-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(5): 2461-2466
doi:10.5923/j.ajmms.20261605.44
Received: Dec. 14, 2025; Accepted: Jan. 10, 2026; Published: May 19, 2026

Laparoscopic Versus Open Surgery for Acute Gynecological Abdomen: A Retrospective–Prospective Clinical Study
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKhudoyarova Dildora Rakhimovna1, Tursunov Nuriddin Bakhriddinovich2
1DSc, Professor, Samarkand State Medical University, Samarkand, Uzbekistan
2Obstetrician-Gynecologist, Samarkand Branch of the Republican Scientific and Practical Center for Emergency Medical Care, Samarkand, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Acute gynecological abdomen represents a group of urgent clinical conditions that require rapid diagnosis and timely surgical intervention. These emergencies include ectopic pregnancy, ovarian torsion, ovarian apoplexy, and ruptured ovarian cysts, which may lead to intra-abdominal bleeding and severe complications if not treated promptly. The objective of this study was to evaluate surgical outcomes in women with acute gynecological abdomen and to optimize management strategies through the use of minimally invasive laparoscopic techniques. A retrospective–prospective clinical study was conducted involving 100 women aged 18–45 years who were admitted with symptoms of acute gynecological abdomen. The patients were divided into two groups: 50 women underwent laparoscopic surgery and 50 women were treated using open surgical access. All patients underwent standardized diagnostic evaluation including clinical examination, ultrasound imaging, Doppler blood flow assessment, laboratory investigations, and additional imaging when required. Surgical outcomes, intraoperative blood loss, postoperative complications, and reproductive outcomes were analyzed. The results demonstrated that laparoscopic surgery was associated with significantly lower complication rates compared with open surgery (5% versus 18%). In addition, laparoscopic procedures resulted in reduced intraoperative blood loss (approximately 350 milliliters versus 750 milliliters) and shorter hospital stay (4 days versus 7–9 days). Preservation of reproductive potential was higher in the laparoscopic group (89%) compared with the open surgery group (72%). In conclusion, laparoscopic management represents a safe and effective surgical approach for acute gynecological abdomen and contributes to improved clinical outcomes and better preservation of reproductive function.
Keywords: Acute Abdomen, Laparoscopy, Gynecologic Surgical Procedures, Ovarian Torsion, Ectopic Pregnancy, Hemostasis
Cite this paper: Khudoyarova Dildora Rakhimovna, Tursunov Nuriddin Bakhriddinovich, Laparoscopic Versus Open Surgery for Acute Gynecological Abdomen: A Retrospective–Prospective Clinical Study, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2461-2466. doi: 10.5923/j.ajmms.20261605.44.
1. Introduction
- Acute gynecological abdomen represents a group of urgent pathological conditions that require rapid diagnosis and timely surgical intervention. These conditions include ectopic pregnancy, ovarian torsion, ovarian apoplexy, ruptured ovarian cysts, and other gynecological emergencies that may lead to significant intra-abdominal bleeding and life-threatening complications if not treated promptly. Acute gynecologic emergencies account for a substantial proportion of hospital admissions in emergency gynecological practice and remain an important cause of reproductive morbidity among women of reproductive age [5,9,11].Historically, laparotomy has been the standard surgical approach for the management of acute gynecologic abdomen. However, with the rapid development of minimally invasive surgical technologies, laparoscopy has become increasingly recognized as a safer and less traumatic alternative in emergency gynecology. Numerous studies demonstrate that laparoscopic surgery provides improved visualization of pelvic structures, reduced surgical trauma, lower postoperative pain, shorter hospitalization, and faster recovery compared with conventional open surgery [1–4].Despite these advantages, the choice between laparoscopic and open surgical approaches in emergency gynecology remains controversial in certain clinical situations, particularly in cases complicated by hemoperitoneum, hemodynamic instability, or unclear diagnosis. In many healthcare systems, including developing regions, laparotomy continues to be widely used due to limitations in equipment availability, surgeon experience, or lack of standardized clinical protocols [3,11].Accurate and timely diagnosis of gynecological causes of acute abdomen is crucial for determining the optimal surgical strategy. Modern diagnostic approaches include transabdominal and transvaginal ultrasound, Doppler blood flow assessment, and additional imaging techniques, when necessary, which significantly improve diagnostic accuracy and facilitate early surgical intervention [6,12].Therefore, comparative clinical evaluation of laparoscopic and open surgical approaches in patients with acute gynecological abdomen remains highly relevant. Understanding the differences in surgical outcomes, intraoperative blood loss, postoperative complications, and reproductive prognosis can help optimize surgical decision-making and improve overall patient management. Recent regional studies have also highlighted the importance of improving surgical tactics and rehabilitation strategies to enhance long-term reproductive outcomes in women undergoing emergency gynecological surgery [7,10].The present study was designed as a retrospective–prospective clinical investigation comparing laparoscopic and open surgical treatment in women with acute gynecological abdomen. The aim of the study was to evaluate clinical outcomes of the two surgical approaches, analyze the effectiveness of different haemostasis methods used during surgery, and assess postoperative rehabilitation strategies in order to optimize the management of acute gynecologic emergencies.
2. Materials and Methods
- This research was designed as a mixed retrospective–prospective clinical study carried out at the Samarkand branch of the Republican Scientific and Practical Center for Emergency Medical Care. This institution functions as the primary regional referral facility for gynecologic emergencies, providing round-the-clock diagnostic and surgical care for women presenting with acute abdominal symptoms. The center is equipped with modern ultrasound systems, Doppler technologies, laparoscopic equipment of various generations, and comprehensive laboratory diagnostic capabilities, which together allow for prompt and highly accurate evaluation of emergency gynecologic conditions.The retrospective component of the study included the analysis of medical records, operative reports, and postoperative outcomes of previously treated patients, while the prospective phase consisted of direct clinical assessment, surgical management, and postoperative follow-up of newly admitted women with acute abdominal presentations. This combined design ensured both the depth of historical clinical data and the precision of real-time observation under standardized protocols.A total of 100 women, aged 18 to 45 years, were included in the study according to predefined diagnostic and eligibility criteria. All participants were evaluated either at the moment of emergency admission or during the review of historical clinical documentation.Patients were included if they demonstrated:Acute abdominal pain or symptoms suggestive of a gynecologic emergency.The need for urgent diagnostic clarification or surgical intervention, as determined by the attending gynecologist.Patients were excluded if they had: Chronic pelvic diseases requiring elective (non-urgent) surgical treatment. A history of abdominal or pelvic surgery within the preceding three months, which could distort clinical presentation or postoperative outcomes.To ensure balanced comparison, all eligible patients were divided into two equal groups of 50 women each: Laparoscopy Group (n = 50): Women treated using minimally invasive laparoscopic techniques. Laparotomy Group (n = 50): Women operated via traditional open surgical access due to clinical indications such as suspected massive intra-abdominal bleeding, large pelvic masses, or lack of visualization during minimally invasive attempts.The equal numerical distribution of patients across the two groups made it possible to perform a reliable comparative analysis of surgical outcomes, postoperative recovery, and complication rates.All patients underwent a standardized diagnostic protocol upon admission.The diagnostic evaluation included clinical examination, assessment of medical and reproductive history, abdominal and transvaginal ultrasound examination, Doppler blood flow assessment of pelvic organs, laboratory tests including complete blood count and coagulation profile, and measurement of serum beta-human chorionic gonadotropin levels when ectopic pregnancy was suspected.In selected cases with unclear clinical presentation, additional imaging methods such as computed tomography were used to improve diagnostic accuracy. Surgical treatment was performed according to the clinical condition of the patient and the diagnostic findings. Laparoscopic procedures were performed using standard minimally invasive techniques with three or four trocars. Hemostasis during laparoscopic surgery was achieved using monopolar coagulation, bipolar coagulation, or laser energy depending on intraoperative conditions. In patients with extensive hemoperitoneum, unstable hemodynamic status, or technical limitations for minimally invasive surgery, open laparotomy was performed.The study protocol was reviewed and approved by the Ethics Committee of Samarkand State Medical University, Samarkand, Uzbekistan (Approval No. SSMU-2026/118, issued on March 15, 2026). The study was conducted in accordance with the ethical principles of the Declaration of Helsinki and international standards for biomedical research involving human subjects.All participants were informed about the objectives and procedures of the study prior to participation. Written informed consent was obtained from all patients before diagnostic evaluation and surgical intervention. Participation in the study was voluntary, and patients had the right to withdraw from the study at any stage without affecting their medical care. Confidentiality and anonymity of all patient data were strictly maintained. Personal identifiers were removed from the database and all clinical information was used solely for scientific and research purposes.Statistical analysis was performed using Statistical Package for the Social Sciences software (version 26.0). Quantitative variables were expressed as mean values with standard deviation. Comparisons between groups were performed using the student t-test for continuous variables and the x-square test for categorical variables. A probability value of less than 0.05 was considered statistically significant.
3. Results
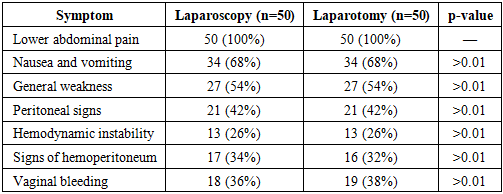
- A total of 100 women aged 18 to 45 years were included in the study, with a mean age of 33.4 ± 2.2 years. All patients presented with symptoms typical of acute gynecological abdomen, most frequently acute pelvic pain, followed by nausea, vomiting, vaginal bleeding, and signs of hemodynamic instability in cases complicated by intra-abdominal hemorrhage. Many patients reported sudden onset of pain during physical activity or at rest, and approximately one-third demonstrated signs suggestive of hemoperitoneum on initial ultrasound evaluation. This group of patients required rapid differential diagnosis to distinguish gynecologic emergencies from other acute abdominal conditions.Both groups were comparable in terms of age, symptom duration (table-1), parity, and baseline clinical characteristics, which allowed for reliable comparative assessment of surgical outcomes of underlying causes demonstrated that acute gynecologic emergencies were primarily represented by ovarian apoplexy, torsion of ovarian cysts, and ectopic pregnancy. These conditions frequently resulted in intra-abdominal bleeding, making diagnosis more challenging. A total of 38 cases of ovarian apoplexy were identified across the broader dataset used for comparative evaluation. Within the study cohort of 100 patients, ovarian apoplexy comprised the largest subgroup.
|
4. Discussion
- The present study demonstrated that laparoscopic management of acute gynecological abdomen is associated with significantly better clinical outcomes compared with open surgical intervention. Patients treated with minimally invasive techniques experienced lower rates of postoperative complications, reduced intraoperative blood loss, shorter hospitalization, and faster functional recovery. These findings support the growing role of laparoscopy as a preferred surgical approach in emergency gynecologic practice and are consistent with previously reported data emphasizing the advantages of minimally invasive surgery in urgent gynecological conditions [1–4].Acute gynecological abdomen remains one of the most challenging clinical scenarios in emergency gynecology, requiring rapid diagnosis and prompt surgical management. Previous studies have shown that minimally invasive techniques provide improved visualization of pelvic structures, reduced tissue trauma, and faster postoperative recovery compared with conventional laparotomy [3,11]. Our findings further confirm that laparoscopy can be safely applied even in complex clinical situations, including cases accompanied by hemoperitoneum or uncertain diagnostic presentation. In such conditions, laparoscopy serves both as a diagnostic and therapeutic modality, allowing precise identification of pathology and immediate surgical treatment.One of the key findings of the present study is the significant reduction in postoperative complications among patients treated with laparoscopic surgery. The lower complication rate observed in the laparoscopic group reflects the advantages of minimal tissue manipulation, improved visualization of anatomical structures, and more precise surgical control. These results are consistent with previous reports indicating that laparoscopic surgery in acute gynecological pathology significantly reduces surgical trauma, postoperative pain, and the duration of hospitalization [4,11].Another important aspect of this study is the analysis of haemostatic techniques used during surgery. The findings indicate that bipolar coagulation provides more effective and controlled hemostasis compared with monopolar and laser coagulation. Bipolar coagulation allows precise energy delivery and minimizes lateral thermal damage to surrounding tissues, which is particularly important in reproductive-age women where preservation of ovarian reserve is a key objective. Similar observations have been reported in previous studies emphasizing the safety and effectiveness of bipolar coagulation in minimally invasive gynecologic surgery [2,3].Postoperative rehabilitation also plays a critical role in determining long-term outcomes following emergency gynecological surgery. Our results demonstrate that early mobilization, physiotherapy, and structured rehabilitation strategies contribute to faster recovery and reduce the incidence of postoperative complications such as chronic pelvic pain, adhesions, and secondary endometriosis. These findings are supported by recent studies highlighting the importance of comprehensive postoperative rehabilitation in improving quality of life and reproductive outcomes after gynecological surgery [7,10].Preservation of reproductive function represents another important outcome of surgical management in women of reproductive age. In our study, patients treated with laparoscopic surgery demonstrated significantly higher rates of fertility preservation compared with those who underwent open surgery. This difference can be explained by the reduced invasiveness of laparoscopic techniques, decreased tissue trauma, and improved anatomical restoration of pelvic organs. Previous research has also indicated that minimally invasive surgical approaches contribute to better reproductive outcomes and lower rates of postoperative adhesions [1,10].Despite these encouraging findings, several limitations of the present study should be acknowledged. First, the study was conducted at a single clinical center, which may limit the generalizability of the results. Second, the sample size was relatively limited, which may influence the statistical power of the analysis. Third, long-term follow-up of reproductive outcomes was not available for all patients included in the study. Future multicenter studies with larger patient populations and longer follow-up periods are necessary to further validate the advantages of laparoscopic surgery in the management of acute gynecological abdomen.Overall, the findings of this study reinforce the growing body of evidence supporting minimally invasive surgery as the preferred approach for the treatment of acute gynecological abdomen. Implementation of standardized surgical techniques, optimization of hemostasis methods, and development of structured postoperative rehabilitation protocols may significantly improve patient outcomes and contribute to better preservation of reproductive health in women experiencing gynecological emergencies.
5. Conclusions
- The findings of this study convincingly demonstrate that laparoscopic interventions represent the most effective and clinically justified approach to managing acute gynecologic abdomen in reproductive-age women. Through comprehensive analysis of perioperative indicators, postoperative complications, and long-term functional outcomes, it becomes evident that minimally invasive surgery provides substantial advantages over traditional laparotomy. These advantages include reduced intraoperative blood loss, shorter operative time, lower rates of postoperative infection and adhesions, and significantly accelerated functional recovery. Collectively, these benefits translate into improved patient comfort, shorter hospital stays, and reduced healthcare burden.A central finding of this investigation is the strong positive influence of laparoscopic surgery on the preservation of reproductive potential. Given that many women presenting with acute gynecologic emergencies are of reproductive age, the ability of laparoscopy to minimize ovarian trauma, prevent unnecessary tissue excision, and reduce the inflammatory response is of critical clinical relevance. The markedly higher fertility preservation rate observed among laparoscopic patients underscores the importance of prioritizing minimally invasive approaches whenever hemodynamically feasible. This advantage carries long-term implications for women’s quality of life, family planning, and overall reproductive health.Equally important is the demonstrated superiority of bipolar coagulation as a hemostasis method. Its precision, controlled thermal spread, and tissue-sparing characteristics make it the optimal choice for managing bleeding during emergency laparoscopic procedures. Its incorporation into standard operative protocols may further decrease postoperative adhesions and reduce the likelihood of secondary endometriosis, thereby improving both short- and long-term outcomes.The study also highlights a structural gap within the current clinical practice: the absence of standardized postoperative rehabilitation algorithms. Analysis of patient recovery trajectories revealed that outcomes are significantly dependent on early, structured rehabilitation that includes physiotherapy, guided mobilization, pelvic floor therapy, and individualized counseling. Establishing unified rehabilitation standards and integrating them into national clinical guidelines would lead to more predictable recovery, fewer chronic pain syndromes, and improved reproductive function preservation.In conclusion, this study provides robust evidence supporting the prioritization of laparoscopic methods as the gold standard for managing acute gynecologic abdomen. The integration of optimal haemostasis techniques and structured rehabilitation programs is essential for maximizing the benefits of minimally invasive surgery. Implementing these findings into everyday clinical practice, along with continuous professional training of surgeons and further refinement of diagnostic methods, will significantly enhance the quality of emergency gynecologic care and contribute to improved long-term health outcomes for women in Uzbekistan and beyond.