-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(5): 2467-2471
doi:10.5923/j.ajmms.20261605.45
Received: Feb. 15, 2026; Accepted: Mar. 20, 2026; Published: May 19, 2026

Immunological Determinants of Myocardial Remodeling in Children After Transcatheter Closure of Ventricular Septal Defect
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAlisher D. Yusubov1, Bakhtiyorjon Y. Umarov2, Guzal U. Mullabaeva3
1Head of the Cardiology Department, Cardiologist, National Children’s Medical Center
2Director, Doctor of Medical Sciences (DSc), National Children’s Medical Center
3Doctor of Medical Sciences, Senior Researcher, National Children’s Medical Center
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Ventricular septal defect (VSD) is one of the most common congenital heart diseases in children, accounting for up to 20–25% of all congenital heart defects. Despite the widespread introduction of transcatheter VSD closure (TC-VSD), a significant proportion of pediatric patients develop adverse myocardial remodeling (AMR) during the post-interventional period, which largely determines long-term functional outcomes. The aim of this study was to investigate immunological mechanisms associated with myocardial remodeling in children after TC-VSD and to assess their prognostic significance. A prospective clinical study included 180 children who underwent TC-VSD closure. Based on long-term echocardiographic and functional outcomes, patients were divided into groups with favorable myocardial remodeling (n = 103) and adverse myocardial remodeling (n = 77). Comprehensive assessment of cardio-hemodynamic parameters, markers of innate, adaptive, and humoral immunity, as well as biochemical markers of myocardial injury was performed in the early and late post-interventional periods. Adverse myocardial remodeling was associated with a significant decrease in the CD4+/CD8+ ratio, increased natural killer cell activity, cytokine imbalance characterized by elevated IL-6 and reduced IL-10 levels, overexpression of TLR4 and TGF-β1, and persistently increased NT-proBNP concentrations. Based on multivariate analysis, an integrated immunological prognostic score (IPREM) was developed, demonstrating high sensitivity and specificity in predicting adverse remodeling. The obtained results confirm the pivotal role of immune dysregulation in post-interventional myocardial remodeling and support the clinical implementation of immuno-cardiological prognostic models in pediatric cardiology.
Keywords: Ventricular septal defect, Transcatheter closure, Myocardial remodeling, Children, Immunological predictors, Cytokines, IPREM score
Cite this paper: Alisher D. Yusubov, Bakhtiyorjon Y. Umarov, Guzal U. Mullabaeva, Immunological Determinants of Myocardial Remodeling in Children After Transcatheter Closure of Ventricular Septal Defect, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2467-2471. doi: 10.5923/j.ajmms.20261605.45.
1. Relevance of the Study
- Congenital heart diseases remain one of the leading causes of morbidity, disability, and long-term cardiovascular complications in the pediatric population worldwide [2]. Among them, ventricular septal defect (VSD) represents the most common anatomical variant, accounting for approximately 20–25% of all congenital heart defects. Advances in pediatric cardiology and interventional technologies have significantly improved survival rates and early clinical outcomes. In particular, transcatheter closure of VSD has become a widely accepted alternative to open surgical repair due to its minimally invasive nature, reduced perioperative trauma, shorter hospital stay, and lower immediate complication rates [1,2]. However, growing clinical evidence indicates that anatomical correction of the defect does not invariably result in complete normalization of myocardial structure and function. Long-term follow-up studies demonstrate that a considerable proportion of children—ranging from 18% to 35%—develop adverse myocardial remodeling after technically successful transcatheter VSD closure [7]. This condition is characterized by persistent ventricular dilation, impaired myocardial deformation, diastolic dysfunction, and a higher risk of arrhythmias and chronic heart failure in later life. Importantly, these pathological changes often remain subclinical for extended periods, escaping detection by conventional echocardiographic parameters such as left ventricular ejection fraction. As a result, myocardial remodeling may progress silently, ultimately affecting functional capacity and quality of life during adolescence and adulthood [10]. Traditionally, myocardial remodeling after congenital defect correction has been attributed primarily to hemodynamic factors, including chronic volume overload, altered pressure gradients, and delayed timing of intervention. While these mechanisms undoubtedly play an important role, recent research has shifted attention toward immunological and inflammatory pathways as critical determinants of post-interventional myocardial outcomes. Persistent activation of innate immune responses, imbalance between pro- and anti-inflammatory cytokines, dysregulation of adaptive immunity, and activation of profibrotic signaling cascades have been increasingly implicated in the development of myocardial fibrosis and functional impairment [9]. Experimental and clinical studies suggest that elevated levels of proinflammatory cytokines such as interleukin-6 and tumor necrosis factor-alpha, combined with insufficient anti-inflammatory regulation mediated by interleukin-10, promote chronic low-grade inflammation within the myocardium. In parallel, activation of Toll-like receptor pathways and increased expression of transforming growth factor-beta 1 contribute to extracellular matrix remodeling and myocardial fibrosis. These immune-mediated processes may persist even after elimination of intracardiac shunting, thereby explaining why adverse remodeling can develop despite favorable immediate procedural results [4,10]. Despite accumulating evidence regarding the immunological basis of myocardial remodeling, existing clinical studies are often limited by small sample sizes, short follow-up periods, and fragmented assessment of immune parameters. Most available prognostic models rely almost exclusively on echocardiographic or biochemical markers and fail to incorporate immunological determinants. Consequently, early identification of children at high risk for adverse myocardial remodeling remains challenging, and opportunities for timely preventive interventions are frequently missed [5,6].In this context, the relevance of the present study lies in its comprehensive and integrative approach to evaluating myocardial remodeling after transcatheter VSD closure. By combining detailed cardio-hemodynamic assessment with systematic analysis of innate, adaptive, and humoral immune parameters, this research addresses a critical gap in pediatric cardiology. The development of an immunologically informed prognostic framework offers a novel strategy for early risk stratification, personalized follow-up, and optimization of long-term outcomes in children with ventricular septal defect [7].Aim of the study The aim of this study was to identify immunological mechanisms associated with myocardial remodeling in children after transcatheter closure of ventricular septal defect and to determine their prognostic value. The study sought to evaluate the dynamic changes of innate, adaptive, and humoral immune parameters in relation to cardio-hemodynamic outcomes and to develop an integrated immunological model for early prediction of adverse myocardial remodeling in the post-interventional period.
2. Materials and Methods
- A prospective observational cohort study was conducted between 2022 and 2025 at the National Children’s Medical Center. The study included children diagnosed with hemodynamically significant ventricular septal defect (VSD) who underwent transcatheter closure. The study protocol was approved by the institutional ethics committee, and written informed consent was obtained from parents or legal guardians of all participants prior to enrollment. The final study cohort consisted of 180 children aged between 2 and 14 years (mean age 6.8 ± 2.4 years), including 96 boys (53.3%) and 84 girls (46.7%). All patients underwent standardized transcatheter VSD closure using nitinol occluder devices under fluoroscopic and echocardiographic guidance. Procedural success was defined as complete defect closure without significant residual shunt or major procedural complications. Clinical follow-up examinations were performed at 1, 6, and 12 months after the intervention. Echocardiographic assessment was performed using a Vivid E95 ultrasound system (GE Healthcare). Cardiac structural and functional parameters included left ventricular ejection fraction (LVEF), left ventricular end-diastolic volume index (LVEDVi), global longitudinal strain (GLS) obtained by speckle-tracking echocardiography, and diastolic function assessed by the E/e′ ratio. Adverse myocardial remodeling was defined as the presence of at least two of the following criteria at 12-month follow-up: LVEDVi above the age-adjusted 95th percentile, GLS values less negative than −18%, or evidence of diastolic dysfunction (E/e′ > 14). Peripheral venous blood samples were collected before the intervention, at 1 month, and at 12 months post-procedure. Immunological evaluation included flow-cytometric quantification of lymphocyte subsets (CD4+, CD8+, CD4/CD8 ratio, and natural killer cells CD16+56+). Serum cytokine concentrations (IL-6, IL-10, TNF-α, and TGF-β1) were measured using enzyme-linked immunosorbent assay (ELISA). Additional markers of innate immune activation included TLR4, HLA-DR, and soluble CD14. Humoral immune parameters included immunoglobulin A (IgA) and secretory IgA. Biochemical markers of myocardial stress included N-terminal pro-brain natriuretic peptide (NT-proBNP) and cardiac troponin I. Potential confounding variables were also collected and included defect size, pre-intervention shunt magnitude (Qp/Qs ratio), age at intervention, type of occluder device, presence of residual shunt, and peri-procedural inflammatory responses. These variables were incorporated into the multivariate statistical models to adjust for possible confounding effects.Sample size calculation was performed before the initiation of the study based on expected differences in cytokine levels between remodeling groups reported in previous pediatric cardiology studies. Assuming a statistical power of 80% and a significance level of α = 0.05, a minimum sample size of 150 patients was required to detect clinically meaningful differences. The final cohort of 180 patients therefore provided adequate statistical power. Statistical analysis was performed using SPSS software version 26. Continuous variables were expressed as mean ± standard deviation and compared using Student’s t-test or the Mann–Whitney U test depending on distribution normality. Categorical variables were analyzed using the chi-square test. Multivariate logistic regression analysis was applied to identify independent predictors of adverse myocardial remodeling. To avoid potential circular reasoning, echocardiographic parameters used for defining remodeling were excluded from the primary immunological prediction model. Receiver operating characteristic (ROC) curve analysis was used to assess predictive performance of the model, and calibration was evaluated using the Hosmer–Lemeshow goodness-of-fit test. A p-value < 0.05 was considered statistically significant.
|
3. Results
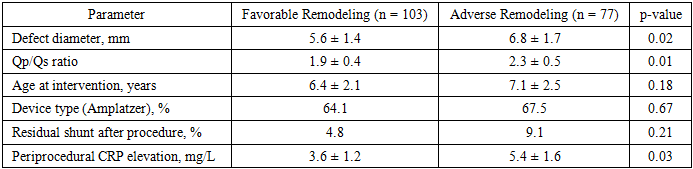
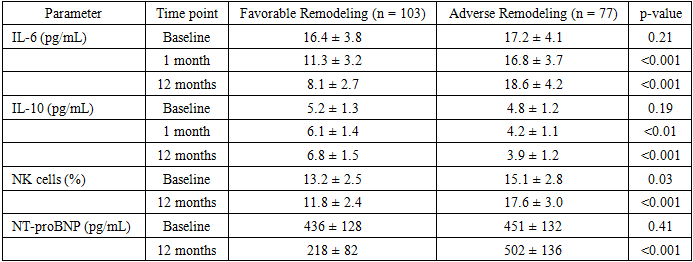
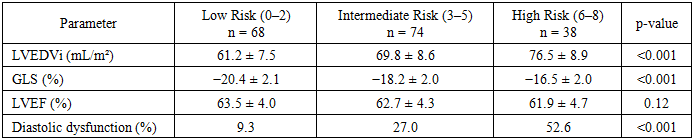
- A total of 180 children who underwent successful transcatheter closure of ventricular septal defect completed the 12-month follow-up and were included in the final analysis. Favorable myocardial remodeling was observed in 103 patients (57.2%), whereas 77 children (42.8%) developed adverse myocardial remodeling according to predefined echocardiographic criteria.Baseline demographic characteristics, including age, sex distribution, and procedural parameters, were comparable between groups (p > 0.05). However, children who subsequently developed adverse remodeling demonstrated significantly greater hemodynamic burden before intervention. The mean defect diameter was larger in the adverse remodeling group (6.8 ± 1.7 mm vs 5.6 ± 1.4 mm, p = 0.02), and the Qp/Qs ratio indicating left-to-right shunt magnitude was also significantly higher (2.3 ± 0.5 vs 1.9 ± 0.4, p = 0.01). Mild residual shunt after device implantation was observed in 9.1% of patients with adverse remodeling compared with 4.8% in the favorable remodeling group, although this difference did not reach statistical significance (p = 0.21).Echocardiographic assessment at 12 months revealed clear structural and functional differences between groups. Children with adverse remodeling demonstrated significantly higher left ventricular end-diastolic volume index (74.8 ± 9.6 mL/m² vs 62.4 ± 8.1 mL/m², p < 0.001) and less negative global longitudinal strain values (−16.9 ± 2.1% vs −20.1 ± 2.2%, p < 0.001), indicating persistent subclinical myocardial dysfunction. In contrast, left ventricular ejection fraction remained within normal limits in both groups (63.2 ± 4.1% vs 61.8 ± 4.6%, p = 0.09). Diastolic dysfunction defined by E/e′ > 14 was identified in 44.2% of patients with adverse remodeling compared with 12.6% in the favorable remodeling group (p < 0.001).Significant differences were also observed in immunological parameters. Patients with adverse myocardial remodeling exhibited a markedly reduced CD4+/CD8+ ratio (1.11 ± 0.22 vs 1.46 ± 0.25, p < 0.001). A CD4/CD8 ratio below 1.2 was present in 68.8% of children in the adverse remodeling group compared with 19.4% in those with favorable outcomes (p < 0.001). The proportion of natural killer cells was also significantly increased in the adverse remodeling group (17.6 ± 3.0% vs 11.8 ± 2.4%, p < 0.01), indicating persistent activation of innate immune responses.Cytokine analysis revealed a pronounced pro-inflammatory imbalance. Interleukin-6 concentrations were more than twofold higher in the adverse remodeling group (18.6 ± 4.2 pg/mL vs 8.1 ± 2.7 pg/mL, p < 0.001), whereas anti-inflammatory interleukin-10 levels were significantly reduced (3.9 ± 1.2 pg/mL vs 6.8 ± 1.5 pg/mL, p < 0.01). Consequently, the IL-6/IL-10 ratio exceeded 3.5 in 72.7% of patients with adverse remodeling compared with 21.4% of patients with favorable myocardial recovery (p < 0.001). Additionally, profibrotic cytokine TGF-β1 levels were significantly elevated in the adverse remodeling group (12.4 ± 2.1 ng/mL vs 7.9 ± 1.8 ng/mL, p < 0.01).Multivariate logistic regression analysis adjusted for potential confounders (defect size, Qp/Qs ratio, age at intervention, device type, and residual shunt) identified several independent immunological predictors of adverse myocardial remodeling. A CD4/CD8 ratio below 1.2 was associated with a 3.62-fold increased risk (95% CI: 2.01–6.54, p < 0.001). NK cell proportion greater than 15% increased the risk by 2.88 times (95% CI: 1.63–5.09, p < 0.01). The strongest association was observed for an IL-6/IL-10 ratio greater than 3.5 (OR = 4.14; 95% CI: 2.29–7.48; p < 0.001). Elevated TGF-β1 concentrations (>10 ng/mL) and NT-proBNP levels (>400 pg/mL) were also significant predictors (OR = 3.41 and OR = 3.79, respectively).Based on these predictors, an integrated immunological prognostic score (IPREM) was developed. The score ranged from 0 to 8 points and demonstrated good discriminative ability. Receiver operating characteristic analysis showed an area under the curve (AUC) of 0.87 (95% CI: 0.81–0.92), indicating high predictive performance. The model sensitivity was 86% and specificity 82%. Calibration analysis using the Hosmer–Lemeshow goodness-of-fit test demonstrated satisfactory agreement between predicted and observed outcomes (p = 0.41).Risk stratification according to the IPREM score demonstrated a clear gradient of adverse remodeling probability. Patients classified as low risk (0–2 points) had a predicted risk of approximately 9%, whereas intermediate-risk patients (3–5 points) demonstrated a probability of 37%. Children classified as high risk (6–8 points) had a markedly increased probability of adverse myocardial remodeling, reaching 74%.
|
|
4. Conclusions
- The results of the present study demonstrate that adverse myocardial remodeling after transcatheter closure of ventricular septal defect occurs in a substantial proportion of pediatric patients despite technically successful defect correction. In the studied cohort, unfavorable myocardial remodeling was observed in 42.8% of children during the 12-month follow-up period. Importantly, conventional echocardiographic parameters such as left ventricular ejection fraction remained within normal limits in most patients, indicating that early myocardial dysfunction may remain subclinical and undetected by routine assessment. The findings highlight a strong association between immune dysregulation and the development of myocardial remodeling after transcatheter VSD closure. Children with adverse remodeling demonstrated significant alterations in both adaptive and innate immune responses, including reduced CD4/CD8 ratios, increased natural killer cell activity, pro-inflammatory cytokine imbalance characterized by elevated IL-6 and reduced IL-10 levels, as well as increased concentrations of profibrotic cytokine TGF-β1 and persistently elevated NT-proBNP levels. Based on these predictors, an integrated immunological prognostic model (IPREM score) was developed, demonstrating good predictive performance for identifying patients at increased risk of adverse myocardial remodeling. The model showed high diagnostic accuracy with an AUC of 0.87, sensitivity of 86%, and specificity of 82%.Although the observational design of the study does not allow causal inference, the results suggest that immunological mechanisms may play an important role in myocardial recovery following structural correction of congenital heart defects. Further multicenter studies and external validation of the proposed model are required to confirm its clinical applicability and to improve long-term risk stratification in pediatric patients after transcatheter VSD closure.