-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(5): 2454-2460
doi:10.5923/j.ajmms.20261605.43
Received: Apr. 26, 2026; Accepted: May 13, 2026; Published: May 19, 2026

Clinicopathological Correlation of Videostroboscopic Findings in Benign Vocal Fold Lesions
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAbbasov Arif Nasibovich, Yuldasheva Ra'no Daminovna, Salimov Khusen Abdurafikovich, Shukurullayeva Dilnoz Inom qizi, Suyunova Zamira Sayfidinovna, Beknazarov Boburjon Baxodir o’g’li, Toshtemirov Sanjarbek Yusubjonovich
University of Business and Science, Tashkent, Uzbekistan
Correspondence to: Abbasov Arif Nasibovich, University of Business and Science, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Background: Benign vocal fold lesions represent the most common organic causes of dysphonia. Accurate preoperative differentiation is essential for selecting optimal surgical strategy. Objective: To evaluate videostroboscopic and clinicopathological features of benign vocal fold lesions and determine diagnostic accuracy of videostroboscopy. Methods: A prospective study included 102 patients with benign vocal fold lesions: nodules (n=34), polyps (n=40), and cysts (n=28). All patients underwent clinical examination, videolaryngoscopy, videostroboscopy, and histological evaluation. Statistical analysis included chi-square testing and diagnostic accuracy assessment. Results: Dysphonia was observed in 90.2% of patients. Mucosal hyperemia was significantly more frequent in nodules (76.5%) compared with polyps (35.0%) and cysts (28.6%) (p<0.001). Videostroboscopy revealed reduced vibratory amplitude in 72.5% of cases and mucosal wave impairment in 66.7%. Diagnostic sensitivity was 91.2% for nodules, 90.0% for polyps, and 89.3% for cysts. Overall diagnostic accuracy was 90.2%, with sensitivity ranging from 89.3% to 91.2%. Conclusion: Videostroboscopy provides reliable preoperative differentiation of benign vocal fold lesions and improves surgical planning. Combined clinicopathological assessment increases diagnostic accuracy.
Keywords: Benign laryngeal lesions, Vocal fold nodules, Vocal fold polyp, Vocal fold cyst, Videostroboscopy, Dysphonia
Cite this paper: Abbasov Arif Nasibovich, Yuldasheva Ra'no Daminovna, Salimov Khusen Abdurafikovich, Shukurullayeva Dilnoz Inom qizi, Suyunova Zamira Sayfidinovna, Beknazarov Boburjon Baxodir o’g’li, Toshtemirov Sanjarbek Yusubjonovich, Clinicopathological Correlation of Videostroboscopic Findings in Benign Vocal Fold Lesions, American Journal of Medicine and Medical Sciences, Vol. 16 No. 5, 2026, pp. 2454-2460. doi: 10.5923/j.ajmms.20261605.43.
1. Introduction
- Benign laryngeal lesions occupy a significant place in the structure of organic pathology of the vocal apparatus and upper respiratory tract. According to epidemiological studies, they account for 50–70% of all tumor and tumor-like processes of the larynx and are detected in 15–25% of patients with dysphonia in outpatient practice [1,2]. The social significance of this problem is determined by the high prevalence of voice disorders, especially among individuals engaged in voice-demanding professions [3].Benign laryngeal lesions are most frequently diagnosed in patients aged 25–55 years, corresponding to the period of highest professional activity [4]. Gender differences have been reported: vocal fold nodules are more common in women, whereas vocal fold polyps and hyperplastic lesions predominate in men [5].Vocal fold polyps account for approximately 30–40% of organic lesions of the vocal apparatus. Vocal fold nodules are more often identified in individuals with prolonged vocal load, whereas vocal fold cysts and vascular lesions occur considerably less frequently [6].The clinical and anatomical features of benign laryngeal lesions are determined by the complex anatomical and functional organization of the larynx, which performs respiratory, phonatory, and protective functions [7]. Even minor structural changes in the mucosa may significantly impair vocal fold biomechanics and phonation [3].The most vulnerable region is the area of the true vocal folds due to high vibratory load and the structural characteristics of Reinke’s space, the superficial layer of the lamina propria [8]. Nodules, polyps, and cystic lesions most commonly develop in this region.The main clinical manifestation of benign laryngeal lesions is dysphonia, presenting as hoarseness, reduced vocal intensity, and rapid vocal fatigue. In cases of large lesions, patients may also complain of throat discomfort and voice instability [9].Modern visualization techniques have significantly expanded diagnostic capabilities. Videolaryngoscopy allows determination of lesion localization and size, whereas videostroboscopy enables assessment of vocal fold vibratory function, amplitude of oscillation, symmetry, and mucosal wave characteristics [2,10].Thus, the clinical and anatomical characteristics of benign laryngeal lesions depend on their localization, morphological type, and size. Understanding these factors is essential for selecting optimal diagnostic and therapeutic strategies.
2. Materials and Methods
- Study design: prospective observational study.The study included 102 patients with benign laryngeal lesions who underwent examination and treatment at the ENT Department of the multidisciplinary clinic of Tashkent State Medical University between 2024 and 2026.The patients were divided into three clinical groups according to the morphological type of the lesion:• Group 1 consisted of 34 patients with vocal fold nodules,• Group 2 included 40 patients with vocal fold polyps,• Group 3 comprised 28 patients with vocal fold cysts.Inclusion criteria were age ≥18 years, the presence of clinically and morphologically confirmed benign laryngeal lesions (vocal fold nodules, polyps, and cysts), and characteristic clinical symptoms including dysphonia, hoarseness, and respiratory disturbances. The diagnosis was confirmed based on videolaryngoscopic findings and subsequent histological examination. Written informed consent was obtained from all patients prior to inclusion in the study. Additionally, the ability to complete the full set of diagnostic procedures according to the study protocol was required.Exclusion criteria included suspected malignant laryngeal tumors or histologically confirmed high-grade dysplasia. Patients with severe decompensated somatic diseases (cardiovascular, renal, or hepatic failure), acute infectious diseases, systemic autoimmune disorders, as well as pregnant and breastfeeding women were excluded. Patients who refused to participate or did not complete the full diagnostic evaluation were also excluded from the study.Sample size justificationThe sample size was determined based on the expected diagnostic accuracy of videostroboscopy for benign vocal fold lesions reported in previous studies, with an anticipated sensitivity of approximately 85–90%. A minimum sample of 90 patients was considered sufficient to achieve 80% statistical power at a significance level of 0.05. The final cohort included 102 patients, which was considered adequate for subgroup comparisons and diagnostic accuracy analysis. Blinding and interobserver agreementVideostroboscopic recordings were independently evaluated by two experienced otorhinolaryngologists who were blinded to the histopathological diagnosis and clinical group allocation. In cases of disagreement, the final interpretation was established by consensus review. Interobserver agreement for videostroboscopic assessment was evaluated using Cohen’s kappa coefficient. The overall agreement between observers was substantial (κ = 0.82), indicating high reproducibility of videostroboscopic interpretation.StatisticsStatistical analysis was performed using SPSS version 26.0 (IBM Corp., USA). Categorical variables were compared using the chi-square test or Fisher’s exact test where appropriate. Multivariate logistic regression analysis was performed to identify independent predictors associated with specific benign vocal fold lesions and videostroboscopic findings. Continuous variables were expressed as mean ± standard deviation. Diagnostic accuracy of videostroboscopy was assessed by calculating sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and overall accuracy. A p-value <0.05 was considered statistically significant.Ethics statementThe study was conducted in accordance with the ethical principles of the Declaration of Helsinki (2013 revision). Written informed consent was obtained from all participants prior to enrollment in the study. Patient confidentiality and anonymity were strictly maintained throughout the investigation.This study was observational in nature and based on routinely collected clinical data obtained during standard diagnostic and therapeutic procedures. No experimental interventions were performed. According to institutional regulations, formal ethics committee approval was not required for this type of study.
3. Results
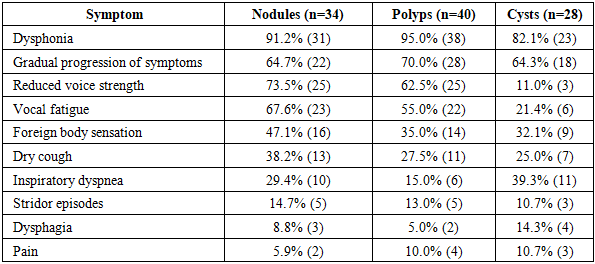
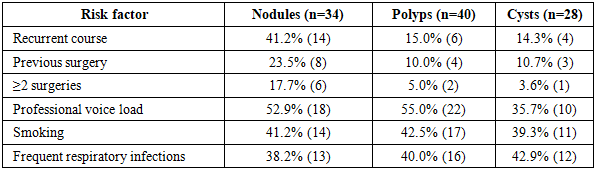
- Clinical examination was performed according to a standardized protocol and included analysis of patient complaints, medical history taking, physical examination, indirect laryngoscopy, videolaryngoscopy, and functional assessment of the vocal apparatus. The obtained data allowed for a detailed characterization of the clinical course of benign vocal fold lesions and evaluation of their impact on voice and respiratory function.A total of 102 patients with benign vocal fold lesions were included: vocal fold nodules (n=34), polyps (n=40), and cysts (n=28). Dysphonia was the most frequent symptom, observed in 90.2% of patients, with no statistically significant difference between groups (p=0.18). Inspiratory dyspnea occurred more frequently in patients with vocal fold cysts (39.3%) compared with nodules (29.4%) and polyps (15.0%) (p=0.04).Incomplete glottic closure was observed in 64.7% of nodules, 70.0% of polyps, and 71.4% of cysts (p=0.62). Mucosal hyperemia and edema were significantly more frequent in vocal fold nodules (76.5%) compared with polyps (35.0%) and cysts (28.6%) (p<0.001). Multivariate analysis identified mucosal hyperemia and professional voice load as independent predictors of vocal fold nodules (p<0.05).In contrast to vocal fold nodules, patients with vocal fold polyps and especially cysts demonstrated more pronounced voice disturbances. Vocal fold cysts were associated with significant impairment of mucosal vibratory activity, clinically manifested by marked dysphonia. Persistent hoarseness was observed in 11 (39.3%) patients. In 6 (21.4%) patients, vocal function deteriorated even with moderate voice load, while 3 (10.7%) patients presented with an intermittent, unstable voice (Table 1). These findings were associated with the subepithelial localization of cysts and pronounced impairment of the mucosal wave.
|
|
|

|
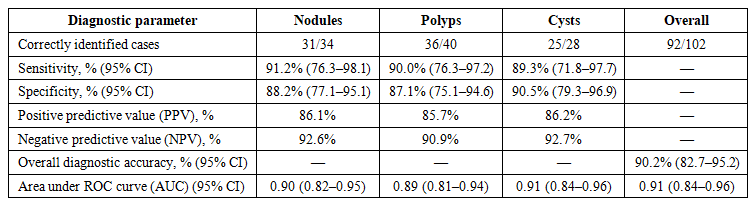 | Table 5. Diagnostic performance of videostroboscopy |
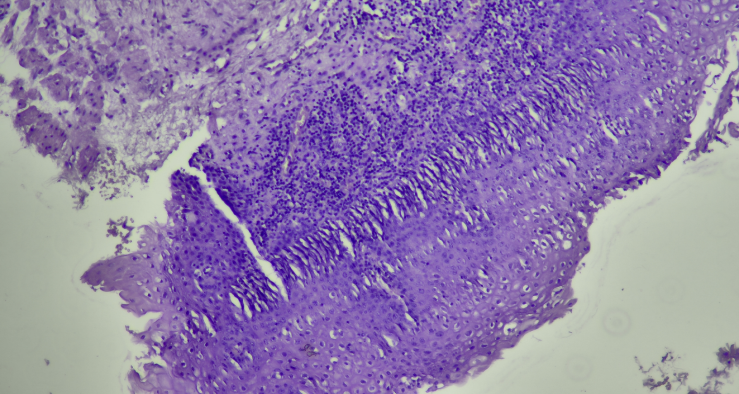 | Figure 1. Vocal fold nodules. Microscopic examination reveals pronounced epithelial hyperplasia in the stratified squamous non-keratinized epithelium. Focal areas of parakeratosis are observed. The basement membrane is preserved. The lamina propria shows fibrotic changes of connective tissue with elements of hyalinosis. Moderate chronic inflammatory infiltration is present, predominantly composed of lymphocytes and plasma cells. Blood vessels are dilated. No cellular atypia is identified. Magnification ×100. Staining: hematoxylin and eosin (H&E) |
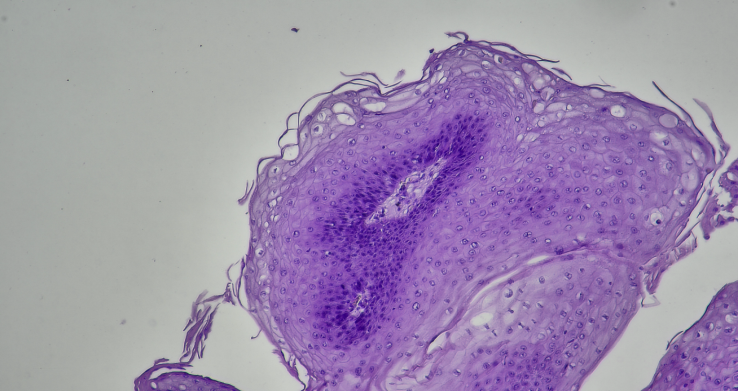 | Figure 2. Vocal fold polyp. Histologically, the lesion is covered by stratified squamous epithelium with dystrophic changes and desquamation. The stroma demonstrates edema and loose connective tissue. Moderate inflammatory infiltration of predominantly lymphohistiocytic character is observed. Myxoid (mucoid) stromal edema is also present. No signs of malignant growth are identified. Magnification ×100. Staining: hematoxylin and eosin (H&E) |
 | Figure 3. Vocal fold cyst. Microscopic examination reveals a cystic cavity within the stratified squamous epithelium. The cavity is lined by single-layer cuboidal epithelium, with focal metaplasia into stratified squamous epithelium. The cyst lumen contains serous or mucous material. The cyst wall is composed of fibrous connective tissue with moderate lymphocytic infiltration. The surrounding tissues show signs of chronic inflammation and vascular reactions. No atypical cells are identified. Magnification ×100. Staining: hematoxylin and eosin (H&E) |
4. Discussion
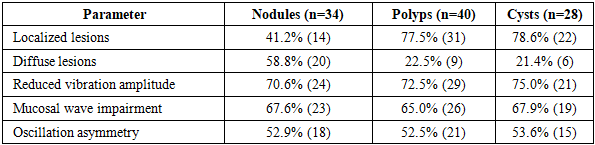
- The obtained results demonstrate that benign vocal fold lesions are characterized by different clinical and functional patterns determined by the morphological type of the lesion and the depth of involvement of the vibratory layer of the mucosa. Dysphonia of varying severity was the most common symptom across all study groups, which is consistent with current understanding of the leading role of organic vocal fold pathology in voice disorders. The severity of dysphonia depended on lesion localization, size, and the degree of involvement of the superficial layer of the lamina propria.The identified differences in clinical course confirm the morphofunctional specificity of each type of benign lesion. Vocal fold nodules were characterized by bilateral symmetric involvement and predominantly functional voice disturbances. Videolaryngoscopy revealed small symmetric thickenings at the junction of the anterior and middle thirds of the vocal folds, accompanied by mild mucosal hyperemia. Videostroboscopy demonstrated reduced vibratory amplitude with partial preservation of the mucosal wave, indicating superficial involvement and predominantly fibrous-hyperplastic changes in the lamina propria. These findings reflect chronic microtrauma of the vocal folds associated with prolonged voice load.Vocal fold polyps demonstrated predominantly unilateral involvement and more pronounced voice disturbances. Endoscopic examination revealed localized exophytic lesions of various shapes with mucosal hyperemia and edema. Videostroboscopic evaluation showed asymmetry of vocal fold vibration, reduced vibratory amplitude, and localized impairment of the mucosal wave. These changes are explained by the vascular-exudative nature of the process, marked stromal edema, and reduced elasticity of the superficial lamina propria. In contrast to nodules, polyps were associated with more pronounced mechanical stiffness of the affected vocal fold and asymmetric vibration.Vocal fold cysts exhibited a different clinical and functional pattern. This group was characterized by more severe impairment of vibratory function due to the subepithelial localization of the lesion. Videolaryngoscopy demonstrated well-defined rounded submucosal lesions with relatively preserved epithelial covering. Videostroboscopy revealed marked reduction in vibratory amplitude and focal absence of the mucosal wave on the affected side. These changes are explained by restricted mucosal mobility and impaired gliding of the superficial lamina propria. The laryngeal framework remained preserved, distinguishing cysts from deeper submucosal lesions.Despite a similar frequency of mucosal wave impairment (65–68%) across all groups, differential diagnosis was based not on a single parameter but on a combination of features, including lesion distribution pattern, degree of vocal fold rigidity, asymmetry of vibration, and depth of involvement of the vibratory layer. Thus, functional analysis of vocal fold vibration allows assessment of morphofunctional changes, significantly expanding diagnostic capabilities compared with conventional indirect laryngoscopy.The obtained data confirm the need for a comprehensive approach to preoperative diagnosis of benign vocal fold lesions. The use of videostroboscopy as a mandatory step in evaluation allows objective assessment of morphofunctional changes and improves diagnostic accuracy. From a practical standpoint, this approach facilitates more precise determination of the extent of surgical intervention and reduces the risk of damage to the vibratory layer of the mucosa.For vocal fold nodules, an organ-preserving microsurgical approach with maximal preservation of the superficial lamina propria is preferred. For vocal fold polyps, microsurgical removal with preservation of vibratory properties of the vocal fold and minimal trauma to surrounding tissues is recommended. For vocal fold cysts, surgical management requires careful dissection due to the subepithelial location and the need to preserve the structure of the vibratory layer.
5. Conclusions
- Benign vocal fold lesions demonstrate different clinical and functional characteristics depending on the morphological type and depth of involvement of the vibratory layer of the mucosa. Videostroboscopy allows identification of diagnostically significant features of vocal fold nodules (bilateral symmetric involvement and partial preservation of the mucosal wave), vocal fold polyps (unilateral lesion, asymmetric vibration, and reduced amplitude), and vocal fold cysts (subepithelial localization and focal absence of the mucosal wave). The use of videostroboscopy improves the accuracy of preoperative diagnosis and contributes to the selection of optimal surgical management.