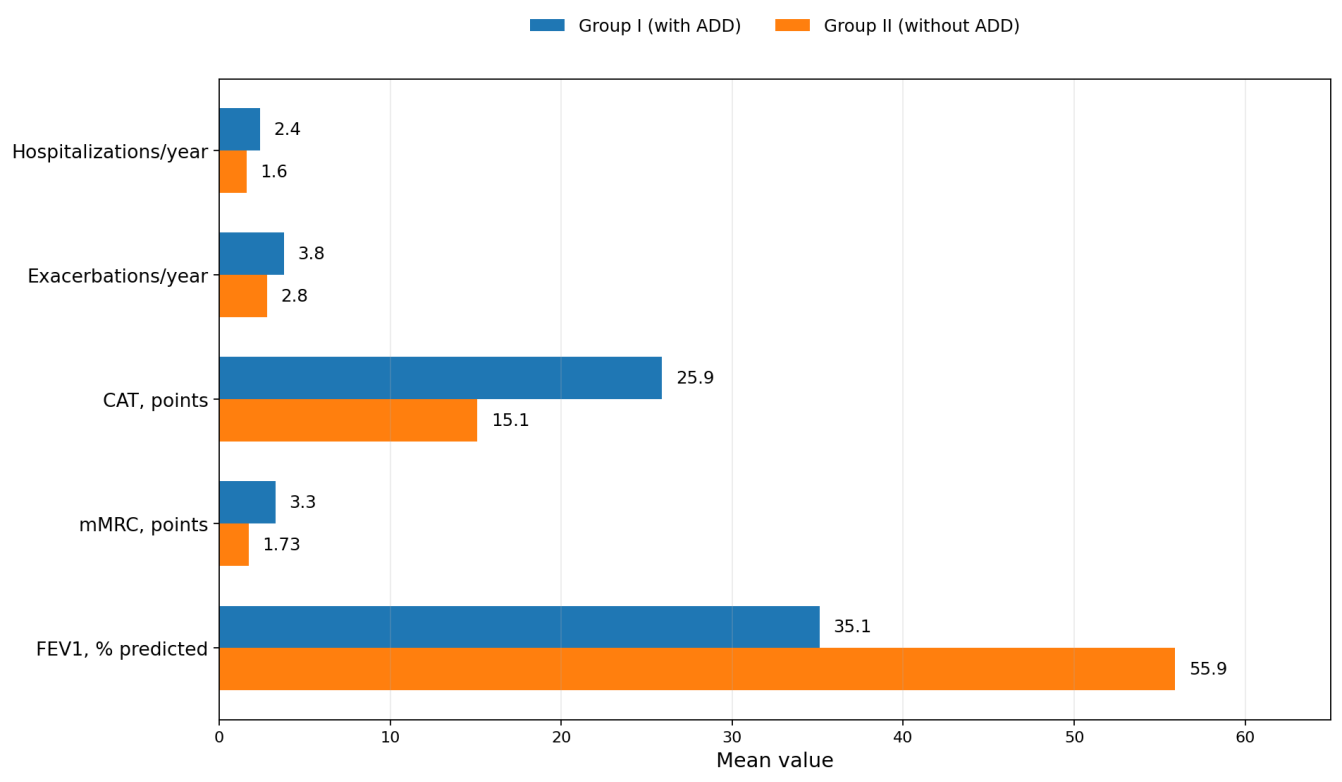 | Figure 2. Clinical and functional indicators in groups of patients with COPD depending on the presence of anxiety-depressive syndrome |
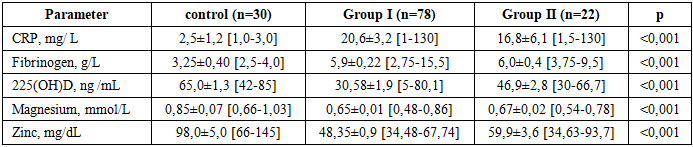
The laboratory block of the study made it possible to supplement clinical observations with objective biochemical data (Table 5). Compared with controls, patients with COPD had higher levels of CRP and fibrinogen, as well as lower values of vitamin D, magnesium and zinc. The most unfavorable profile was found in group I, which is consistent with a more severe clinical course of the disease and a greater severity of psycho-emotional disorders.Table 5. Markers of systemic inflammation and micronutrient status
 |
| |
|
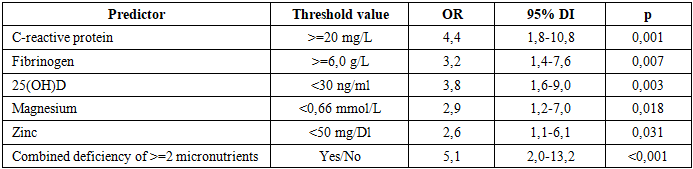
Logistic regression analysis was performed to assess the prognostic significance of laboratory parameters. The results of Table 6 and Figure 3 show that the greatest strength of association with severe COPD associated with anxiety and depressive disorders was a combined deficiency of two or more micronutrients, an increase in CRP and a decrease in vitamin D levels. The inclusion of confidence intervals allows us to judge not only the magnitude of the effect, but also its stability.Table 6. Logistic regression: laboratory predictors of unfavorable course of COPD
 |
| |
|
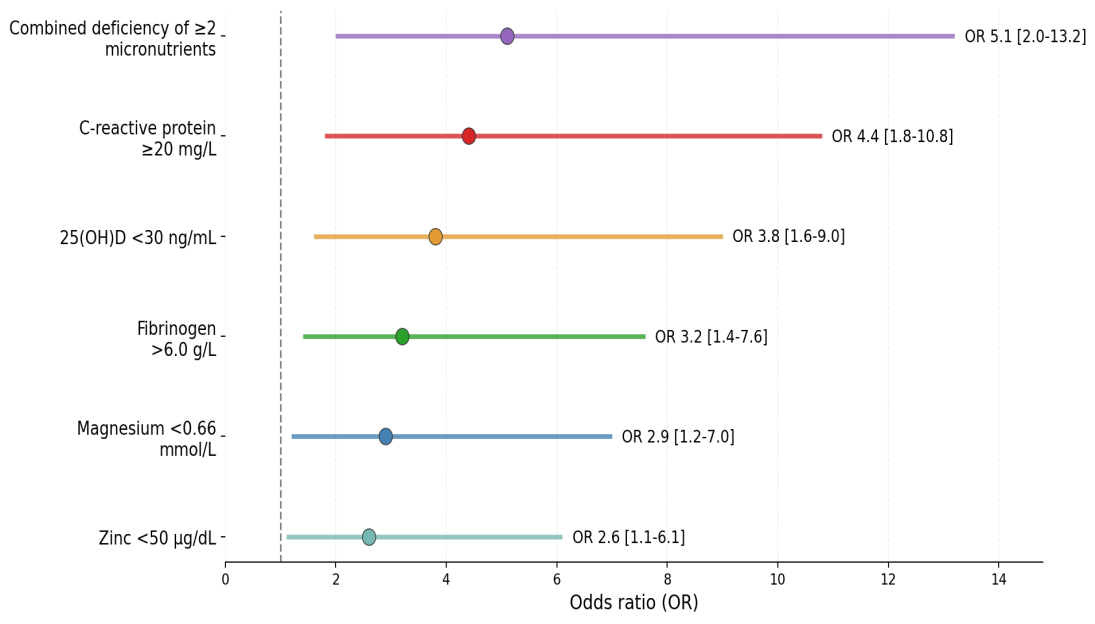 | Figure 3. Odds ratios for laboratory predictors of unfavorable COPD |
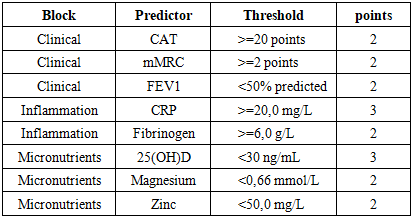
From a practical point of view, the totality of identified clinical and laboratory patterns makes it possible to present the results in the form of a structured risk stratification scale. Table 7 consistently shows the main components of the final assessment, including parameters of symptom load, frequency of exacerbations, indicators of external respiratory function, the presence of anxiety and depressive disorders, markers of systemic inflammation and signs of micronutrient deficiency. This representation facilitates the integral interpretation of the data obtained and makes their step-by-step clinical assessment possible.Table 7. Components of the prognostic risk score
 |
| |
|
The scale presented in Table 7 combines the most significant indicators that in the present study were associated with a more severe course of the disease. Moreover, the structure of the scale makes it possible to take into account not one isolated parameter, but the combined influence of clinical symptoms, inflammatory activity and micronutrient disorders. This approach makes the final score more clinically applicable because it reflects the multicomponent nature of COPD progression. The next step is the interpretation of the total score, which allows you to assign the patient to a certain risk category and select the appropriate monitoring tactics. These data are shown in Table 8.Table 8. Risk categories by total points
 |
| |
|
4. Discussion
The results obtained confirm that anxiety and depressive disorders occupy a significant place in the structure of comorbidity in COPD and are associated with a more severe clinical phenotype of the disease. In the present study, anxiety-depressive syndrome was detected in 78.0% of patients, which exceeds the average figures given in the literature for the general population of COPD patients, but corresponds to data from clinical samples with a predominance of patients with moderate and severe disease [4,6,15] This frequency probably reflects the combined influence of a pronounced symptom burden, a long course of the disease and a high frequency of exacerbations.Particularly noteworthy is the fact that the presence of anxiety-depressive syndrome was accompanied not only by changes in psychometric indicators, but also by a significant deterioration of key clinical and functional parameters. In patients of group I, FEV1 was significantly lower, and mMRC and CAT scores were significantly higher than in patients without anxiety-depressive syndrome. This is consistent with the idea of a two-way relationship between the severity of bronchial obstruction, the severity of symptoms and psycho-emotional maladjustment: the more severe the respiratory restrictions, the higher the risk of anxiety and depression, and psycho-emotional disorders, in turn, increase the subjective perception of shortness of breath and reduce the patient’s adaptive capabilities [1,4,6,12,15].The increased frequency of exacerbations and hospitalizations in patients with anxiety-depressive syndrome is of particular clinical interest. Repeated exacerbations reflect not only greater biological activity of the disease, but also a higher risk of functional decline in the long term. The differences observed in our work indicate that psychoemotional comorbidity is associated with a more unfavorable course of COPD and can be used as an additional marker of clinical instability. This finding is consistent with the literature that anxiety and depression are associated with lower treatment adherence, poorer disease self-management, and more frequent health care utilization [1,4,6,15].The laboratory block of research complements the clinical picture. Patients with COPD showed pronounced signs of systemic inflammation, and the most unfavorable profile was observed in the group with anxiety and depressive disorders. A significant increase in the levels of CRP and fibrinogen is consistent with modern ideas about chronic systemic inflammation as one of the universal pathogenetic mechanisms of COPD progression [3,10,13] The presence of higher values of inflammatory markers in patients with psychoemotional disorders further indicates the likely commonality of inflammatory and neuropsychiatric mechanisms [7,10,13].No less revealing was the assessment of micronutrient status. In the study cohort, a significant decrease in the levels of vitamin D, magnesium and zinc was found, and the most pronounced deficiency was characteristic of patients with anxiety-depressive syndrome. These data are consistent with the literature on the role of vitamin D in regulating the immune response and muscle function, as well as the importance of magnesium and zinc in maintaining metabolic and neurotransmitter balance [7,8,10,11]. It is important that the differences were not only statistically significant, but also clinically significant, since they were accompanied by a deterioration in functional and symptomatic indicators.The results of logistic regression analysis allow us to move from describing associations to identifying specific prognostically significant features. In the present study, the strongest association with severe COPD associated with anxiety and depressive disorders was demonstrated by a combined deficiency of two or more micronutrients, an increase in CRP and a decrease in vitamin D levels. This result seems natural: a combined micronutrient deficiency reflects a deeper metabolic imbalance, while high levels of CRP characterize active systemic inflammation. The joint assessment of these parameters allows us not to limit ourselves to fixing an already formed serious condition, but to use them for risk stratification.The practical value of the data obtained lies in the fact that they served as the basis for the development of a clinical and laboratory prognosis scale. Unlike an isolated assessment of symptoms or a single biochemical indicator, the proposed approach combines clinical, inflammatory and micronutrient components, that is, it reflects the multicomponent nature of the unfavorable course of COPD. This integrative model is consistent with the current understanding of COPD as a systemic disease and can be used to earlier identify patients who require enhanced monitoring and multidisciplinary management.In general, the results of the study allow us to consider anxiety and depressive disorders, systemic inflammation and micronutrient deficiency as interconnected parts of a single unfavorable course of COPD. This expands the clinical assessment of the patient and confirms the feasibility of an integrated approach, including psychometric screening, monitoring of inflammatory parameters and assessment of nutritional status.
5. Conclusions
1. Anxiety and depressive disorders are widespread in patients with COPD and were detected in 78.0% of patients in the study sample.2. The presence of anxiety-depressive syndrome is associated with a more severe clinical course of the disease: a more pronounced decrease in FEV1, higher mMRC and CAT values, a higher frequency of exacerbations and hospitalizations.3. Patients with COPD, especially those with anxiety and depressive disorders, have higher levels of C-reactive protein and fibrinogen, as well as more pronounced deficiencies of vitamin D, magnesium and zinc.4. The most significant laboratory predictors of an unfavorable course of COPD associated with anxiety and depressive disorders are a combined deficiency of two or more micronutrients, an increase in CRP 20 mg l and a decrease in the level of 25(OH)D 30 ng ml.5. Integration of psychometric, clinical, functional and laboratory indicators allows for risk stratification and justifies a personalized approach to the management of patients with COPD.
References
| [1] | Bolotova E.V., Dudnikova A.V., Trembach V.V. Possibilities for correcting depressive disorders in patients with chronic obstructive pulmonary disease. Almanac of Clinical Medicine. 2020; 48(5): 299-306. doi: 10.18786 2072-0505-2020-48-063. |
| [2] | Budnevsky A.V., Ovsyannikov E.S., Maltseva Yu.S. and others. Features of the course of chronic obstructive pulmonary disease against the background of metabolic syndrome. Science of the Young (Eruditio Juvenium). 2020; 8(2): 164-171. |
| [3] | Klyachkin L.M., Geltser B.I. Systemic inflammation in chronic obstructive pulmonary disease. Therapeutic archive. 2018; 90(3): 5-12. |
| [4] | Kochetova E.V. The severity of depression in patients with chronic obstructive pulmonary disease in combination with hypertension. Medical and pharmaceutical journal Pulse. 2020; 22(9): 36-41. |
| [5] | Chuchalin A.G. Chronic obstructive pulmonary disease: modern approaches to diagnosis and treatment. Pulmonology. 2019; 29(1): 7-20. |
| [6] | Biswas D, Mukherjee S, Chakroborty R, et al. Occurrence of anxiety and depression among stable COPD patients and its impact on functional capability. J Clin Diagnosis Res. 2017; 11(2): OC24-OC27. |
| [7] | Dias CJ, Barroso R, Dias-Filho CAA, et al. Possible influences of vitamin D levels on sleep quality, depression, anxiety and physiological stress in patients with chronic obstructive pulmonary disease: a case-control study. Sleep Sci. 2022; 15(Spec 2): 369-374. |
| [8] | Fu L, Fei J, Tan ZX, et al. Low vitamin D status is associated with inflammation in patients with chronic obstructive pulmonary disease. Journal of Immunology. 2021; 206(3): 515-523. |
| [9] | Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. 2020 report. 2020. |
| [10] | Jiang Y, Li M, Yu Y, et al. Correlation between vitamin D, inflammatory markers and T lymphocytes with the severity of chronic obstructive pulmonary disease and its effect on the risk of acute exacerbation. Clinical Therapeutics. 2025; 47(1): 44-54. |
| [11] | Li M, Zhao L, Hu C, et al. Improvement of lung function by micronutrient supplementation in patients with COPD: a systematic review and meta-analysis. Nutrients. 2024; 16(7): 1028. |
| [12] | Mathew AR, Yount SE, Kalhan R, Hitsman B. Psychological functioning in patients with chronic obstructive pulmonary disease: a preliminary study of relations with smoking status and disease impact. Nicotine Tob Res. 2019; 21(5): 686-690. |
| [13] | Miller AH, Raison CL. The role of inflammation in depression: from evolutionary imperative to modern treatment target. Nat Rev Immunol. 2016; 16: 22-34. |
| [14] | Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease. Am J Respir Crit Care Med. 2019; 195(5): 557-582. |
| [15] | Yohannes AM, Kaplan A, Hanania NA. Anxiety and depression in chronic obstructive pulmonary disease: recognition and management. J Fam Pract. 2018; 67(2 Suppl): S11-S18. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML