Fattakhov R. A.
Tashkent State Medical University, Tashkent, Uzbekistan
Correspondence to: Fattakhov R. A., Tashkent State Medical University, Tashkent, Uzbekistan.
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
The purpose of the study was to evaluate the diagnostic and prognostic significance of metabolic parameters in predicting the development of comorbid conditions in patients with chronic obstructive pulmonary disease (COPD). Materials and methods. The study included 100 patients with COPD aged 38-82 years. Clinical and functional assessment, spirometry, six-minute walk test, analysis of symptoms using the CAT and mMRC scales, as well as determination of carbohydrate, lipid and inflammatory profiles were carried out. To assess the prognostic significance of metabolic markers, logistic regression analysis with calculation of odds ratio (OR) and ROC analysis were used. Results. As COPD worsened, disturbances in carbohydrate and lipid metabolism, as well as the activity of systemic inflammation, increased. Patients with comorbid pathology had more severe dyspnea, a higher total CAT score, and lower FEV₁ and exercise tolerance values. The most significant prognostic predictors of comorbidity were C-reactive protein, HOMA-IR, triglycerides, hypoalbuminemia and hyperfibrinogenemia. The combined HOMA-IR model of TG CRP showed an AUC of 0.89. Conclusion Metabolic predictors have high clinical and prognostic significance in patients with COPD and can be used for early risk stratification of comorbid conditions and personalization of interdisciplinary monitoring.
Keywords:
Chronic obstructive pulmonary disease, Comorbidity, Metabolic predictors, HOMA-IR, C-reactive protein, ROC analysis, Odds ratio
Cite this paper: Fattakhov R. A., Prognostic Significance of Metabolic Predictors in the Development of Comorbidity in Patients Chronic Obstructive Pulmonary Disease, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2481-2487. doi: 10.5923/j.ajmms.20261605.47.
1. Introduction
Chronic obstructive pulmonary disease is one of the most significant chronic respiratory diseases, as it is characterized by high prevalence, progressive course and a significant contribution to the structure of mortality and disability. According to modern concepts, the clinical outcome of COPD is determined not only by the degree of bronchial obstruction, but also by the spectrum of concomitant diseases that worsen exercise tolerance, increase the frequency of hospitalizations and are associated with a more unfavorable long-term prognosis [11].In recent years, COPD has increasingly been viewed as a systemic disease, which is based on low-intensity chronic inflammation, oxidative stress and disorders of metabolic homeostasis. It is the systemic nature of the pathological process that explains the frequent combination of COPD with cardiovascular, endocrine, renal and nutritional disorders [5,13,17]. In this context, Sirtuin 1 (SIRT1) has been discussed as a regulator of metabolic reprogramming, cellular senescence, apoptosis and chronic disease mechanisms, which may be relevant to the systemic manifestations of COPD [3,12,14,15].Comorbidity in COPD is not random, but natural. The works of domestic and foreign authors have shown that a significant proportion of patients develop stable clusters of cardiometabolic, cachectic and inflammatory disorders, which determine the clinical profile of the patient to a greater extent than isolated indicators of external respiratory function [4,7,8,16].From a practical point of view, of particular interest is the search for early metabolic markers that can be used to predict the development of comorbid conditions even before their full clinical manifestation. Increased fasting glycemia, insulin resistance, dyslipidemia, hypoalbuminemia and increased markers of systemic inflammation are already considered as indicators of an unfavorable course of COPD and the risk of multimorbidity [1,9,10,18].Recent studies have emphasized that the integration of metabolic predictors into the clinical algorithm for monitoring patients with COPD corresponds to the modern trend towards personalized medicine. Systematic review and meta-analysis by H. Alrabbaie et al. showed a high prevalence of metabolic syndrome in COPD, while Egerod, Lange and Vestbo demonstrated the clinical relevance of comorbidity profiles for risk stratification [6,7].However, in real practice, a symptom-based model of patient management dominates, and the prognostic potential of metabolic indicators is not sufficiently used. This makes it urgent to clarify the diagnostic and prognostic role of metabolic predictors in patients with COPD and to develop a practice-oriented approach to assessing the risk of comorbidity [11,16,17].Purpose of the studyTo evaluate the diagnostic and prognostic significance of metabolic parameters in predicting the development of comorbid conditions in patients with chronic obstructive pulmonary disease.
2. Materials and Methods
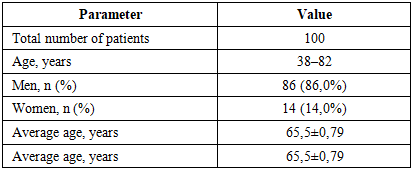
The work is based on data from a comprehensive clinical, functional and laboratory examination of 100 patients with COPD who were under observation in a specialized medical institution. The age of the subjects ranged from 38 to 82 years, the average age was 65.5 0.79 years; men predominated and made up 86.0% of the sample. Main clinical and demographic characteristics are presented in Table 1.Table 1. Clinical and demographic characteristics of the surveyed sample
 |
| |
|
All studies were carried out in compliance with the requirements of the Declaration of Helsinki and regulatory documents of the Ministry of Health of the Republic of Uzbekistan. Inclusion criteria were a verified diagnosis of COPD, voluntary informed consent of the patient and the ability to adequately assess their own condition. Patients with severe comorbidities, mental disorders, and conditions that could limit compliance with the study protocol were excluded from the study.Clinical assessment included analysis of complaints, duration of the disease, smoking history, frequency of exacerbations and hospitalizations, as well as identification of signs of concomitant cardiovascular, endocrine and metabolic pathologies. The severity of symptoms was determined using the CAT and mMRC scales, and exercise tolerance using the six-minute walk test. Pulmonary function testing was performed using spirometry.The laboratory phase included assessment of fasting glucose, insulin, HOMA-IR index, lipid profile, C-reactive protein, fibrinogen, uric acid, albumin and body mass index. Statistical processing was carried out using methods of variation statistics, correlation and logistic regression analysis. The prognostic value of the markers was clarified using ROC analysis with calculation of AUC, sensitivity and specificity.The distribution of patients according to disease stages according to GOLD was uneven: the proportion of patients with stages I and II was 6.0% and 13.0%, respectively, while patients with stages III and IV predominated (51.0% and 30.0%). This indicates the accumulation in the sample of individuals with clinically significant and functionally more severe COPD, which is important to consider when interpreting metabolic and prognostic indicators.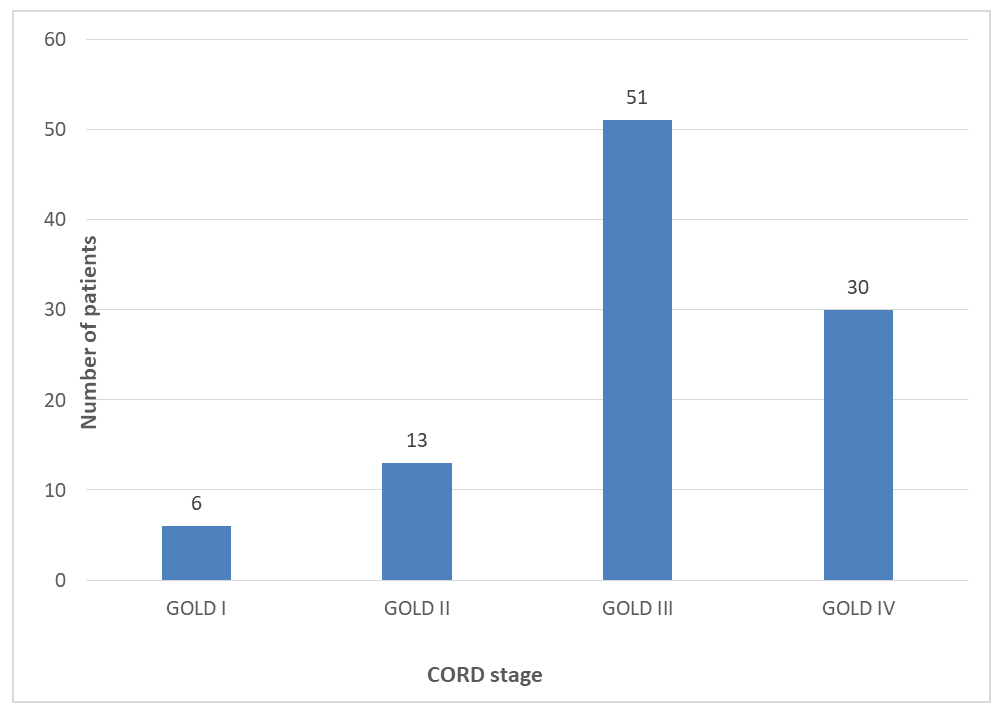 | Figure 1. Distribution of patients by COPD stage |
3. Results
At the first stage, the dynamics of metabolic parameters were assessed depending on the severity of COPD. The data obtained demonstrated that as the disease progresses, an increasingly pronounced complex of disorders of carbohydrate and lipid metabolism is formed, and the activity of systemic inflammation also increases. These changes are presented in Table 2.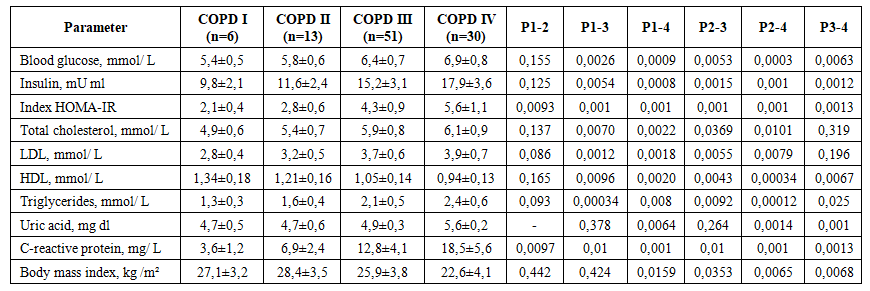 | Table 2. Metabolic parameters in patients with COPD depending on the severity of the disease (M±SD) |
Analysis of Table 2 shows a consistent increase in the levels of glucose, insulin and HOMA-IR index from stage I to stage IV COPD. A similar trend was found for total cholesterol, LDL, triglycerides, uric acid, C-reactive protein and fibrinogen, while HDL concentrations decreased as the disease became more severe. This profile confirms that the progression of COPD is accompanied not only by an increase in respiratory failure, but also by systemic metabolic dysregulation.The next step was to compare the clinical and functional characteristics of patients with and without comorbid pathology. This made it possible to determine to what extent the presence of concomitant diseases is associated with the severity of symptoms, limitation of physical activity and decreased ventilation function of the lungs.As can be seen from Table 3, the presence of comorbid pathology is associated with a more severe clinical course of COPD. In such patients, the median mMRC dyspnea was higher, the total CAT score was higher, and the proportion of GOLD III IV stages reached 86.8%. In addition, in this group there was a significant decrease in FEV₁, which indicates a combination of respiratory and systemic severity of the disease. | Table 3. Clinical and functional indicators in patients with COPD depending on the presence of comorbid pathology |
To clarify the functional consequences of comorbidity, a comparative assessment of the results of the six-minute walk test and blood oxygen saturation indicators before and after exercise was performed. These data are presented in table 4. | Table 4. Indicators of the six-minute walk test in patients with COPD depending on the presence of comorbid pathology |
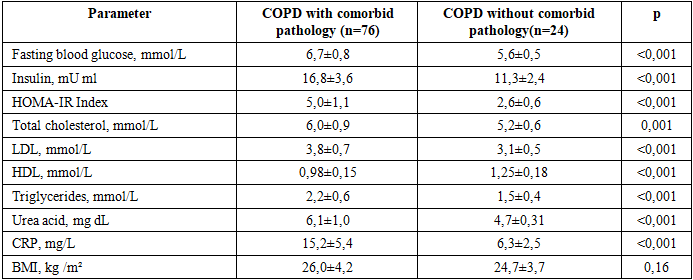
The results obtained demonstrate a lower actual 6MWD distance in patients with comorbid pathology compared to patients without it. Even with similar calculated proper values, differences in the actual distance traveled and the relative percentage of the expected value confirm a decrease in the functional reserve in patients with an unfavorable comorbid profile.Since clinical differences were accompanied by functional limitations, the next step was to compare the metabolic parameters themselves in groups with and without comorbidity. This made it possible to clarify those parameters that most reflect the systemic component of the disease.Table 5 shows that patients with comorbid pathology had higher values of fasting glucose, insulin and HOMA-IR index, as well as more pronounced lipid profile abnormalities and systemic inflammation. The most significant between-group differences concerned HOMA-IR, CRP, triglycerides and uric acid. At the same time, no statistically significant difference was found in BMI, which emphasizes the greater informativeness of biochemical predictors compared to an isolated assessment of body weight.Table 5. Metabolic parameters in patients with COPD depending on the presence of comorbid pathology
 |
| |
|
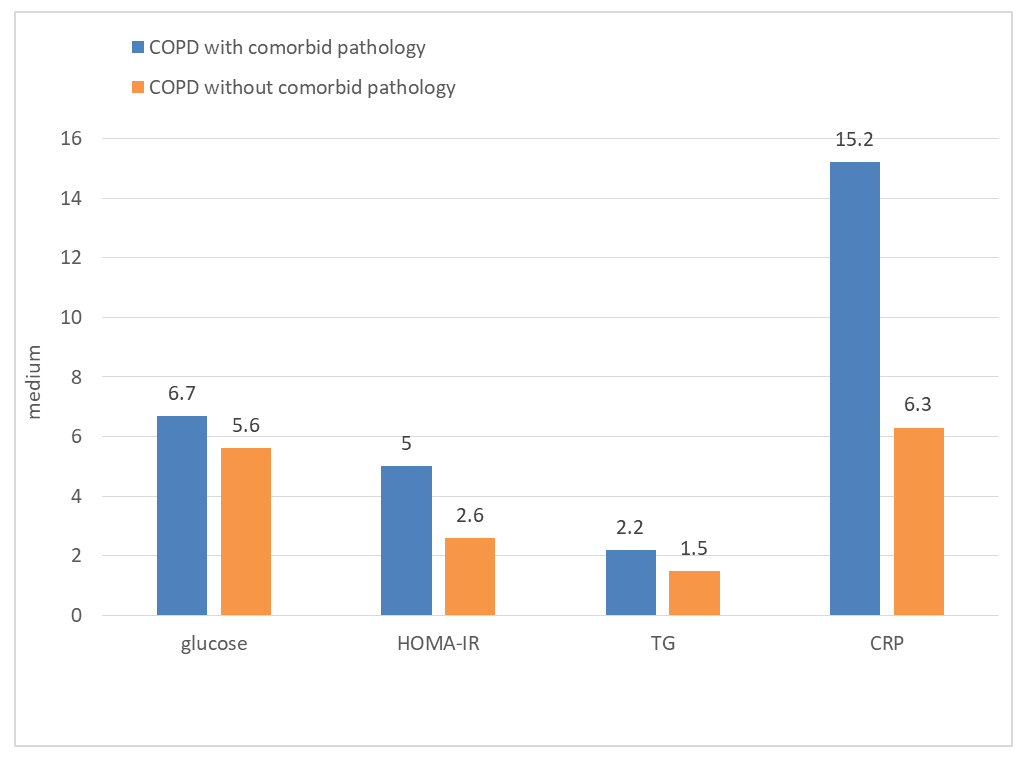 | Figure 2. Comparison of selected metabolic parameters in patients with COPD with and without comorbid pathology |
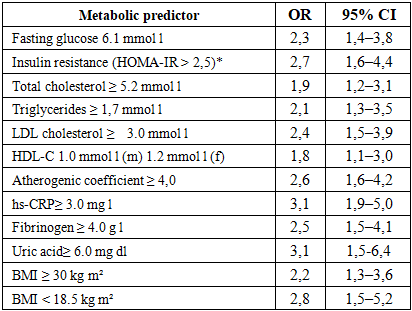
To quantify the contribution of individual metabolic factors to the likelihood of comorbidity, logistic regression analysis was performed to calculate OR and 95% confidence intervals. The results of this stage are presented in Table 6.Table 6. Prognostic significance of individual metabolic predictors of comorbidity development in patients with COPD
 |
| |
|
According to Table 6, the highest contribution to the risk of comorbidity was made by C-reactive protein 10.0 mg l (OR 3.1; 95% CI 1.8 5.2), HOMA-IR 2.5 (OR 2.7; 95% CI 1.6 4.4), albumin 4.0 g l (OR 2.4; 95% CI 1.4 4.0) and fasting hyperglycemia 6.1 mmol l (OR 2.3; 95% CI 1.4 3.8). Consequently, both inflammatory and cardiometabolic markers, reflecting the systemic nature of COPD, are prognostically significant.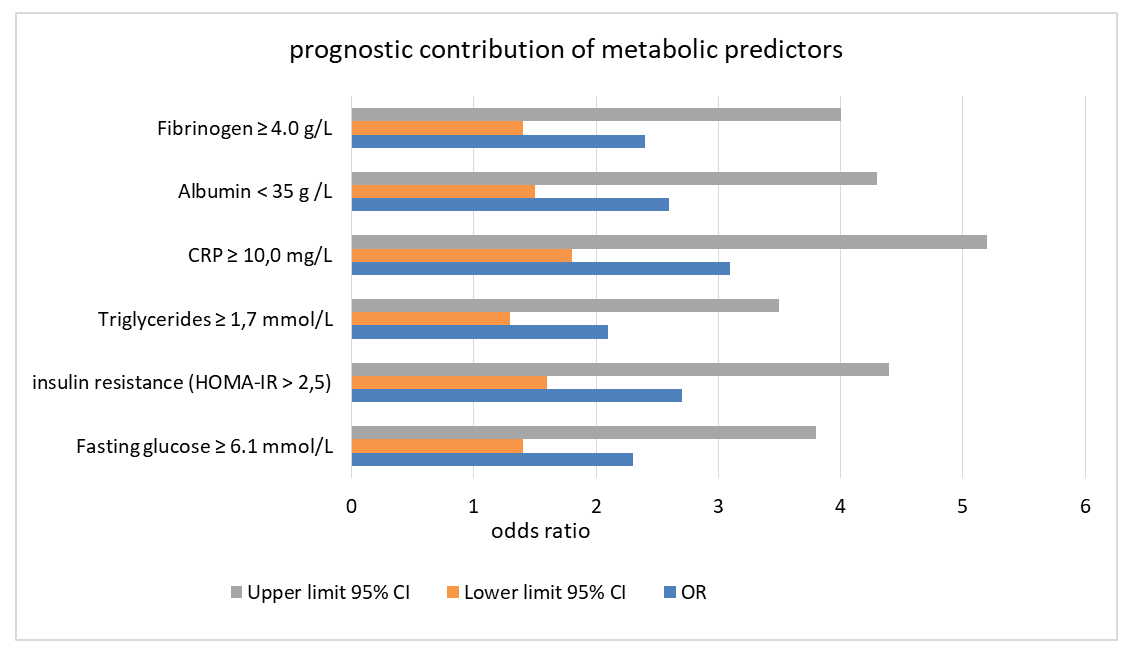 | Figure 3. Contribution of metabolic predictors to the risk of developing comorbidity in patients with COPD |
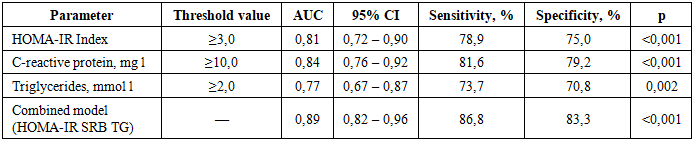
After assessing independent prognostic factors, an ROC assessment of the diagnostic effectiveness of individual indicators and their combinations was carried out. This made it possible to move from describing the strength of association to assessing the practical accuracy of tests in risk stratification.Table 7. Diagnostic accuracy of individual and combined metabolic predictors in predicting comorbidity
 |
| |
|
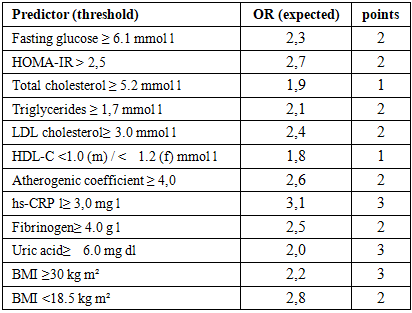
As follows from Table 7, the best diagnostic performance was demonstrated by the combined model that included HOMA-IR, CRP and triglycerides: AUC was 0.89 with a sensitivity of 86.8% and specificity of 83.3%. Among single measures, CRP (AUC 0.84) and HOMA-IR (AUC 0.81) had the greatest accuracy, highlighting the clinical utility of simultaneously assessing inflammatory and metabolic markers.Based on the calculated ORs, a risk stratification scoring scale was formed. Table 8 presents the threshold values of the predictors and the corresponding score, intended for practical use.Table 8. Scoring scale for comorbidity risk stratification in patients with COPD based on metabolic predictors
 |
| |
|
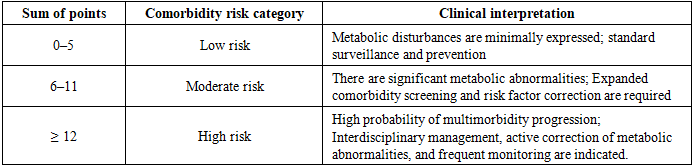
The presented scale integrates the most significant markers into a single system convenient for outpatient and inpatient practice. A higher total score corresponds to a higher likelihood of an unfavorable comorbid profile. A practical interpretation of the total score is presented in Table 9.Table 9. Comorbidity risk categories based on total scores
 |
| |
|
Patients with a score of 0-5 points can be considered a low-risk group, whereas a range of 6-11 points requires extended screening and active risk factor correction. A score of 12 points indicates a high probability of multimorbidity and the need for interdisciplinary observation with more frequent clinical and laboratory monitoring.
4. Discussion
The obtained data confirm that COPD should be considered a systemic disease, in which the progression of respiratory pathology is accompanied by pronounced metabolic restructuring. As the disease progressed from early stages to GOLD III-IV, levels of glucose, insulin, HOMA-IR, total cholesterol, LDL, triglycerides, CRP, and fibrinogen increased. This trend is consistent with the concept of a unified inflammatory-metabolic continuum described in domestic reviews and modern international studies [6,13,16,17].These findings may also be considered in the context of reports highlighting Sirtuin 1 (SIRT1) as a diagnostic and therapeutic target in chronic disease and metabolic dysregulation [3,12,14,15].Of particular importance is the fact that an unfavorable metabolic profile was closely associated not only with the stage of the disease but also with the presence of clinically significant comorbid pathology. Patients with comorbidity exhibited a higher symptom burden, lower FEV1 values, and reduced exercise tolerance. Consequently, metabolic deviations are not a secondary laboratory finding but reflect a systemic component of the disease that influences the functional status of patients [4,5,8,18].From a practical standpoint, the most significant predictors were those combining inflammatory and cardiometabolic components. High OR values for CRP, HOMA-IR, hypoalbuminemia, hyperfibrinogenemia, and fasting hyperglycemia indicate that the risk of comorbidity is increased by both chronic inflammation and disorders of energy and protein metabolism. This conclusion is consistent with data showing that it is the combination of inflammatory and metabolic factors that determines the clinical worsening of COPD and prognostically unfavorable comorbidity profiles [1,2,7,9].The results of the ROC analysis further enhance the clinical significance of the identified associations. The high AUC of the combined HOMA-IR-CRP-TG model suggests that an integrated assessment of multiple markers is more accurate than using any single marker. This confirms the need to transition from isolated interpretation of laboratory parameters to a multifactorial risk stratification model, which aligns with the modern direction of personalized medicine and clinical phenotyping of patients with COPD [6,11].The proposed scoring system is of particular practical value, as it transforms the results of statistical analysis into a tool for clinical decision-making. Unlike descriptive characteristics, the scale allows for the direct identification of patients at low, moderate, and high risk of comorbidity. This approach can be used for in-depth examination as well as for patient referral to specialists such as internists, cardiologists, endocrinologists, and others, depending on the dominant risk profile.Overall, the study results allow for the consideration of metabolic predictors as an important component of the comprehensive assessment of patients with COPD. Their inclusion in the standard monitoring algorithm creates prerequisites for earlier detection of unfavorable systemic profiles, timely prevention of comorbid conditions, and personalization of treatment and preventive tactics. Furthermore, the interpretation of indicators should be performed not in isolation, but in the context of clinical severity, functional status, and the structure of concomitant pathology.
5. Conclusions
In patients with chronic obstructive pulmonary disease, systemic metabolic disorders have been identified, the severity of which increases with increasing severity of the disease and in the presence of comorbid pathology.The most significant predictive markers of comorbidity risk were C-reactive protein, HOMA-IR, triglycerides, hypoalbuminemia and hyperfibrinogenemia.The combined HOMA-IR TG CRP model demonstrated high diagnostic accuracy, and the developed scoring scale allows for practical stratification of comorbidity risk in patients with COPD.The inclusion of metabolic predictors in the algorithm for examining patients with COPD is clinically justified and can help personalize the management and interdisciplinary monitoring of this category of patients.
References
| [1] | Agarwal M., Singh R., Kaur H. Role of blood urea nitrogen and serum albumin ratio in predicting in-hospital mortality of patients with chronic obstructive pulmonary disease Monaldi Archives for Chest Disease. 2022. Vol. 92, 2. |
| [2] | Alrabbaie H, Al-Wardat M, Etoom M, Beauchamp M, Goldstein R, Brooks D. The prevalence of metabolic syndrome in chronic obstructive pulmonary disease: A systematic review and meta-analysis. Chron Respira Dis. 2025 Jan-Dec; 22: 14799731251346194. doi: 10.1177 14799731251346194. |
| [3] | Anti-Aging Genes Improve Appetite Regulation and Reverse Cell Senescence and Apoptosis in Global Populations. Advances in Aging Research, 2016, 5, 9-26. |
| [4] | Budnevsky A.V. Features of the course of chronic obstructive pulmonary disease against the background of metabolic syndrome A.V. Budnevsky, E.S. Ovsyannikov, Yu.S. Maltseva and others. Science of the young (Eruditio Juvenium). 2020. T. 8. 2. pp. 164-171. |
| [5] | Chaulin, A. M. Comorbidity: chronic obstructive pulmonary disease and cardiovascular diseases A. M. Chaulin, Yu. V. Grigorieva, D. V. Duplyakov Practical medicine. 2020. T. 18. 1. pp. 26-31. |
| [6] | Egerod L., Lange P., Vestbo J. Comorbidity profiles in chronic obstructive pulmonary disease European Respiratory Journal Open Research. 2025. Vol. 11, 5. |
| [7] | Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease. 2024. 200 p. |
| [8] | Kinvanlun I. G. Renal dysfunction in comorbid patients with chronic obstructive pulmonary disease: risk factors and bidirectional action of systemic effects I. G. Kinvanlun, I. S. Sabirov, Sh. E. Umurzakov et al. The Scientific Heritage. 2021. 58-2(58). pp. 59-64. |
| [9] | Kozlov, E. V. Features of metabolic syndrome in elderly men with chronic obstructive pulmonary disease E. V. Kozlov, R. A. Yaskevich, K. N. Kochergina Clinical gerontology. 2019. T. 25. 5-6. pp. 24-28. |
| [10] | Makarova E. V. Cardiometabolic syndrome and chronic obstructive pulmonary disease: risk factors and mechanisms of comorbidity (review) E. V. Makarova, G. N. Varvarina, V. A. Vakhlamov and others. Medical almanac. 2020. 4(65). pp. 6-20. |
| [11] | Moaleș E.A., et al. Assessment of metabolic syndrome in patients with chronic obstructive pulmonary disease Diagnostics. 2024. Vol. 14, 21. Art. 2437. |
| [12] | Nutrition Therapy Regulates Caffeine Metabolism with Relevance to NAFLD and Induction of Type 3 Diabetes. J Diabetes Metab Disord. 2017; 4: 019. |
| [13] | Papaporfyriou A. et al. Cardiovascular diseases in COPD: from diagnosis and prevalence to therapy Life. 2023. T. 13. 6. P. 1299. |
| [14] | Single Gene Inactivation with Implications to Diabetes and Multiple Organ Dysfunction Syndrome. J Clin Epigenet. 20167; Vol. 3 No. 3:24. |
| [15] | Sirtuin 1, a Diagnostic Protein Marker and its Relevance to Chronic Disease and Therapeutic Drug Interventions. EC Pharmacology and Toxicology 6.4 (2018): 209-215. |
| [16] | Voronkova O. V. Etiopathogenetic parallels and unresolved issues of the pathogenesis of comorbidity of chronic obstructive pulmonary disease and metabolic syndrome (literature review) O. V. Voronkova, T. V. Saprina, E. B. Bukreeva, A. P. Zima Obesity and metabolism. 2020. T. 17. 3. pp. 292-298. |
| [17] | Wüthrich, K. A. Chronic obstructive pulmonary disease and metabolic syndrome: state of the problem (literature review) K. A. Wüthrich, L. V. Kukol, V. V. Lazik Bulletin of St. Petersburg University. Medicine. 2017. T. 12. 1. pp. 18-30. |
| [18] | Yakovleva O. A. Problems of comorbidity of chronic obstructive pulmonary disease and diabetes Annali d Italia. - 2022. - 28. P. 37-42. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML