Mamatkurbonov Shokirjon Bahodirovich, Madjidova Yakutkhan Nabievna
Tashkent State Medical University, Tashkent, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
Background: Epilepsy is one of the most common chronic diseases of the central nervous system, characterized by a high prevalence, significant rates of disability, and a marked reduction in patients’ quality of life. Despite considerable advances in modern neurology, the influence of climatic and geographic factors, as well as individual anatomical and functional characteristics of the cerebrospinal fluid system on the course of epilepsy, remains insufficiently studied. Objective. To conduct a comprehensive assessment of the clinical-neurological, cognitive, and neuroimaging features of epilepsy in patients living in different climatic and geographic conditions, taking into account the cerebrospinal fluid cranial index. Materials and Methods. The study included 197 patients aged 18 to 70 years diagnosed with epilepsy. Clinical-neurological, neuropsychological (MoCA, MMSE), neurophysiological (EEG) methods were used. Results. It was found that patients living in mountainous regions had a significantly higher frequency of seizures (62.7% vs. 45.3%, p<0.05), more pronounced cognitive impairments, and a reduced quality of life. A decrease in the CSF-CI was associated with a more severe course of the disease and greater cognitive deficits. Conclusion. Climatic and geographic factors, as well as the cerebrospinal fluid cranial index, have a significant impact on the course of epilepsy and should be considered when developing individualized treatment strategies.
Keywords:
Epilepsy, Cerebrospinal fluid cranial index, Cognitive impairment, Climate, Quality of life
Cite this paper: Mamatkurbonov Shokirjon Bahodirovich, Madjidova Yakutkhan Nabievna, Features of the Course of Epilepsy in Residents of Mountain–Desert Regions of the Surkhandarya Region, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2472-2480. doi: 10.5923/j.ajmms.20261605.46.
1. Introduction
Epilepsy is a chronic brain disorder characterized by recurrent epileptic seizures caused by excessive neuronal activity. According to current data, this disease affects up to 1% of the population, which determines its high social significance [1–3].In addition to seizures themselves, epilepsy is associated with a wide range of cognitive and psychoemotional disorders that significantly affect patients’ quality of life [4,5].In recent years, increasing attention has been paid to the study of factors that may modify the course of the disease. Among them, climatic and geographic living conditions occupy a special place, as they may influence the functional state of the central nervous system through hypoxic, temperature, and barometric mechanisms [6].Equally important is the condition of the cerebrospinal fluid system, reflected by the cerebrospinal fluid cranial index. This parameter characterizes the ratio between cerebrospinal fluid spaces and the volume of the skull and may serve as an indicator of the compensatory capacity of the intracranial system [7].Thus, a comprehensive study of these factors is of considerable scientific and practical interest.
2. Materials and Methods
This study was designed as an observational (clinical-analytical) study with elements of comparative analysis. The research was conducted at the neurological departments of the Surkhandarya branch of the Republican Scientific Center for Emergency Medical Care from 2021 to 2023.A total of 197 patients diagnosed with epilepsy, aged between 18 and 70 years, residing in mountainous and desert regions of the Surkhandarya region, were included in the study.Inclusion criteria:• confirmed diagnosis of epilepsy; • age between 18 and 70 years; • residence in the studied climatic and geographical regions; • availability of clinical and instrumental examination data. Exclusion criteria:• severe somatic diseases in the stage of decompensation; • mental disorders that impede communication with the patient; • refusal to participate in the study. The sample was formed using a consecutive sampling method, including all patients who met the inclusion criteria. The sample size was determined by the availability of clinical material and provides sufficient statistical power to detect intergroup differences.Data Collection InstrumentsThe following methods and instruments were used for data collection:• Clinical and anamnestic assessment (collection of complaints, medical history, and life history); • Neurological examination with assessment of focal neurological symptoms; • Neuropsychological scales: - MMSE (Mini-Mental State Examination) for cognitive function assessment (range: 0–30 points); - QOLIE (Quality of Life in Epilepsy Inventory) for assessing quality of life in patients with epilepsy; • Neurophysiological examination: electroencephalography (EEG). The applied scales are validated and widely used in clinical practice, ensuring the reliability and reproducibility of the obtained data.Study ProcedurePatients were recruited during their visits to inpatient and outpatient departments.All participants underwent a standard comprehensive examination, including:• clinical and neurological assessment; • neuropsychological testing; • instrumental methods (EEG, MRI/CT). Questionnaires and testing were conducted individually for each patient in a clinical setting. The collected data were recorded in standardized forms and subsequently entered into an electronic database for further analysis.Ethical ConsiderationsThe study was conducted in accordance with the principles of the Declaration of Helsinki.All participants were informed about the aims and methods of the study and provided written informed consent to participate.Full confidentiality and anonymity of personal data were ensured.Data AnalysisStatistical analysis was performed using software such as SPSS, Statistica, or Microsoft Excel (to be specified if necessary). The following methods were applied:• descriptive statistics (mean values, standard deviation); • comparative analysis (Student’s t-test, chi-square (χ²) test); • correlation analysis (where applicable). The choice of statistical methods was determined by the data distribution and study objectives. Differences were considered statistically significant at p < 0.05.
3. Results
Prospectively, the medical records of 197 patients with epileptic seizures were analyzed. The diagnosis was established based on a typical clinical presentation, medical history, and laboratory and instrumental methods of examination. The gender distribution of the examined patients included 121 males and 76 females, and the mean age of the participants was 45.9±6.8 years (Table 1).Table 1. Distribution of Patients by Region of Residence
 |
| |
|
We classified the groups according to the International League Against Epilepsy (ILAE) classification (2001), dividing them by disease type into symptomatic, idiopathic, and cryptogenic forms of epilepsy. The results are presented in Table 2.Table 2. Distribution of Patients with Epilepsy by Type According to Climatic Conditions of Residence
 |
| |
|
Among all examined patients (197 individuals), symptomatic epilepsy was observed in 169 patients (85.8%). The mean age of patients in this group was 42.5±1.1 years. The following probable etiological factors of symptomatic epilepsy (SE) were identified: traumatic brain injury (74; 43.8%), cerebrovascular disorders (70; 41.42%), and neuroinfections (25; 14.8%), the results of which are presented in Figure 1.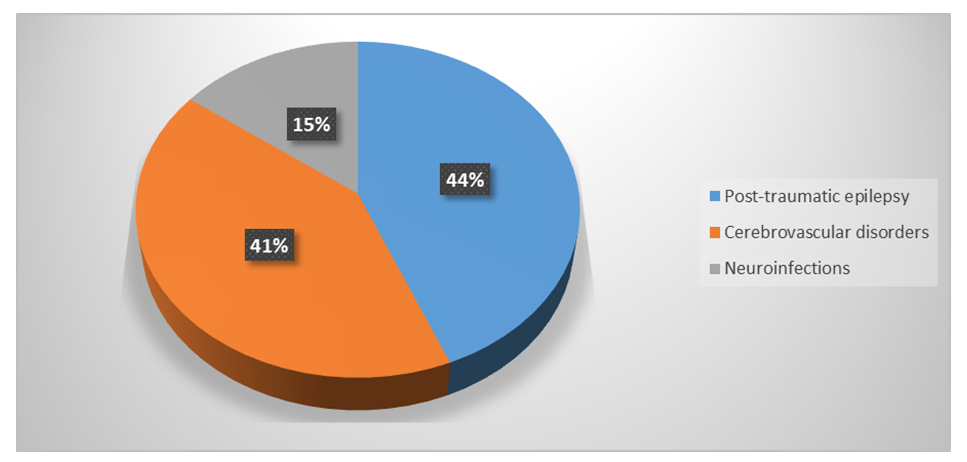 | Figure 1. Etiological factors of symptomatic epilepsy (%) |
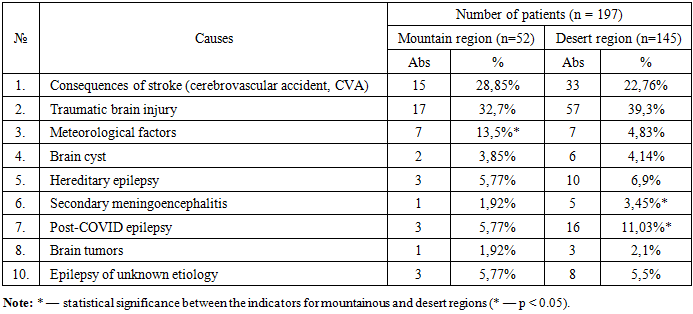
As follows from the data in Table 3, in patients living in different climatic conditions of the Surkhandarya region, certain differences were revealed in the structure of etiological factors of epilepsy.Table 3. Etiology of epilepsy in the studied patients depending on climatic conditions of residence
 |
| |
|
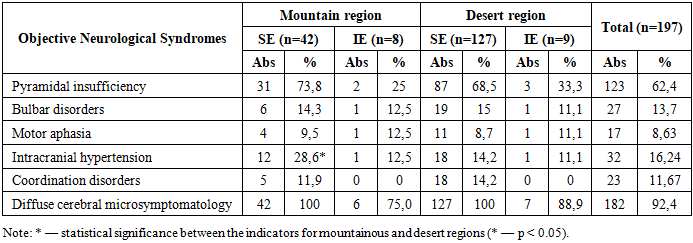
Thus, in patients from mountainous regions, epilepsy developed in 28.85% of cases (15 patients) following a previous acute cerebrovascular accident, whereas in patients from desert areas this indicator was 22.76% (33 patients), which is 1.3 times lower.Traumatic brain injury as an etiological factor was identified in 32.7% of patients from mountainous regions (7 patients) and in 39.3% of patients from desert areas (57 patients). The development of epilepsy against the background of brain cysts was observed in 3.85% of cases (2 patients) among residents of mountainous regions and in 4.14% of cases (6 patients) among patients from desert areas.Particular attention should be paid to the meteorological factor, which was recorded significantly more often in patients from mountainous regions—in 13.5% of cases (7 patients), whereas in desert areas it was observed only in 4.83% of patients (7 patients), which is almost 3 times less. This indicates a more pronounced influence of climatic and atmospheric conditions of mountainous regions on the development of epilepsy.Hereditary predisposition was identified in 5.77% of patients from mountainous regions (3 patients) and in 6.9% of patients from desert areas (10 patients), with no statistically significant differences between the groups.It is also important to note the role of neuroinfections, in particular the post-COVID condition, in the development of epilepsy. In patients who had experienced COVID-19 (19 individuals, 9.6%), there was a tendency toward increased seizure frequency, greater severity, as well as more pronounced cognitive impairments, asthenic manifestations, and symptoms of depression.Epilepsy of unknown origin was diagnosed in 5.77% of patients from mountainous regions (3 patients) and in 5.5% of patients from desert areas (8 patients), with no significant differences.Thus, the obtained data indicate a significant role of climatic factors in the development and course of epilepsy. In patients from mountainous regions, the disease more often developed following stroke and was much more frequently associated with meteorological factors, confirming the more adverse influence of high-altitude conditions.On objective examination, patients showed subclinical signs of a reflex hemic syndrome without pathological reflexes, mild oral automatism signs, Chvostek’s sign, increased deep tendon reflexes, and muscle hypotonia.Neurological examination revealed diffuse cerebral microsymptomatology in all patients (100%), regardless of the region of residence. However, intracranial hypertension syndrome was significantly more common in patients from mountainous regions—28.6% of cases—whereas in desert areas it was observed in 14.2% of cases (p < 0.05), which is twice less frequent.Pyramidal insufficiency was noted in 73.8% of patients with symptomatic epilepsy (SE) from mountainous regions and in 68.5% of patients with SE from desert regions. Bulbar disorders were observed in 14.3% of patients with SE from mountainous regions and 15% of patients with SE from desert regions. Signs of motor aphasia and coordination disorders in patients with SE accounted for 9.5% and 8.7%, respectively, for mountainous and desert regions, with no statistical significance. In patients with idiopathic epilepsy (IE), mild diffuse microsymptomatology was characteristic, observed in 75.0% of patients living in mountainous regions and 88.9% of patients in desert regions (Table 4).Table 4. Frequency of Occurrence of Objective Neurological Symptoms in Patients with Symptomatic and Idiopathic Epilepsy Living in Mountainous and Desert Regions
 |
| |
|
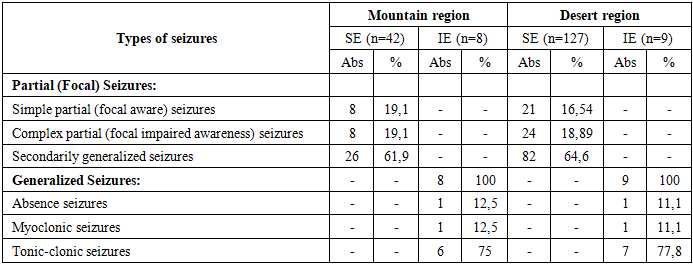
As follows from Table 4, in idiopathic epilepsy (IE), pyramidal insufficiency was recorded significantly less frequently (73.8% vs. 25% in patients from mountainous regions; 87% vs. 33.3% in patients from desert regions; p < 0.01), intracranial hypertension (12.5% vs. 28.6% in patients from mountainous regions; 11.1% vs. 14.2% in desert regions; p < 0.05), and coordination disorders (0% vs. 11.9% in patients from mountainous regions; 0% vs. 14.2% in desert regions; p < 0.01).It is worth noting that among patients with epilepsy, the most frequently observed syndrome was diffuse cerebral microsymptomatology, which was detected in 92.4% of all examined patients. It manifested as mild oculomotor disturbances, smoothing of the nasolabial fold, and occasionally oral automatism reflexes. In patients with symptomatic epilepsy (SE), these manifestations were observed in 100% of cases, while in IE they were seen in 82.5%, which is almost 20% lower, although these differences were not statistically significant.Coordination disorders mainly manifested as intention tremor and mild ataxia, indicating cerebellar insufficiency in 11.67% of patients, with a predominance among those with SE.Pyramidal insufficiency was detected in 62.4% of patients, manifested by decreased limb strength, increased tendon reflexes, and pathological reflexes. In SE, this percentage was higher by 47.8% in mountainous regions and by 35.2% in desert regions.At the time of hospital admission, patients with epilepsy reported the following complaints: loss of consciousness (57.0%), head and dental injuries (24.7%), headache (89.4%), dizziness (16.3%), and memory impairment (63.1%). All patients exhibited emotional lability (64%), aggressiveness (20%), and depression (9%). In older patients, chronic psychoses with episodes of exacerbation were noted (20%). In all cases, intellectual-mnestic impairments were observed (constructive apraxia, reduced concentration of voluntary attention, and speech disorders); these impairments were identified after the onset of seizures.Careful history-taking revealed that even before the manifestation of the first seizures, 76% of patients had emotional lability, which worsened with the onset of the disease.In studying the clinical manifestations of the disease, it was found that the main type of epileptic paroxysms in patients with SE were secondarily generalized seizures, which occurred in 61.9% of examined patients from mountainous regions and 64.6% of patients from desert areas (p < 0.05) (Table 5).Table 5. Distribution of the Examined Patients According to Types of Seizures
 |
| |
|
At the same time, in 38.1% of patients living in mountainous areas and 35.4% of those living in desert regions, seizures did not have a clinical partial component. This fact confirms the need for differential diagnosis with primary generalized tonic-clonic seizures, which are characteristic of patients with idiopathic epilepsy.In SE, various types of simple partial seizures were recorded in 19.1% of patients living in mountainous regions and 16.54% of those living in desert regions, while complex partial seizures were observed in 19.1% of patients from mountainous areas and 18.89% of patients from desert areas.For patients with idiopathic epilepsy (IE), exclusively primary generalized seizures were characteristic. Among them, tonic-clonic seizures were recorded in 75% of patients from mountainous regions and 77.8% of patients from desert regions; absence seizures were observed in 12.5% of patients from mountainous regions and 11.1% from desert regions; myoclonic seizures were noted in 12.5% of patients from mountainous regions and 11.1% from desert regions.In the analysis of the neurological status, among the 197 examined patients, motor symptoms, cognitive and behavioral disorders were observed in 161 patients (81.7%). In patients living in mountainous regions, these indicators were more frequently detected—88.5% (46 patients) compared to 79.3% (115 patients), respectively; in 36 patients (18.3%) out of the total number of patients, the neurological status showed no remarkable features.In the study of the motor function of the upper and lower limbs, a decrease in muscle tone of the hypotonic type was observed in 2.17% of patients from mountainous regions, whereas in patients from desert regions this indicator was detected twice as often, amounting to 4.35% (p < 0.05).Coordination disorders, characterized by unsteadiness in the Romberg position and intention tremor during the finger-to-nose test, were observed in 17.4% of examined patients from mountainous regions and 15.6% of patients from desert regions, with no statistically significant differences. Pathological reflexes were observed in 1 patient (2.17%) from mountainous regions and in 2.61% (3 patients) from desert regions in the form of the Babinski reflex.In the assessment of higher cortical functions, cognitive dysfunction was noted in 37% of cases (17 patients) from mountainous regions and 35.6% (41 patients) from desert regions, which also did not reach statistical significance. Thus, patients with epilepsy were characterized by microfocal changes such as pyramidal insufficiency and transient coordination disorders.Thus, the obtained results indicate the role of climatic factors in the development of epilepsy and its severity. In particular, in patients living in mountainous regions, epilepsy developed 1.3 times more often following stroke (CVA), and meteorological factors were involved three times more often, which emphasizes the more adverse impact of elevated atmospheric conditions and mountainous environments on the development of epilepsy.The severity of disturbances in the brain’s bioelectrical activity was assessed according to the classification proposed by E.A. Zhirmunskaya and V.S. Losev (1984). The evaluation was carried out using a six-point scale reflecting a continuum from “ideal normality” (0 points) to “very severe disturbances” (6 points). As can be seen from the data obtained, in patients with symptomatic epilepsy (SE) living in mountainous regions, the severity of disturbances in brain bioelectrical activity was more pronounced, with an average score of 3.8±0.14 points, which is 1.3 times higher than in patients with SE living in desert regions and 2.6 times higher than in patients with idiopathic epilepsy (IE) living in desert regions (p < 0.01). The overall mean score among all examined patients was 2.96±0.11 points. It should be noted that in patients living in mountainous regions, disturbances in brain bioelectrical activity were more pronounced compared to patients living in desert areas.Electroencephalography was performed in all patients with symptomatic and idiopathic epilepsy depending on climatic conditions of residence. Epileptiform activity on EEG was detected in 36 (85.7%) patients with symptomatic epilepsy (SE) and in 3 (37.5%) patients with idiopathic epilepsy (IE) from mountainous regions, as well as in 104 (81.9%) patients with SE and in 3 (33.3%) patients with IE from mountainous regions, respectively (p < 0.05). It should be noted that epileptiform activity was observed more frequently in patients from mountainous regions compared to those from desert areas; however, the differences were not statistically significant.Video-EEG monitoring (VEEGM) performed in patients in whom epileptiform activity could not be recorded on routine EEG made it possible to detect pathological epileptiform phenomena in 100% of cases.In addition to epileptiform activity, other EEG parameters during the interictal period were analyzed. In particular, visual EEG analysis revealed various diffuse changes in electrical activity, such as the absence of a regular dominant rhythm with the presence of polymorphic and polyrhythmic activity instead; disruption of the normal organization of the EEG manifested as asymmetry of an irregular and non-persistent character; disturbances in the normal topographic distribution of the main EEG rhythms and their amplitude relationships; and diffuse pathological oscillations. Involvement of deep brain structures was identified, the most typical sign of which was generalized bilaterally synchronous delta and theta waves occurring either continuously or periodically in the form of bursts. In some cases, involvement of midline brain structures manifested as bilaterally synchronous generalized bursts of high-amplitude alpha waves (above 100–120 µV) or beta oscillations with amplitudes exceeding 30 µV.We performed an analysis of zonal differences on EEG. Pronounced zonal differences were preserved in 12 (28.6%) patients with symptomatic epilepsy (SE) and in 5 (62.5%; p < 0.05) patients with idiopathic epilepsy (IE) living in mountainous regions, as well as in 39 (30.71%) patients with SE and in 5 (55.6%) patients with IE living in desert regions; they were attenuated in 16 (38.1%) patients with SE and in 2 (25%) patients with IE from mountainous regions, as well as in 46 (36.2%) patients with SE and in 3 (33%) patients from desert regions; they were distorted in 14 (33.3%) patients with SE and in 1 (12.5%; p < 0.05) patient with IE from mountainous regions, and in 42 (33.1%) patients with SE and in 1 (11.1%) patient from desert regions.Diffuse EEG changes classified as mild were observed in 8 (19.1%) patients with SE and in 5 (62.5%; p < 0.05) patients with IE living in mountainous regions, as well as in 30 (23.6%) patients with SE and in 5 (55.6%) patients with IE living in desert regions; moderate changes were seen in 16 (38.1%) patients with SE and in 2 (25%) patients with IE living in mountainous regions, as well as in 47 (37%) patients with SE and in 3 (33.3%) patients with IE in desert regions; and pronounced changes were observed in 18 (42.9%) patients with SE and in 1 (12.5%) patient with IE living in mountainous regions, as well as in 50 (39.4%) patients with SE and in 1 (11.1%) patient with IE in desert regions. All indicators showed statistically significant differences between patients from mountainous and desert regions (p < 0.05). Mild diffuse changes were most frequently observed in patients with IE living in mountainous regions, while pronounced diffuse changes were more common in patients with SE from mountainous regions, indicating a more negative impact of mountainous climatic factors on epilepsy severity.According to the organization of EEG types, four variants of background EEG were identified, reflecting their key characteristics: organized (mountain region—4 (9.52%) in SE and 3 (37.5%) in IE; desert region—14 (11%) in SE and 3 (33.3%) in IE; p < 0.01), disorganized (mountain region—8 (19.1%) in SE and 3 (37.5%) in IE; desert region—23 (18.1%) in SE and 4 (44.4%) in IE; p < 0.05), hypersynchronous (mountain region—17 (40.5%) in SE and 1 (12.5%) in IE; desert region—43 (33.86%) in SE and 1 (11.1%) in IE; p < 0.01), and desynchronous (mountain region—13 (30.95%) in SE and 1 (12.5%) in IE; desert region—47 (37%) in SE and 1 (11.1%) in IE; p < 0.05). The results indicate that the hypersynchronous EEG type was most frequently observed in patients with SE living in mountainous regions, whereas the disorganized type was most common among patients living in desert regions.The most pronounced EEG changes were observed in patients with symptomatic epilepsy associated with cerebrovascular pathology and the consequences of traumatic brain injury.Thus, routine electroencephalographic examination performed in the interictal period revealed epileptiform activity in 36 (85.7%) patients with SE and in 3 (37.5%) patients with IE from mountainous regions, as well as in 104 (81.9%) patients with SE and in 3 (33.3%) patients with IE from mountainous regions, respectively (p < 0.05). It should be emphasized that epileptiform activity was more frequently observed in patients from mountainous regions compared to those from desert areas; however, the differences were not statistically significant.Neurophysiological analysis showed that diffuse changes in brain bioelectrical activity were mainly of moderate severity. The most pronounced EEG changes were observed in patients with cerebrovascular pathology and consequences of traumatic brain injury from mountainous regions. These were characterized by a disorganized EEG, absence of alpha rhythm, predominance of slow waves of varying amplitude, as well as the possible negative influence of reduced atmospheric pressure in mountainous areas, geo-electromagnetic waves, electron-charged air, and other environmental climatic factors.Cognitive impairment in epilepsy is one of the most important components of the clinical picture of the disease, significantly affecting patients’ quality of life and social adaptation. Various factors play an important role in the pathogenesis of these disorders, including organic damage to brain structures, neuronal dysfunction, interictal epileptic activity, recurrent seizures, as well as the use of certain antiepileptic drugs (AEDs), which may lead to seizure aggravation [8,13].The study of cognitive impairment was conducted in all patients with epilepsy (n = 197). The control group consisted of 30 practically healthy individuals matched for age and sex. At the initial examination, patients’ complaints were analyzed. It was noted that 100% of patients reported seizures (Figure 2). Among nonspecific complaints, memory impairment ranked first; it was recorded 5.5% more often in Group I patients living in mountainous regions compared to Group II patients living in desert regions (Group I—88.2%; Group II—82.7% (p < 0.05)). Fatigue ranked second, being reported 2.6% more often in Group II patients (Group I—83.3%; Group II—85.9% (p < 0.05)). Headache ranked third and was reported 11.1% more often in Group I patients, which was statistically significant and is most likely associated with the negative effect of reduced atmospheric pressure in mountainous regions (by 7%, p = 0.65).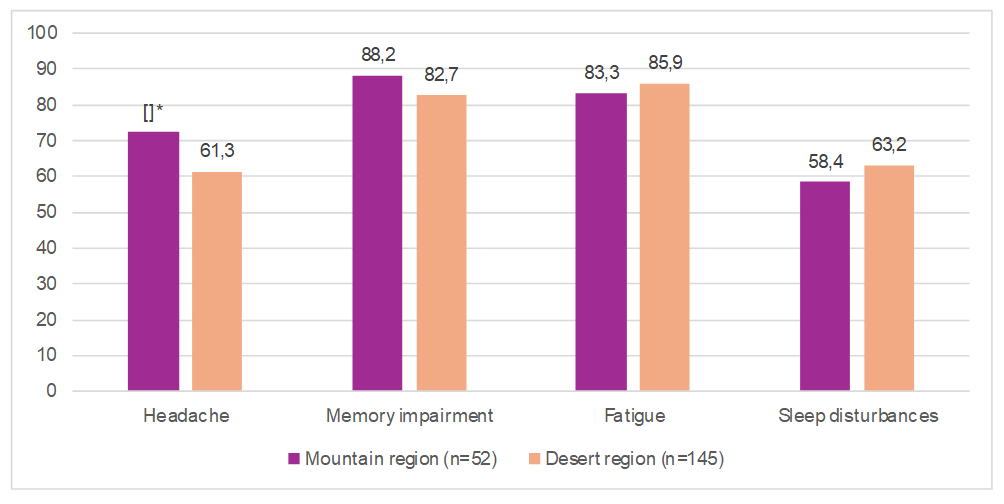 | Figure 2. Complaints of patients with epilepsy depending on climatic conditions of residence |
The analysis of the results of the Montreal Cognitive Assessment (MoCA) scale showed that the severity of cognitive impairment, based on the total score, in patients with epilepsy differed depending on climatic conditions of residence as well as the form of epilepsy.According to the results of the Montreal Cognitive Assessment (MoCA), the mean test score in patients with symptomatic epilepsy (SE) living in mountainous regions was 18.1±1.5 points, which was 34.7% lower than in the control group, where the score was 27.7±3.1 points, indicating impaired cognitive functioning. In patients with idiopathic epilepsy (IE) living in mountainous regions, the score was 21.75±1.8 points, which was 21.5% lower than in the control group, indicating mild to moderate cognitive impairment.In the analysis of patients living in desert regions, it was determined that in patients with SE residing in desert areas, the mean MoCA score was 20.7±1.8 points, corresponding to a moderate degree of cognitive impairment and being 25.3% lower than in the control group. In patients with IE living in desert regions, this value was 23.7 points, which was 14.4% lower than in the control group.Thus, the lowest results were observed in patients with frequent generalized seizures and symptomatic epilepsy living in mountainous regions, accompanied by more pronounced cognitive impairment, most likely due to underlying organic brain disorders and the negative influence of mountainous climatic conditions. In contrast, patients with idiopathic epilepsy living in desert regions demonstrated relatively satisfactory results, which is associated with less frequent focal seizures and a lesser impact of adverse climatic conditions.In patients with SE, especially those living in mountainous regions, a marked reduction in the number of recalled words was recorded, along with a more pronounced deficit of attention during mental arithmetic and backward counting. In patients with frequent epileptic seizures and long disease duration, abstract thinking was severely impaired, and moderate dementia was detected.Clinically, cognitive impairments in patients were mainly manifested by reduced memory and attention concentration, difficulties in generalization, abstraction and forecasting, slowed thinking, and difficulties in perceiving and understanding new material. In most patients, partial disorientation in time was noted, more often in individuals with SE. These disorders frequently served as a cause of social maladaptation. The analysis of the MMSE test results showed that the mean total score in both groups was significantly lower compared to the control group. In the analysis of the MMSE test data interpretation depending on the severity of cognitive impairment, it was found that mild and moderate cognitive disorders predominated in most cases. However, in patients with symptomatic epilepsy (SE) living in mountainous regions, a moderate course was more frequently observed, whereas in patients from desert regions the severity of cognitive impairment was less pronounced. Specifically, the level of cognitive impairment in patients with SE from mountainous regions was 17.6% lower than in the control group; in patients with idiopathic epilepsy (IE) from mountainous regions, this indicator was 14.23% lower. At the same time, in patients with SE from desert regions, the level of cognitive impairment was 14.9% lower than in the control group. The closest to normal results were observed in patients with IE living in desert regions, whose indicators were 11.53% lower compared to the control group.Based on the obtained results, we concluded that symptomatic epilepsy is associated with more pronounced cognitive impairments. This is likely due to the higher frequency of epileptic seizures, longer disease duration, and consequently prolonged use of antiepileptic drugs (AEDs), which was confirmed by correlation analysis. In addition, when comparing SE in patients from mountainous and desert regions, we found that patients from mountainous regions had a more severe course of the disease with more pronounced cognitive impairments.Based on the analysis of the results of scales assessing the level of cognitive impairment, it was noted that the most pronounced deviations from normal values were observed in patients with frequent generalized seizures and symptomatic epilepsy living in mountainous regions. This condition was accompanied by more severe cognitive impairments, most likely due to organic brain damage and the negative influence of mountainous climatic conditions. In contrast, patients with idiopathic epilepsy living in desert regions demonstrated relatively satisfactory results, which is associated with less frequent focal seizures and a lesser impact of adverse climatic conditions.The results of our study showed that cognitive disorders, along with seizure activity itself, are among the leading clinical symptoms in various forms of epilepsy.
4. Discussion
The obtained results demonstrate that the course of epilepsy is significantly influenced by climatic and geographic living conditions. Patients residing in mountainous regions exhibited a more severe disease course, characterized by a higher frequency of seizures, more pronounced neurological deficits, and greater cognitive impairment compared to patients living in desert areas. These findings suggest that environmental and atmospheric factors, including reduced barometric pressure, hypoxic conditions, and geo-electromagnetic influences, may contribute to the aggravation of epileptic activity.The predominance of symptomatic epilepsy in the studied cohort is consistent with current literature, where structural brain lesions such as cerebrovascular disorders and traumatic brain injury are considered leading etiological factors. In patients from mountainous regions, a higher proportion of epilepsy cases developed following cerebrovascular events, which may reflect both vascular vulnerability and environmental stressors associated with altitude.Electroencephalographic findings further support the more severe functional state of the brain in patients from mountainous regions. More frequent epileptiform activity, pronounced diffuse changes, and disorganization of background rhythms indicate greater involvement of cortical and subcortical structures. The higher prevalence of hypersynchronous EEG patterns in these patients may reflect increased neuronal excitability and impaired regulatory mechanisms.Cognitive impairment, as assessed by MoCA and MMSE scales, was more pronounced in patients with symptomatic epilepsy, particularly those living in mountainous areas. This may be explained by the combined effect of structural brain damage, recurrent seizures, prolonged disease duration, and the influence of antiepileptic therapy. The observed correlation between disease severity and cognitive decline highlights the importance of early diagnosis and comprehensive management.Additionally, a reduced liquor-cranial index was associated with more severe clinical manifestations and cognitive deficits, suggesting that alterations in cerebrospinal fluid dynamics may play a role in the pathophysiology of epilepsy and its progression.Overall, the findings emphasize the multifactorial nature of epilepsy and highlight the significant role of climatic and geographic factors in modulating disease expression. These results underline the need for a personalized approach to diagnosis, treatment, and rehabilitation, taking into account environmental conditions, structural brain changes, and neurophysiological parameters.
5. Conclusions
1. The course of epilepsy depends on climatic and geographic conditions: in patients living in mountainous regions, the disease is more severe, with more frequent seizures and pronounced neurological symptoms. 2. The predominant form is symptomatic epilepsy, with the main causes being traumatic brain injury and cerebrovascular pathology. 3. Patients living in mountainous regions demonstrate more pronounced EEG changes and a higher level of cognitive impairment. 4. A decrease in the cerebrospinal (liquor-cranial) index is associated with a more severe course of epilepsy and cognitive deficits. 5. Consideration of climatic factors is necessary for the individualization of treatment and rehabilitation of patients.
ACKNOWLEDGEMENTS
The authors express their sincere gratitude to the staff of the Department of Neurology at Tashkent State Medical University for their valuable assistance in organizing the study, recruiting patients, and collecting clinical data. We are especially grateful to all patients who participated in this research for their cooperation and trust. We also acknowledge the contribution of the specialists who provided technical support in performing the necessary diagnostic procedures.
DISCLOSURE
The authors declare that they have no competing interests, financial or personal, that could have appeared to influence the work reported in this paper.
References
| [1] | World Health Organization (WHO). Epilepsy: Fact sheet. 2024. Available at: https://www.who.int/news-room/fact-sheets/detail/epilepsy. |
| [2] | Fisher R.S., Acevedo C., Arzimanoglou A. et al. ILAE Official Report: A practical clinical definition of epilepsy. Epilepsia. 2014; 55(4): 475–482. |
| [3] | Thijs R.D., Surges R., O’Brien T.J., Sander J.W. Epilepsy in adults. Lancet. 2019; 393(10172): 689–701. |
| [4] | Beghi E. The epidemiology of epilepsy. Neuroepidemiology. 2020; 54(2): 185–191. |
| [5] | Hauser W.A., Annegers J.F., Kurland L.T. Incidence of epilepsy and unprovoked seizures in Rochester, Minnesota: 1935–1984. Epilepsia. 1993; 34(3): 453–468. |
| [6] | Kwan P., Brodie M.J. Early identification of refractory epilepsy. N Engl J Med. 2000; 342(5): 314–319. |
| [7] | Helmstaedter C., Elger C.E. Cognitive consequences of epilepsy surgery. Lancet Neurol. 2009; 8(6): 543–553. |
| [8] | Dodrill C.B. Neuropsychological effects of seizures. Epilepsy Behav. 2004; 5(Suppl 1): S21–S24. |
| [9] | Hermann B.P., Seidenberg M. Epilepsy and cognition. Epilepsy Curr. 2007; 7(1): 1–6. |
| [10] | Baxendale S., Thompson P.J. Beyond localization: the role of traditional neuropsychological tests in an age of imaging. Epilepsia. 2010; 51(11): 2180–2188. |
| [11] | Devinsky O., Vezzani A., O’Brien T.J., Jette N., Scheffer I.E., de Curtis M., Perucca P. Epilepsy. Nat Rev Dis Primers. 2018; 4: 18024. |
| [12] | Institute of Medicine (US). Epilepsy Across the Spectrum: Promoting Health and Understanding. Washington, DC: National Academies Press; 2012. |
| [13] | Löscher W., Schmidt D. Modern antiepileptic drug development has failed to deliver: ways out of the current dilemma. Epilepsia. 2011; 52(4): 657–678. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML